Tell me everything about acynotic heart disease and cyanotic heart disease in detail in paediatrics
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need for a comprehensive, detailed answer. Let me compile it all together.
Congenital Heart Disease in Paediatrics: Acyanotic and Cyanotic
Congenital heart disease (CHD) affects approximately 8 per 1,000 live births and is the most common category of birth defects. It is broadly divided into acyanotic (no central cyanosis at rest) and cyanotic (central cyanosis present) lesions. The dividing principle is whether deoxygenated blood reaches the systemic circulation.
Screening: Pulse oximetry before nursery discharge (ideally >24 hours of life) is standard. The result is positive if SpO2 <90% in any limb, SpO2 <95% in both extremities on three readings 1 hour apart, or a >3% absolute difference between right hand and foot on three readings.
Classification Overview (Pulmonary Blood Flow)
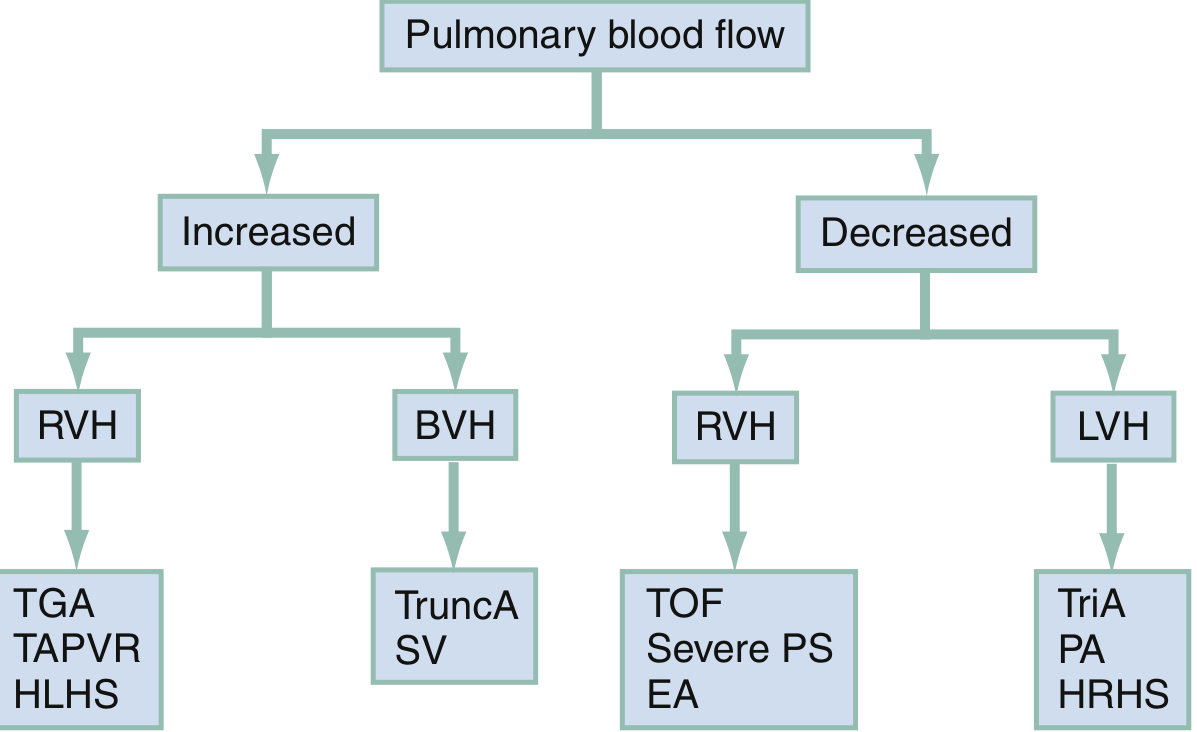
The flowchart above from Rosen's Emergency Medicine organises cyanotic lesions by pulmonary blood flow direction (increased vs. decreased) and dominant ECG finding (RVH, BVH, LVH) - a powerful diagnostic tool at the bedside.
