Varicose vein
Reading File
Finding Sources
Searching PubMed
"varicose veins"[MeSH Terms] AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Varicose Veins
Definition
A vein is called "varicose" when it is dilated and tortuous. While varicosity can affect spermatic veins (varicocele), oesophageal veins, and haemorrhoidal veins, the lower limb is the most clinically significant site. - S Das Manual on Clinical Surgery, 13th Ed.
Anatomy & Pathophysiology
The superficial venous system of the lower limb consists of:
- Long (great) saphenous vein (GSV) - drains into the femoral vein at the sapheno-femoral junction (SFJ)
- Short (small) saphenous vein (SSV) - drains into the popliteal vein at the sapheno-popliteal junction (SPJ)
- Perforating (communicating) veins link the superficial to the deep system
Normal venous return from the leg depends on:
- Competent one-way valves preventing reflux
- The calf muscle pump during walking
- Negative intrathoracic pressure
Varicosity occurs when valves become incompetent - blood refluxes downward (from deep to superficial), causing progressive venous hypertension and dilation of superficial veins.
Aetiology
Primary (majority)
- Cause is not fully known; valves are intrinsically weak
- Familial/genetic predisposition - a 2025 meta-analysis (PMID: 40319023) identified rare variation in PTPRB gene associated with varicose veins
- Erect posture (unique to humans) - increases hydrostatic pressure in leg veins
- Standing occupation (conductors, policemen, tram drivers)
- Female sex (hormonal factor - progesterone causes smooth muscle relaxation in vein walls)
Secondary
- Deep vein thrombosis (DVT) - post-thrombotic valve destruction (most important secondary cause)
- Pregnancy - uterine compression + hormonal effects
- Abdominal/pelvic tumours (fibroids, ovarian cysts, lymphadenopathy) compressing iliac veins
- Retroperitoneal fibrosis
- Ascites
- Congenital arteriovenous fistula (in younger patients)
History Taking
| Feature | Detail |
|---|---|
| Age | Any age; middle-aged most common |
| Sex | Women >> Men (ratio ~10:1) |
| Ethnic group | Less common in primitive African/Asian populations |
| Occupation | Prolonged standing, heavy exertion |
| Symptoms | Aching pain in leg (worse by end of day, relieved by elevation) |
| Night cramps | Common |
