HTN in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "pregnancy" AND "preeclampsia"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have enough comprehensive data to write a detailed, well-structured answer. Let me compile everything.
Hypertension in Pregnancy
Classification
Hypertension in pregnancy is defined as BP ≥ 140/90 mmHg. The normal physiologic trend shows a nadir at ~18-22 weeks (median 113/69 mmHg), rising back to term levels. The upper reference limit is 144/95 mmHg at term.
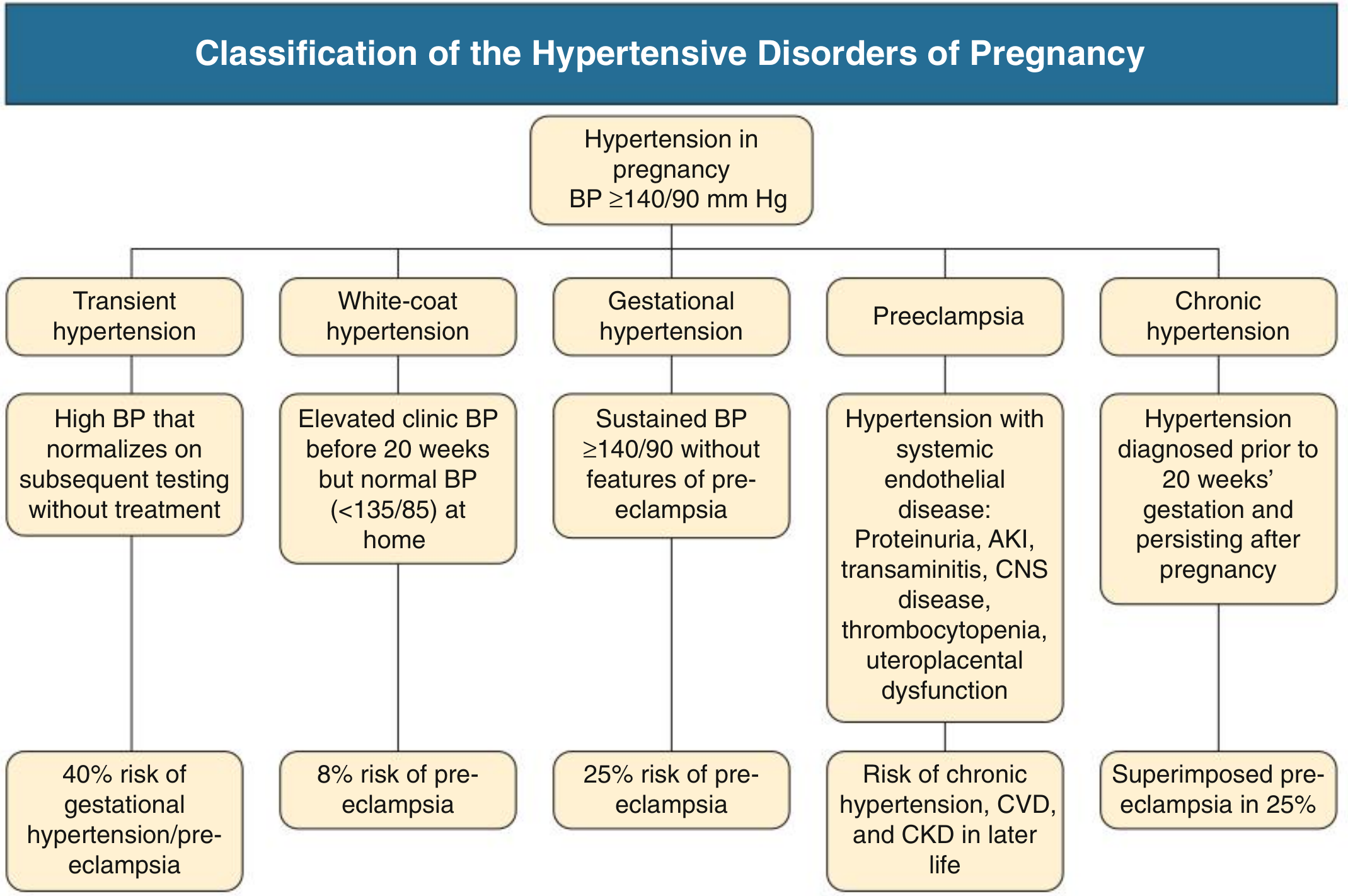
There are five main categories:
| Category | Definition | Key Risk |
|---|---|---|
| Transient HTN | BP normalizes on subsequent testing without treatment | 40% risk of gestational HTN/preeclampsia |
| White-coat HTN | Clinic BP ≥140/90 but home BP <135/85 | 8% risk of preeclampsia (double baseline) |
| Gestational HTN | New HTN after 20 weeks, no features of preeclampsia | 25% progress to preeclampsia |
| Preeclampsia | HTN after 20 weeks + maternal/uteroplacental organ dysfunction | Risk of chronic HTN, CVD, CKD later |
| Chronic HTN | BP ≥140/90 pre-pregnancy or before 20 weeks, persists >12 wks postpartum | 25% risk of superimposed preeclampsia |
- Comprehensive Clinical Nephrology, 7th Edition
Epidemiology
- HTN affects 10-12% of all pregnancies
- Global preeclampsia incidence: 4.6% of all pregnancies
- Eclampsia: 1.4% globally (lower in high-income countries - ~0.3% of hypertensive pregnancies)
- Comprehensive Clinical Nephrology, 7th Edition
Preeclampsia
Diagnostic Criteria
Preeclampsia = new hypertension after 20 weeks + any one of the following:
- Proteinuria: uPCR >30 mg/mmol or uACR >8 mg/mmol (note: proteinuria is not essential if other criteria exist)
- AKI
- Elevated transaminases (liver dysfunction)
- Neurological features (headache, visual disturbance, altered consciousness, seizures)
- Thrombocytopenia (platelets <100,000/mm³)