Hyperoxia (Oxygen Challenge) Test
Used to distinguish cardiac from pulmonary cyanosis. The infant breathes FiO2 = 1.0 for ≥10 minutes and an ABG is repeated.
| Condition | PaO2 at FiO2 0.21 | PaO2 at FiO2 1.0 | PaCO2 |
|---|---|---|---|
| Normal | 70 mmHg (95%) | >200 mmHg (100%) | 35 |
| Pulmonary disease | 50 mmHg (85%) | >150 mmHg (100%) | 50 |
| Neurologic disease | 50 mmHg (85%) | >150 mmHg (100%) | 50 |
| Methemoglobinemia | 70 mmHg (85%) | >200 mmHg (85%) | 35 |
| Cardiac (separate circulations - D-TGA with intact VS) | <40 mmHg (<75%) | <50 mmHg (<85%) | 35 |
| Cardiac (restricted PBF - TOF, tricuspid atresia, pulm. atresia) | <40 mmHg (<75%) | <50 mmHg (<85%) | 35 |
| Cardiac (complete mixing - truncus, TAPVR, single ventricle) | 50 mmHg (85%) | <150 mmHg (<100%) | 35 |
Note: Hyperoxia test is now less commonly performed due to known adverse effects of hyperoxaemia and alkalosis.
- The Harriet Lane Handbook, p. 241
Syndromes Associated with CHD
| Syndrome | Common Cardiac Defect |
|---|---|
| CHARGE | TOF, truncus arteriosus, aortic arch anomalies |
| Down syndrome (Trisomy 21) | AVSD, VSD, ASD |
| Turner syndrome (45,XO) | Coarctation of aorta, bicuspid aortic valve |
| Williams syndrome | Supravalvular aortic stenosis, peripheral PS |
| Noonan syndrome | Pulmonary stenosis, HCM |
| DiGeorge syndrome (22q11) | Conotruncal defects (TOF, truncus, interrupted aortic arch) |
| Marfan syndrome | Aortic root dilation, MR |
PART 1: ACYANOTIC CONGENITAL HEART DISEASE
Acyanotic CHD falls into two mechanistic groups:
- Left-to-right shunts - increase pulmonary blood flow (VSD, ASD, PDA, AVSD)
- Obstructive lesions - no shunting at rest (PS, AS, CoA)
1. Ventricular Septal Defect (VSD)
Most common CHD overall (~30-40% of all CHD).
Pathophysiology: Left-to-right shunting at the ventricular level. Shunt magnitude depends on the defect size and pulmonary vascular resistance (PVR). Small VSDs may close spontaneously; large, unrestrictive VSDs cause left ventricular volume overload and may lead to pulmonary hypertension and eventually Eisenmenger syndrome.
Clinical Presentation (from Harriet Lane Handbook, p. 243):
- Murmur: 2-5/6 holosystolic or early systolic murmur, loudest at the lower left sternal border (LLSB), ± systolic thrill
- Large shunts produce an apical diastolic rumble (from increased mitral flow)
- With large VSD + pulmonary hypertension: S2 may become narrow/single
- Symptoms: Presents from 4 weeks onward with heart failure (poor feeding, tachypnoea, diaphoresis)
ECG:
- Small VSD: Normal
- Medium VSD: LVH ± left atrial enlargement (LAE)
- Large VSD: Biventricular hypertrophy (BVH) ± LAE; pure RVH if Eisenmenger develops
CXR: Cardiomegaly with increased pulmonary vascular markings (PVMs) if hemodynamically significant
Management:
- Small muscular VSDs: Observe - high rate of spontaneous closure
- Large VSDs with heart failure: Medical stabilisation (diuretics, ACE inhibitors), surgical or catheter-based closure
- Goal: Close before irreversible pulmonary hypertension develops (ideally before 6-12 months)
2. Atrial Septal Defect (ASD)
Pathophysiology: Left-to-right shunting at the atrial level. Less acute than VSD because right and left atrial pressures are similar. Four types: Ostium secundum (most common, 70%), ostium primum (associated with Down syndrome), sinus venosus, and coronary sinus.