| Ankle swelling | Towards end of day |
| Itching | Due to venous stasis |
| Previous history | DVT, prior injection/surgery, pregnancy |
Key teaching point from S Das: "It is not the varicose veins which produce the symptoms, but it is the disordered psychology which is the root of all evils" - asymptomatic varicose veins on one side and severe symptoms with few visible veins on the other side can co-exist.
Clinical Examination
Inspection (standing position)
- Distribution of dilated, tortuous veins along GSV or SSV territory
- Skin changes: pigmentation, eczema, lipodermatosclerosis
- Venous ulcers (typically at the lower third of the medial leg)
- Ankle oedema
Clinical Tests
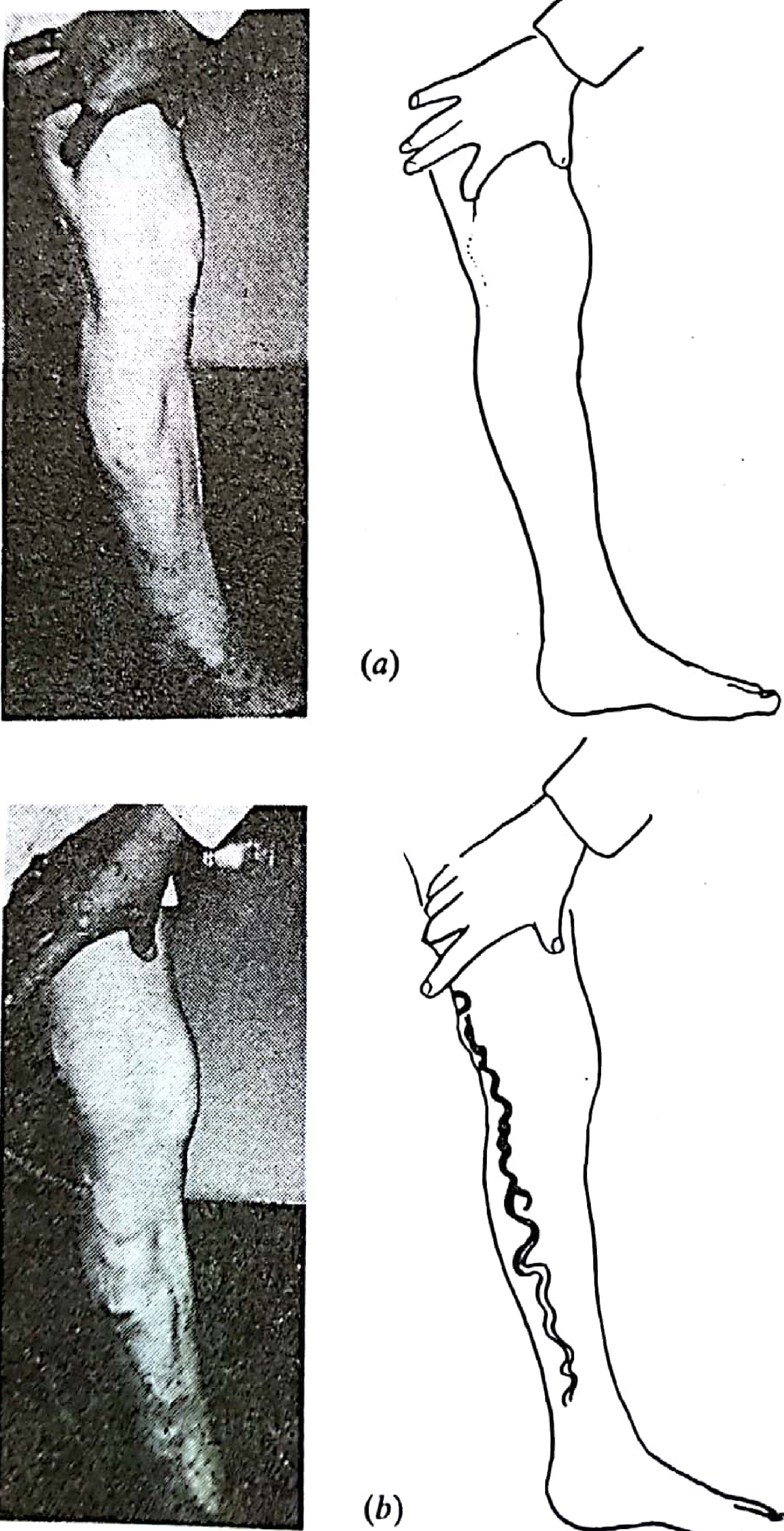
1. Trendelenburg Test
- Elevate the leg to empty the veins
- Compress the SFJ with a finger/tourniquet
- Ask the patient to stand
- If veins remain empty on standing = sapheno-femoral incompetence confirmed
- On releasing compression, rapid filling from above confirms SFJ incompetence
2. Schwartz Test (Percussion Test)
- Tap the most prominent varicosity
- A fluid impulse felt at the saphenous opening indicates absent/incompetent valves between the two fingers
3. Perthes' Test
- Tests deep vein patency
- Tourniquet applied to the thigh; patient asked to walk briskly
- If varicosities empty = deep veins are patent (perforators functioning)
- If varicosities become more prominent or painful = deep veins are blocked (do NOT strip; it is the only venous drainage!)
4. Morrissey's Cough Impulse Test
- Leg elevated, then placed back down
- Patient coughs forcibly
- Expansile impulse felt at the saphenous opening = sapheno-femoral valve incompetence
5. Fegan's Method (locate perforators)
- Mark points of excessive bulge while standing
- Elevate leg; palpate along the varicosities for gaps/pits in the deep fascia = sites of incompetent perforators
Investigations
- Duplex ultrasound - gold standard; identifies site of reflux (SFJ, SPJ, perforators), maps the vein anatomy, confirms deep vein patency, guides intervention
- Doppler - hand-held directional Doppler to detect reflux in superficial veins
- Venography - now largely replaced by duplex
- Ambulatory Venous Pressure (AVP) - AVP >80 mmHg predicts 80% incidence of venous ulceration - Schwartz's Principles of Surgery, 11th Ed.