- Uteroplacental dysfunction: fetal growth restriction, abnormal umbilical artery Doppler, or stillbirth
Severe features include: SBP ≥160 or DBP ≥110 mmHg, pulmonary edema, thrombocytopenia, marked renal/hepatic dysfunction, and CNS manifestations.
Risk Factors
Obstetric: Nulliparity, previous preeclampsia, multiple gestation, new partner, IVF conception
Medical: Chronic HTN, CKD, pre-gestational diabetes, obesity (BMI >30), antiphospholipid syndrome, SLE, polycystic ovarian syndrome
Genetic/Other: Thrombophilia, first-degree relative with preeclampsia, age >40, born SGA
Pathogenesis

The mechanism follows a two-stage model:
-
Stage 1 - Abnormal placentation (early pregnancy): Failed trophoblastic invasion of spiral arteries. Normally, trophoblasts remodel spiral arteries into low-resistance, high-capacitance vessels. In preeclampsia, this remodeling fails, causing uteroplacental ischemia and oxidative stress in the placenta.
-
Stage 2 - Systemic maternal disease: Hypoxic placenta releases factors causing:
- Decreased circulating PlGF (placental growth factor - proangiogenic)
- Increased sFlt-1 (soluble fms-like tyrosine kinase-1 - antiangiogenic)
- Systemic endothelial dysfunction → hypertension, proteinuria, multiorgan involvement
- Comprehensive Clinical Nephrology, 7th Edition
HELLP Syndrome
HELLP = Hemolysis, Elevated Liver enzymes, Low Platelets
-
Considered a variant of severe preeclampsia, though may be a separate entity
-
Women with HELLP tend to be older, White, and multiparous compared to preeclampsia
-
Characteristic renin-angiotensin changes of preeclampsia do not occur in HELLP
-
AKI occurs in 10-25% of preeclampsia/HELLP cases (vs ~1% in preeclampsia alone)
-
Management is similar to severe preeclampsia - delivery is the definitive treatment
-
Key distinction from TTP: preceding HTN/proteinuria/liver injury favor HELLP; severe hemolysis/renal failure without liver injury favors TTP. Plasma exchange benefits TTP but not HELLP.