Clinical Presentation (Harriet Lane Handbook, p. 243):
- Murmur: Grade 2-3/6 systolic ejection murmur at the upper left sternal border (LUSB)
- Hallmark: Wide, fixed split S2 (fixed because atrial pressures equilibrate throughout the respiratory cycle)
- May have a mid-diastolic rumble at LLSB (tricuspid flow murmur)
- Usually asymptomatic in childhood; symptoms emerge in adulthood if untreated
ECG:
- Small ASD: Normal
- Large ASD: Right axis deviation (RAD), mild RVH, or RBBB with RSR' in V1
CXR: Cardiomegaly with increased PVMs if hemodynamically significant
Management:
- Ostium secundum: Catheter-based closure (Amplatzer device) for defects ≥5 mm with haemodynamic significance
- Ostium primum and sinus venosus: Surgical closure
- Goal: Closure before school age to prevent long-term atrial arrhythmias and pulmonary hypertension
3. Patent Ductus Arteriosus (PDA)
Incidence: 40-60% of very low birth weight (VLBW) infants.
Pathophysiology: Persistence of the fetal ductus arteriosus connecting the main pulmonary artery to the descending aorta. Left-to-right shunting from aorta to pulmonary circulation causes pulmonary overcirculation and left ventricular volume overload.
Clinical Presentation (Harriet Lane Handbook, p. 243):
- Murmur: 1-4/6 continuous "machinery" murmur, loudest at the upper left sternal border (LUSB)
- Wide pulse pressure (bounding pulses) - from diastolic run-off into pulmonary circulation
- Signs of heart failure in large PDAs
ECG:
- Small-moderate PDA: Normal or LVH
- Large PDA: BVH
CXR: Cardiomegaly with increased PVMs proportional to shunt size
Management:
- Premature infants: Indomethacin or ibuprofen (COX inhibitors to promote closure); surgical ligation if medical management fails
- Term infants/children: Catheter-based closure (coil or Amplatzer duct occluder)
- Spontaneous closure is uncommon after 3 months in term infants
4. Atrioventricular Septal Defect (AVSD) / Endocardial Cushion Defect
Strong association with Down syndrome (Trisomy 21).
Pathophysiology: Defect in the endocardial cushions results in primum ASD + inlet VSD + common atrioventricular valve (rather than separate mitral and tricuspid valves). Causes massive shunting at both atrial and ventricular levels + AV valve regurgitation.
Clinical Presentation (Harriet Lane Handbook, p. 243):
- Hyperactive precordium with systolic thrill at LLSB
- Loud S1 ± grade 3-4/6 holosystolic regurgitant murmur along LLSB
- ± Systolic murmur of mitral regurgitation (MR) at apex
- ± Mid-diastolic rumble at LLSB or apex ± gallop rhythm
ECG:
- Pathognomonic: Superior QRS axis (left axis deviation)
- RVH and LVH may be present
CXR: Cardiomegaly with increased PVMs
Management:
- Surgical repair at 3-6 months of age (before irreversible pulmonary hypertension)
- Partial AVSD (primum ASD only): Surgical patch closure
5. Pulmonary Stenosis (PS)
Obstructive lesion - no shunt. Most commonly valvular.
Clinical Presentation (Harriet Lane Handbook, p. 243):
- Ejection click at LUSB (valvular PS); the click decreases with inspiration and increases with expiration (opposite of aortic click)
- S2 may be widely split with diminished P2
- Systolic ejection murmur (SEM) 2-5/6 ± thrill at LUSB, radiating to back and sides
ECG:
- Mild PS: Normal
- Moderate PS: RAD and RVH
- Severe PS: Right atrial enlargement (RAE) and RVH with strain
CXR: Normal heart size with normal to decreased PVMs (post-stenotic dilation of the main pulmonary artery)
Management:
- Mild PS (gradient <40 mmHg): Observe
- Moderate-severe PS (gradient >40 mmHg): Balloon pulmonary valvuloplasty (first line)
- Dysplastic valves: Surgical valvotomy
6. Aortic Stenosis (AS)
Obstructive lesion. Valvular (most common), subvalvular, or supravalvular.