- Plethysmography - non-invasive assessment of venous reflux and calf pump function
Complications
- Haemorrhage - profuse due to high venous pressure; treat with leg elevation
- Superficial thrombophlebitis - vein becomes tender, firm, red, hot; sometimes extremely painful
- Venous ulceration - usually at lower third medial leg; shallow, flat floor with pink granulation; edge is sloping, pale purple-blue; surrounding pigmentation and induration
- Pigmentation - haemosiderin deposition from RBC extravasation
- Eczema/Dermatitis - pruritic rash overlying varices
- Lipodermatosclerosis - skin thickening and fibrosis from fibrin accumulation and white cell activation
- Calcification of vein wall (phleboliths)
- Periostitis - in long-standing ulcer over tibia
- Equinus deformity - from chronic pain causing habitual tip-toe walking -> Achilles tendon shortening
- Marjolin's ulcer - malignant transformation (squamous cell carcinoma) in a long-standing venous ulcer (raised, everted edge; enlarged inguinal lymph nodes)
CEAP Classification (Chronic Venous Disease)
| Class | Description |
|---|---|
| C0 | No visible/palpable signs |
| C1 | Telangiectases / reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4 | Skin changes (pigmentation, eczema, lipodermatosclerosis) |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
Treatment
1. Conservative
- Compression stockings (graduated elastic support) - suitable for elderly/unfit, pregnant patients, mild disease
- Weight reduction, regular exercise, leg elevation
- Avoid prolonged standing
2. Injection Sclerotherapy
- Sclerosant (e.g. ethanolamine, sodium tetradecyl sulphate, or foam sclerotherapy using polidocanol/STS) is injected into the vein lumen
- Vein is immediately compressed and firmly bandaged for at least 7 days
- Causes fibrosis and obliteration of the lumen
- Limitation: does not address the source of incompetence at the junction - higher recurrence rate than surgery
- Best for: reticular veins, telangiectases, small residual varicosities
3. Endovenous (Minimally Invasive) Techniques - now first-line
These are performed under ultrasound guidance:
a. Endothermal Ablation (preferred by most guidelines):
- Laser (EVLA/EVLT) - 810-1470 nm diode laser; heat destroys vein wall endothelium
- Radiofrequency Ablation (RFA/EVRF) - e.g. ClosureFAST; RF energy causes collagen contraction and fibrosis
- Requires tumescent anaesthesia (perivenous instillation of dilute local anaesthetic + adrenaline)
- Protects surrounding structures and causes vein compression
- A 2024 meta-analysis (PMID: 38316290) comparing RFA vs EVLA found similar efficacy; RFA associated with less post-procedure pain and bruising
b. Mechanochemical Ablation (MOCA)
- Spinning angled wire damages endothelium + simultaneous liquid sclerosant injection
- No tumescent anaesthesia required
- Useful for needle-phobic patients; similar early efficacy to endothermal, but higher medium-term recanalisation rates
c. Endovenous Glue (Cyanoacrylate)
- Cyanoacrylate adhesive injected to seal the lumen
- Minimal intraprocedural pain, no tumescent needed
- Highest consumable cost; long-term data still emerging
4. Open Surgery (traditional - now largely second-line)
Indicated when endovenous options are unavailable or technically unsuitable.
Sapheno-femoral junction (SFJ) ligation and GSV stripping:
- High ligation of GSV flush at SFJ (Trendelenburg operation)
- All tributaries at the SFJ are ligated (reducing neovascularisation and recurrence)
- GSV is then stripped (invagination technique) using a wire stripper
- Followed by phlebectomy (stab avulsions) of varicose tributaries through 2-mm incisions
Sapheno-popliteal junction (SPJ) ligation and SSV stripping:
- Preoperative duplex marking of SPJ is mandatory
- Patient prone; transverse incision over SPJ; SSV ligated flush or proximally
- SPJ stripping vs proximal resection - risk of sural nerve injury
Complications of standard varicose vein surgery (Bailey & Love 28th Ed.):
- Minor and major complications in up to 20% of patients
- Wound infection (most common) - reduced by prophylactic antibiotics
- Nerve injury (saphenous nerve after GSV stripping; sural nerve after SSV procedures)
- Haematoma, DVT, recurrence (from neovascularisation at the SFJ)
Special Considerations
- Pregnancy: Treat conservatively with compression stockings until 6 weeks post-delivery; then re-evaluate
- Deep vein obstruction: If Perthes' test is positive (deep veins blocked), surgical stripping is absolutely contraindicated - the varicose veins are the only route of drainage
- Venous ulcers: Treat the underlying incompetence surgically; local wound care, four-layer compression bandaging; skin grafting for resistant cases
- NICE guidelines (UK): Endothermal ablation is the first-line treatment; foam sclerotherapy second; open surgery third
Sources:
- S Das Manual on Clinical Surgery, 13th Ed.
- Pye's Surgical Handicraft, 22nd Ed.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
- Current Surgical Therapy, 14th Ed.
- RFA vs EVLA meta-analysis: Jiang et al. 2024 (PMID: 38316290)
- PTPRB genetics: Rämo et al. 2025 (PMID: 40319023)
This is a shared conversation. Sign in to Orris to start your own chat.