-
Brenner and Rector's The Kidney, 2-Volume Set; Creasy & Resnik's Maternal-Fetal Medicine
Eclampsia
- Seizures in a woman with preeclampsia that cannot be attributed to other causes
- ~20% of eclamptic episodes occur >48 hours postpartum - vigilance must continue after delivery
- Magnesium sulfate is the treatment of choice for seizure prevention and treatment (superior to phenytoin/diazepam)
Management
Treatment Thresholds
- Severe HTN (SBP ≥160 or DBP ≥105-110 mmHg): Immediate antihypertensive therapy is indicated - untreated severe HTN carries risk of maternal stroke and placental abruption
- Mild-moderate HTN (140-159/90-109 mmHg): Treat to reduce risk of progression; target BP typically 130-150/80-100 mmHg
Antihypertensive Drug Safety in Pregnancy
| Drug | Class | Notes |
|---|---|---|
| Methyldopa | Central α2-agonist | First-line; most extensive safety data; sedation, short duration |
| Labetalol (oral/IV) | α+β blocker | Preferred β-blocker; theoretical benefit on uteroplacental flow; avoid in asthma |
| Nifedipine (long-acting) | CCB | Once-daily dosing; may cause edema |
| Nicardipine (IV) | CCB | Extensive data as tocolytic; effective for acute control |
| Hydralazine (IV/IM) | Direct vasodilator | Second-line acute; risk of maternal hypotension and placental abruption |
| Metoprolol | β-blocker | Less safety data than labetalol |
| Verapamil/Diltiazem | CCB | Limited data; no known adverse fetal effects |
| Diuretics | - | Generally avoided - may impair plasma volume expansion |
| Atenolol | β-blocker | Avoid - associated with fetal growth restriction |
| Nitroprusside | Vasodilator | Avoid if >4 hours - fetal cyanide poisoning risk |
| ACE inhibitors | RAAS | Contraindicated - fetal renal agenesis, oligohydramnios, skull defects |
| ARBs | RAAS | Contraindicated - same risks as ACEi |
- Brenner and Rector's The Kidney; Goodman & Gilman's Pharmacological Basis of Therapeutics
Acute Severe HTN Protocol
- Labetalol IV: 20 mg IV, escalate to 40 mg at 10 min if inadequate
- Hydralazine IV/IM: 5-10 mg, repeat at 20-min intervals
- Add magnesium sulfate for CNS manifestations or severe preeclampsia (seizure prophylaxis)
Definitive Treatment
Delivery is the only cure for preeclampsia. If severe preeclampsia with end-organ damage and a mature fetus - deliver promptly. If very preterm, temporizing with hospitalization and pharmacotherapy may allow further fetal maturation.
Prevention
Low-dose aspirin (75-150 mg/day) initiated before 16 weeks in high-risk women reduces preeclampsia incidence. Meta-analyses support its use; a Cochrane review confirms benefit. Some guidelines (e.g., USPSTF) recommend universal aspirin for moderate-high risk women. Long-term follow-up data on children exposed to low-dose aspirin in utero are reassuring.
- Brenner and Rector's The Kidney; NKF Primer on Kidney Diseases, 8e
Calcium supplementation (in populations with low calcium intake) also reduces BP disorders of pregnancy.
Secondary Causes of HTN in Pregnancy
At least 10% of chronic HTN in pregnancy has a secondary cause. Screen for:
- Renal artery stenosis (fibromuscular dysplasia) - suspect with severe resistant HTN; MR angiography is safe
- Pheochromocytoma - catastrophic if missed; can trigger fatal crisis during labor
- Primary hyperaldosteronism - may worsen in pregnancy (progesterone partially antagonizes aldosterone but not universally); spironolactone has theoretical risks (antiandrogenic) - eplerenone preferred if needed
- Obstructive sleep apnea - 40% of women with HTN in pregnancy may have OSA
Long-term Implications
Women who have had preeclampsia carry significantly elevated long-term risks of:
- Chronic hypertension
- Cardiovascular disease
- Chronic kidney disease
These women warrant cardiovascular risk factor surveillance postpartum.
Recent evidence (2025): A network meta-analysis in AJOG (PMID 40216176) compared oral antihypertensives in pregnancy and may update relative preferences among labetalol, nifedipine, and methyldopa - worth reviewing if making clinical decisions.
This is a shared conversation. Sign in to Orris to start your own chat.