Clinical Presentation (Harriet Lane Handbook, p. 243-244):
- Ejection click that does NOT vary with respiration (valvular AS)
- Harsh SEM 2-4/6 at the 2nd right intercostal space (RICS) or 3rd left ICS, radiating to neck and apex
- Systolic thrill at RUSB, suprasternal notch, or over carotids
- ± Early diastolic decrescendo murmur (aortic regurgitation)
- Narrow pulse pressure if severe stenosis
- Critical AS in neonates: presents with shock (duct-dependent systemic circulation)
ECG:
- Mild AS: Normal
- Moderate-severe AS: LVH ± strain pattern
CXR: Usually normal; may show post-stenotic dilation of aorta
Management:
- Critical neonatal AS: Prostaglandin E1 (PGE1) infusion to maintain ductal patency, then balloon valvuloplasty or surgical valvotomy
- Older children: Balloon valvuloplasty (valvular) or surgical resection (subvalvular membrane)
7. Coarctation of the Aorta (CoA)
Male:female ratio of 2:1. Association with Turner syndrome and bicuspid aortic valve.
Clinical Presentation (Harriet Lane Handbook, p. 243-244):
- Key finding: Blood pressure differential between upper and lower limbs (higher in arms); diminished or delayed femoral pulses
- 2-3/6 SEM at LUSB ± thrill, murmur may radiate to interscapular area
- Neonates with critical CoA present with shock (duct-dependent systemic circulation) as the ductus closes
- Older children may be asymptomatic, discovered incidentally by hypertension or murmur
Presentation timeline: From first week of life onward (Rosen's Emergency Medicine)
ECG:
- Neonates: RVH (normal finding in neonates)
- Older children: LVH
CXR:
- Neonates: Cardiomegaly
- Older children: "3 sign" on the aortic knuckle (indentation at coarctation site); rib notching (from intercostal collaterals) - appears after age 5-6 years
Management:
- Critical neonatal CoA: PGE1 infusion, surgical repair (extended end-to-end anastomosis)
- Older children: Balloon angioplasty ± stenting or surgical repair
PART 2: CYANOTIC CONGENITAL HEART DISEASE
Cyanotic CHD results from either decreased pulmonary blood flow (right-to-left shunting bypasses the lungs) or right-to-left mixing of deoxygenated blood directly into the systemic circulation.
The "5 T's" of Cyanotic CHD (Rosen's Emergency Medicine, p. 3209):
- Tetralogy of Fallot
- Transposition of the Great Arteries (TGA)
- Tricuspid Atresia
- TAPVR (Total Anomalous Pulmonary Venous Return)
- Truncus Arteriosus
Additional: Ebstein anomaly, pulmonary atresia, hypoplastic left heart syndrome (HLHS), hypoplastic right heart syndrome (HRHS), single ventricle.
Key bedside clue: "Comfortably blue" (central cyanosis with minimal respiratory distress) strongly suggests cardiac rather than pulmonary aetiology. Cyanosis worsening with crying also points to cardiac disease.
Classic CXR silhouettes:
- Boot-shaped heart (coeur en sabot): Tetralogy of Fallot
- Egg on a string: Transposition of the great arteries
- Snowman/figure-of-eight heart: Total anomalous pulmonary venous return (TAPVR)
1. Tetralogy of Fallot (TOF)
Most common cyanotic CHD beyond infancy.
Four Components (Harriet Lane Handbook, p. 245; Rosen's, p. 3209):
- Large, unrestrictive, misaligned VSD
- Right ventricular outflow tract (RVOT) obstruction (infundibular and/or valvular pulmonary stenosis)
- Overriding aorta (straddles the VSD, receives blood from both ventricles)
- Right ventricular hypertrophy (RVH) - secondary to RVOT obstruction
Embryology: Single defect - failure of the subpulmonic conus to expand causes all four anomalies. Associated anomalies: right-sided aortic arch (25%), ASD ("pentalogy"), anomalous coronary artery origin.
