Anemia , classifications and iron deficiency anemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"iron deficiency anemia" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough, well-illustrated answer.
Anemia: Classifications and Iron Deficiency Anemia
Definition
Anemia is defined as a reduction in blood counts (hemoglobin, hematocrit, or red cell number) below the normal range for a given population. It is not a diagnosis in itself but a manifestation of an underlying process.
- Harrison's Principles of Internal Medicine 22E, p. 492
Classifications of Anemia
There are two major ways to classify anemia: by red cell size (morphologic/MCV-based) and by mechanism (pathophysiologic).
1. Morphologic Classification (by MCV)
Pioneered by hematologist Max Wintrobe, this is the most clinically practical approach because MCV guides the diagnostic workup.
| Category | MCV | Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, thalassemia, anemia of chronic disease/inflammation, sideroblastic anemia |
| Normocytic | 80-100 fL | Aplastic anemia, renal disease, endocrinopathies, myeloma, marrow invasion, pure red cell aplasia |
| Macrocytic | > 100 fL | Oval macrocytes: B12 deficiency, folate deficiency, chemotherapy, myelodysplasia; Round macrocytes: alcohol use, hypothyroidism, liver disease, reticulocytosis, dysproteinemia |
Note: Anemia of chronic disease typically shows normocytic cells, though it can be microcytic in severe or prolonged cases.
- Harrison's Principles of Internal Medicine 22E, p. 492
2. Mechanistic Classification (by Pathophysiology)
The reticulocyte count is the key first step: elevated reticulocytes point to increased destruction/loss; low reticulocytes point to underproduction.
A. Blood Loss
- Acute: trauma
- Chronic: GI lesions (peptic ulcer, colorectal cancer), gynecologic causes
B. Increased Red Cell Destruction (Hemolysis)
Inherited (intrinsic) causes:
- Red cell membrane disorders: hereditary spherocytosis, hereditary elliptocytosis
- Enzyme deficiencies: G6PD deficiency (HMP shunt), pyruvate kinase deficiency (glycolysis)
- Hemoglobin abnormalities: thalassemia syndromes (deficient globin synthesis), sickle cell disease, unstable hemoglobins
Acquired causes:
- Paroxysmal nocturnal hemoglobinuria (PNH) - phosphatidylinositol-linked glycoprotein deficiency
- Antibody-mediated: autoimmune hemolytic anemia, hemolytic disease of the newborn, transfusion reactions, drug-induced
- Microangiopathic hemolytic anemia (MAHA): HUS, DIC, TTP
- Cardiac traumatic hemolysis: defective valves
- Infections: malaria, babesiosis
- Repetitive physical trauma (march hemoglobinuria)
C. Decreased Red Cell Production (Underproduction)
-
Nutritional deficiencies: iron deficiency (impairs heme synthesis), B12/folate deficiency (impairs DNA synthesis), copper, Vitamin C
-
Erythropoietin deficiency: renal disease, anemia of inflammation, anemia of aging
-
Stem cell/progenitor failure: aplastic anemia, pure red cell aplasia, Fanconi anemia
-
Marrow replacement: metastatic neoplasms, granulomatous disease, infections
-
Primary hematopoietic neoplasms: leukemia, myelodysplastic syndromes
-
Robbins, Cotran & Kumar - Pathologic Basis of Disease, Table 14.1
Iron Deficiency Anemia (IDA)
Iron deficiency is the most common nutritional disorder in the world and the most common cause of anemia globally.