Pathophysiology: RVOT obstruction forces deoxygenated RV blood across the VSD into the aorta. The degree of cyanosis is directly proportional to the degree of RVOT obstruction. "Pink tet" = mild RVOT obstruction with net left-to-right shunt (acyanotic at rest).
Clinical Features (Harriet Lane Handbook, p. 245; Rosen's, p. 3209-3210):
- Murmur: Loud systolic ejection murmur at LMSB and LUSB ± thrill; a loud, single S2 (aortic closure only)
- Cyanosis worsening with crying and feeding (infants); physical exertion (older children)
- Chronic hypoxaemia leads to polycythaemia and digital clubbing (fingers and toes)
- Presentation: Birth to 12 weeks (Rosen's table)
ECG: RAD and RVH
CXR: Boot-shaped heart with normal heart size ± decreased pulmonary vascular markings
TOF - Hypercyanotic ("Tet") Spells
Peak incidence: 2-4 months of age.
Pathophysiological cycle (Rosen's, p. 3210):
- Trigger: Anything that reduces SVR (crying, defecation, fever, hypovolemia, tachycardia)
- SVR falls → large R-to-L shunt across VSD → decreased PaO2, increased PCO2, fall in pH
- Metabolic acidosis stimulates the respiratory centre → hyperpnoea
- Hyperpnoea increases venous return to the RV → more blood shunted across VSD (vicious cycle)
- Clinical features: Tachypnoea, progressive cyanosis, decreasing murmur (less flow across RVOT), agitation, possible loss of consciousness
Management of Tet Spells (Rosen's Emergency Medicine, Box 165.8):
| Step | Intervention |
|---|---|
| 1 | Knee-to-chest position (increases SVR, reduces R-to-L shunt) |
| 2 | Supplemental oxygen (limited value alone) |
| 3 | Morphine 0.1-0.2 mg/kg IV/IM (reduces hyperpnoea and anxiety) OR Fentanyl 1 μg/kg IV/IM (or 1.5-2 mcg/kg intranasally) |
| 4 | IV fluid bolus (10-20 mL/kg) to increase preload |
| 5 | Phenylephrine 5-20 μg/kg IV bolus (vasopressor to increase SVR) |
| 6 | Propranolol 0.1 mg/kg slow IV (reduces infundibular spasm) |
| 7 | Sodium bicarbonate 1 mEq/kg IV (corrects metabolic acidosis) |
| 8 | General anaesthesia and surgical intervention if refractory |
Definitive Management: Complete surgical repair (VSD closure + RVOT relief) - typically at 3-6 months of age or earlier if symptomatic.
2. Transposition of the Great Arteries (d-TGA)
Pathophysiology: The aorta arises from the morphologic RV and the pulmonary artery arises from the morphologic LV - creating two parallel, separate circulations that are incompatible with life. Survival depends on mixing through an ASD, VSD, or PDA. D-TGA with intact ventricular septum is the most lethal form (no mixing).
Clinical Features (Harriet Lane Handbook, p. 245):
- Profound cyanosis from birth
- Nonspecific examination; loud, single S2
- No murmur unless associated VSD or PS is present
- Does NOT improve with oxygen (hyperoxia test: PaO2 remains <50 mmHg)
- Presentation: Birth to 2 weeks
ECG: RAD and RVH (RV is the systemic ventricle); upright T wave in V1 after day 3 may be the only abnormality
CXR: Classic "egg on a string" silhouette (narrow mediastinum from the AP relationship of great vessels) + cardiomegaly + increased PVMs
Management:
- Emergency: IV PGE1 to maintain ductal patency for mixing; balloon atrial septostomy (Rashkind procedure) to create/enlarge ASD for inter-atrial mixing
- Definitive: Arterial switch operation (Jatene procedure) - ideally within first 2 weeks of life, before the LV loses its capacity to support the systemic circulation
3. Tricuspid Atresia
Pathophysiology: Absent tricuspid valve with a hypoplastic right ventricle. No blood flow from RA to RV. Survival requires an ASD (for RA-to-LA flow), plus either a PDA or VSD (for some pulmonary blood flow). All systemic venous blood mixes at the LA level.