At-Risk Populations
- Infants and toddlers
- Adolescent girls
- Women of childbearing age (due to menstruation)
- Pregnant women
- People in low-resource countries (poor diet + parasite burden)
Iron Metabolism (Normal)
Iron Distribution in Healthy Adults:
| Pool | Males (mg) | Females (mg) |
|---|---|---|
| Total | 3450 | 2450 |
| Hemoglobin | 2100 | 1750 |
| Myoglobin | 300 | 250 |
| Enzymes | 50 | 50 |
| Storage (ferritin/hemosiderin) | 1000 | 400 |
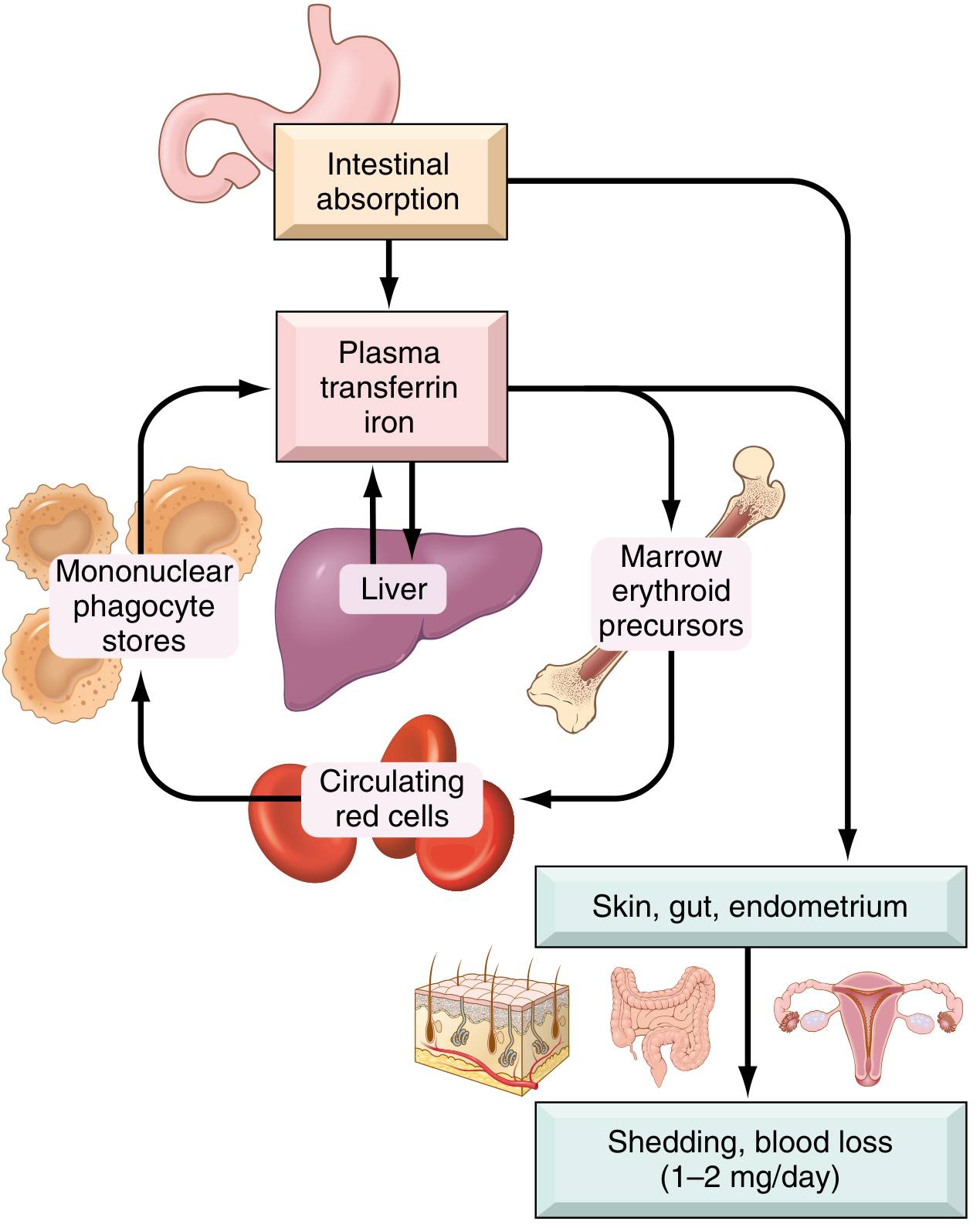
Key points of iron metabolism:
- No regulated excretion pathway - daily losses limited to 1-2 mg (shed epithelial cells)
- Dietary iron: 10-20 mg/day in the US diet; ~20% of heme iron is absorbed vs. only 1-2% of nonheme iron
- Iron is transported in plasma bound to transferrin (normally ~1/3 saturated)
- Storage forms: ferritin (water-soluble, found in hepatocytes/macrophages) and hemosiderin (aggregated ferritin in lysosomes; stains Prussian blue)
- Regulation: Hepcidin (liver peptide) binds and degrades ferroportin, blocking iron transfer from enterocytes and macrophages into plasma. High iron body stores = high hepcidin = less absorption; low stores = low hepcidin = more absorption
Etiology of IDA
Iron deficiency results from one or more of these four mechanisms:
- Dietary lack - more common in low-resource countries where diet is predominantly non-heme iron (poorly absorbed). Rare in developed nations.