Clinical Features (Harriet Lane Handbook, p. 245):
- Single S2 ± grade 2-3/6 systolic regurgitation murmur at LLSB (if VSD present)
- Occasional PDA murmur
- Cyanosis degree depends on amount of pulmonary blood flow (VSD/PDA size)
- Presentation: Birth to 2 weeks
ECG:
- Pathognomonic: Superior QRS axis (left axis deviation in a cyanotic infant)
- Right atrial enlargement (RAE) or combined atrial enlargement (CAE) + LVH
CXR: Normal or slightly enlarged heart; may have boot-shaped appearance
Management:
- PGE1 if pulmonary blood flow is inadequate
- Palliative: Modified Blalock-Taussig shunt (MBTS - subclavian to pulmonary artery) in neonates
- Staged Fontan circulation repair over years
4. Total Anomalous Pulmonary Venous Return (TAPVR)
Pathophysiology: Pulmonary veins fail to connect to the left atrium. All four pulmonary veins drain anomalously into the systemic venous circulation. An ASD or patent foramen ovale (PFO) is mandatory for survival (only route of oxygenated blood to the left heart).
Four types (Harriet Lane Handbook, p. 245):
- Supracardiac (most common ~50%): Pulmonary veins drain into SVC via vertical vein
- Cardiac (~25%): Drain into coronary sinus or RA directly
- Subdiaphragmatic/Infracardiac (~20%): Drain below the diaphragm into IVC, portal vein, ductus venosus, or hepatic vein - usually obstructed (most critical form)
- Mixed (~5%)
Clinical Features (Harriet Lane Handbook, p. 245-246):
- Hyperactive RV impulse, quadruple rhythm
- S2 fixed and widely split (mimics ASD)
- 2-3/6 SEM at LUSB + mid-diastolic rumble at LLSB
ECG: RAD, RVH (RSR' in V1); may see RAE
CXR:
- Classic "snowman" or "figure-of-eight" sign (enlarged vertical vein + SVC + RA creating the snowman shape + congested pulmonary vasculature)
- However, this classic finding is rarely seen until after 4 months of age
- Infradiaphragmatic TAPVR: Small heart with severe pulmonary oedema (looks like respiratory distress syndrome)
Presentation: Birth to 2 weeks (obstructed type presents very acutely at birth)
Management:
- Obstructed TAPVR: Surgical emergency - pulmonary venous confluence to LA anastomosis (no role for PGE1 - it may worsen pulmonary congestion in obstructed types)
- Non-obstructed TAPVR: Elective surgical repair in early infancy
5. Truncus Arteriosus
Pathophysiology: A single great vessel (truncus) arises from the heart and gives rise to both the aorta and pulmonary artery. Always associated with a large, conoventricular VSD. Blood from both ventricles mixes completely in the single truncal vessel, leading to obligate mixing cyanosis. Causes increased pulmonary blood flow (pulmonary hypertension can develop rapidly).
Incidence: <1% of all CHD (Harriet Lane Handbook, p. 245)
ECG: BVH (biventricular hypertrophy - from the diagram above, truncus = BVH + cyanosis)
CXR: Cardiomegaly, increased PVMs, right-sided aortic arch (35%)
Presentation: Birth to 2 weeks, presenting with cardiac failure from excessive pulmonary blood flow
Management:
- Surgical repair (Rastelli-type repair): Separation of pulmonary artery from truncus + RV-to-PA conduit + VSD closure - ideally in neonatal period
6. Ebstein Anomaly
Pathophysiology: Downward displacement of the tricuspid valve into the RV, causing massive tricuspid regurgitation and "atrialisation" of part of the RV. The functional RV is very small. Right atrial pressure is high, forcing R-to-L shunting across a PFO/ASD.
Clinical Features:
- Presents birth to 2 weeks (severe form) or later
- Prominent systolic murmur of TR
- Widely split S1 (sail sound from the large anterior TV leaflet)
- "Wall-to-wall" heart on CXR (massive cardiomegaly)
- ECG: Tall P waves, RBBB, delta waves (accessory pathways - Wolf-Parkinson-White in 20-25%)
CXR: Massive cardiomegaly (decreased PVMs)
7. Hypoplastic Left Heart Syndrome (HLHS)
Pathophysiology: Severe underdevelopment of left-sided structures (hypoplastic LV, mitral atresia/stenosis, aortic atresia/stenosis, hypoplastic aortic arch). The RV becomes the single systemic ventricle. Systemic circulation is entirely duct-dependent - the body survives via R-to-L flow through the PDA.
Clinical Features:
- Presents with cardiovascular collapse/shock as ductus closes at 24-48 hours of life
- Grey, mottled, cold; absent pulses; metabolic acidosis
- CXR: Pulmonary oedema, cardiomegaly
- ECG: RVH
Management:
- PGE1 immediately to re-open/maintain PDA
- Staged surgical palliation: Norwood procedure (stage I, neonatal) → bidirectional Glenn (stage II, 4-6 months) → Fontan completion (stage III, 2-4 years)
- OR orthotopic heart transplantation
Summary Comparison Table
| Feature | Acyanotic (L→R Shunts) | Acyanotic (Obstructive) | Cyanotic |
|---|---|---|---|
| Mechanism | L-to-R shunt → pulmonary overcirculation | Outflow obstruction (no shunt at rest) | R-to-L shunt or obligate mixing |
| Cyanosis | Absent (at rest) | Absent | Present |
| Pulmonary BF | Increased | Normal or decreased | Increased (TGA, truncus, TAPVR) OR Decreased (TOF, tricuspid atresia, Ebstein) |
| CXR | Cardiomegaly + increased PVMs | Usually normal | Depends on lesion |
| Key examples | VSD, ASD, PDA, AVSD | PS, AS, CoA | TOF, TGA, tricuspid atresia, TAPVR, truncus |
| Heart failure onset | 4+ weeks (as PVR falls) | Neonatal (critical) or later | Birth to 2 weeks (most) |
| Hyperoxia test | Normal (not cyanotic) | Normal | PaO2 does not rise above 100-150 |
Timing of Presentation Summary
| Presentation | Defects |
|---|---|
| Cyanosis - birth to 2 weeks | TGA, TAPVR, tricuspid atresia, Ebstein, truncus, pulmonary atresia, HRHS, HLHS |
| Cyanosis - birth to 12 weeks | Tetralogy of Fallot |
| Shock (duct-dependent systemic) | CoA, critical AS, HLHS - from first week onward |
| Heart failure (CHF) - 4 weeks onward | VSD, PDA, AVSD |
- The Harriet Lane Handbook (23rd ed.), Table 165.4; Rosen's Emergency Medicine
Eisenmenger Syndrome
A late, irreversible complication of any large, unrepaired L-to-R shunt (VSD > ASD > PDA). Chronic pulmonary overcirculation causes progressive pulmonary vascular remodelling and rising PVR. When PVR exceeds SVR, shunting reverses to R-to-L, causing late-onset cyanosis in a patient previously acyanotic. At this stage, surgical correction of the underlying defect is contraindicated (would remove the pressure relief valve for the RV). Prevention by timely repair is key.
Sources:
- The Harriet Lane Handbook, 23rd Edition (Johns Hopkins Hospital), Tables 7.9, 7.10, 7.11; pp. 240-246
- Rosen's Emergency Medicine, 9th Edition, Chapter 165, pp. 3207-3213
- Braunwald's Heart Disease, 11th Edition - Congenital Heart Disease section
- Robbins & Kumar Basic Pathology - Congenital Heart Disease, p. 156-158
This is a shared conversation. Sign in to Orris to start your own chat.