- Impaired absorption - celiac disease, post-gastrectomy, achlorhydria, drugs (antacids, PPIs), TMPRSS6 mutations (rare)
- Increased requirement - pregnancy (fetal demand + blood volume expansion), infancy/adolescence (rapid growth), lactation
- Chronic blood loss - the most important cause in adults in high-resource countries
- GI blood loss: peptic ulcers, esophageal varices, colorectal cancer, angiodysplasia, hookworm
- Gynecologic: menorrhagia, fibroids
- Repeated phlebotomy or hemodialysis
- Pulmonary hemosiderosis
Important: In adult men and postmenopausal women, IDA should always trigger a search for a GI source of bleeding, as occult colorectal cancer is a significant concern.
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 614
Stages of Iron Deficiency
| Stage | Features |
|---|---|
| Pre-latent (Iron depletion) | Depleted bone marrow stores; serum ferritin falls; no anemia yet |
| Latent (Iron-deficient erythropoiesis) | Serum iron falls, TIBC rises, transferrin saturation falls; no anemia |
| Iron deficiency anemia | Hemoglobin falls; microcytic hypochromic anemia develops |
Pathologic Blood Film

Fig: Iron deficiency anemia - peripheral blood smear showing hypochromic microcytic red cells containing a narrow rim of peripheral hemoglobin. (Robbins, Cotran & Kumar - Pathologic Basis of Disease)
Clinical Features
Anemia-related (general):
- Fatigue, pallor, dyspnea on exertion, palpitations, weakness, headache
IDA-specific (from depletion of iron-containing enzymes throughout the body):
- Koilonychia (spoon-shaped nails)
- Angular cheilitis (cracking at corners of mouth)
- Glossitis (atrophy of tongue papillae, sore tongue)
- Pica - craving for non-foodstuffs (clay = geophagia; ice = pagophagia; starch = amylophagia)
- Plummer-Vinson syndrome (rare): triad of microcytic hypochromic anemia + atrophic glossitis + esophageal webs
- Alopecia, gastric mucosal atrophy, intestinal malabsorption
- Restless legs syndrome - iron depletion from the CNS
Laboratory Diagnosis
| Test | Finding in IDA |
|---|---|
| Hemoglobin / Hematocrit | Low |
| MCV | Low (< 80 fL) |
| MCH / MCHC | Low (hypochromia) |
| Serum iron | Low |
| TIBC (Total Iron-Binding Capacity) | High (reflects elevated transferrin) |
| Transferrin saturation | < 15% (normally ~20-45%) |
| Serum ferritin | Low (< 12 µg/L) |
| Hepcidin | Low (suppressed by iron depletion) |
| Reticulocytes | Low (before treatment) |
| Peripheral smear | Microcytic, hypochromic RBCs; poikilocytosis (pencil cells, target cells) |
IDA vs. Anemia of Chronic Inflammation (ACI) - Key Distinction
| Parameter | IDA | ACI |
|---|---|---|
| Serum iron | Low | Low |
| TIBC | High | Low |
| Transferrin saturation | Low | Low |
| Serum ferritin | Low | High/Normal |
| Storage iron (bone marrow) | Absent | Increased |
| Hepcidin | Low | High (IL-6 driven) |
In ACI, inflammatory mediators (especially IL-6) stimulate hepcidin production, locking iron inside macrophages and preventing its use by erythroid precursors - "iron in the midst of plenty."
Treatment
Oral iron supplementation is first-line:
- Ferrous sulfate 325 mg three times daily (contains ~65 mg elemental iron per tablet)
- Take on an empty stomach; Vitamin C enhances absorption
- Response: reticulocyte count rises in 5-7 days, followed by steady Hb rise
- Full correction of Hb takes 6-8 weeks; iron stores take 3-6 months to replenish
- Common side effects: constipation, nausea, dark stools
IV iron (ferric carboxymaltose, ferric gluconate, iron sucrose, low-molecular-weight iron dextran):
- Used when oral iron is not tolerated, not absorbed (malabsorption), or blood loss exceeds what oral supplementation can replace
- Preferred in inflammatory bowel disease, post-bariatric surgery, CKD, heart failure, pregnancy with severe IDA
Treat the underlying cause - this is as important as supplementation. Without correcting the source of blood loss or nutritional inadequacy, recurrence is inevitable.
Sources: Harrison's Principles of Internal Medicine 22E; Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology
Recent evidence: A 2026 systematic review and meta-analysis (PMID: 41241142) on pediatric IDA treatment confirms oral iron is effective first-line therapy, with IV iron as a safe alternative for refractory cases.
This is a shared conversation. Sign in to Orris to start your own chat.