Hii
Hey there! How can I help you today?
Can you hell me learn pharma
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have excellent content to build a thorough, nurse-friendly pharmacology basics guide. Here it is:
Pharmacology Basics for Nursing Students
Based on Katzung's Basic & Clinical Pharmacology, 16th Edition
1. What Is Pharmacology?
Pharmacology is the study of substances (drugs) that interact with living systems through chemical processes. For nurses, the two most important branches are:
- Pharmacokinetics - what the body does to the drug (how it's absorbed, distributed, metabolised, excreted)
- Pharmacodynamics - what the drug does to the body (mechanisms of action, effects)
2. What Is a Drug?
A drug is any substance that changes a biological function through chemical action. Most drugs work by binding to a receptor - a specific target molecule that plays a regulatory role in the body.
- Agonist - activates the receptor (mimics the body's natural response)
- Antagonist - blocks the receptor (prevents the natural response)
Key point: "The dose makes the poison" (Paracelsus, 1493-1541). Any substance can be harmful at the wrong dose - this is why nurses must be precise with drug dosing.
3. Pharmacokinetics: ADME
Think of the acronym ADME - the four processes governing a drug's journey through the body:
A - Absorption
How the drug gets from the administration site into the bloodstream.
- Depends on the route of administration (oral, IV, IM, sublingual, transdermal, etc.)
- Oral drugs must survive the stomach environment and pass through the gut wall
- IV drugs bypass absorption - they go directly into the blood (100% bioavailability)
- Lipid-soluble (non-ionized) drugs cross membranes more easily than water-soluble ones
D - Distribution
How the drug spreads from the blood to tissues and organs.
- Measured by Volume of Distribution (Vd) - a theoretical volume describing how widely the drug spreads
- High Vd = drug distributes widely into tissues (e.g. fat-soluble drugs)
- Low Vd = drug stays mostly in the blood
- Some drugs bind to plasma proteins (mainly albumin); only the free (unbound) fraction is active
M - Metabolism
How the drug is chemically transformed, mainly in the liver.
- The liver uses enzymes (especially Cytochrome P450 / CYP enzymes) to break down drugs
- Metabolism often converts an active drug to an inactive form for easier elimination
- Some drugs are prodrugs - inactive when taken, activated by metabolism (e.g. codeine → morphine)
- Drug interactions often happen here - some drugs inhibit or induce CYP enzymes, affecting other drugs' levels
E - Excretion
How the drug is removed from the body.
- Primarily via the kidneys (urine) - water-soluble metabolites are excreted
- Also via bile, faeces, lungs (inhaled anaesthetics), sweat, breast milk
- Patients with kidney or liver disease may need dose adjustments since they can't eliminate drugs normally
4. Key Pharmacokinetic Parameters
Half-Life (t½)
The time required for the amount of drug in the body to decrease by half.
Formula: t½ = 0.7 × Volume of Distribution / Clearance
Why it matters for nurses:
- It takes 4-5 half-lives to reach steady-state (when drug levels stabilise)
- It also takes 4-5 half-lives to eliminate a drug after stopping it
- A drug given every half-life will accumulate; if dosing interval is shorter than 4 half-lives, accumulation is detectable
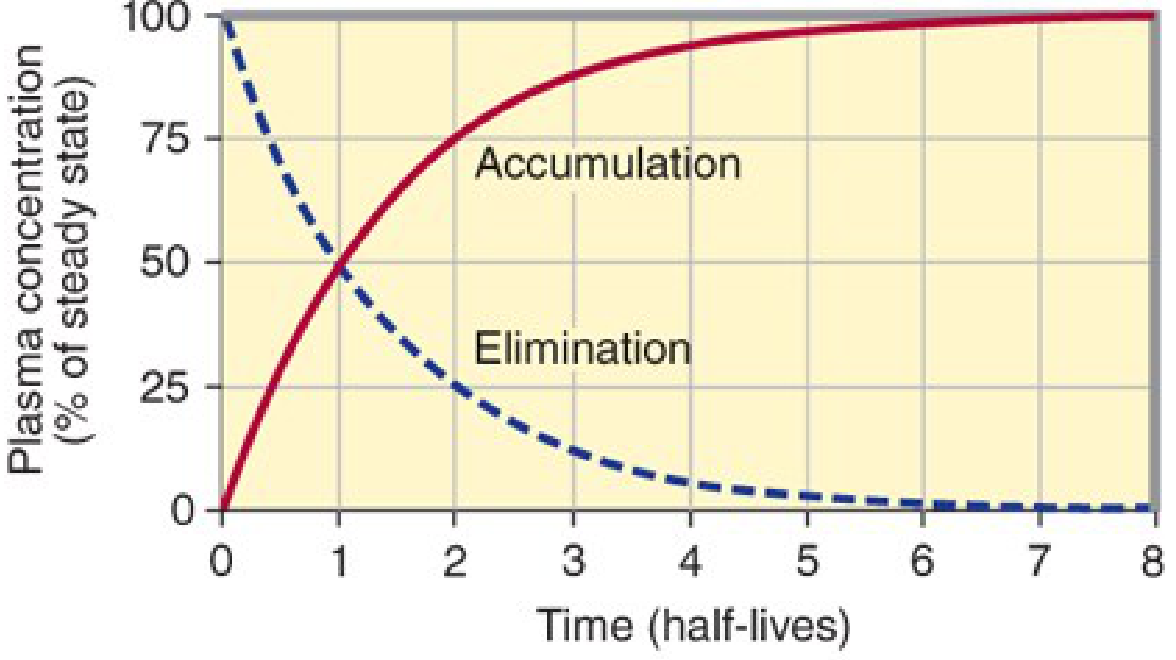
The solid line shows drug accumulating to ~90% steady state after 4 half-lives. The dashed line shows elimination after stopping the drug.
Clearance (CL)
The volume of blood cleared of drug per unit time. Reduced in kidney/liver disease - a critical consideration for safe nursing practice.
5. Pharmacodynamics: How Drugs Work
Drug-Receptor Interaction
Drugs work by binding to receptors and either:
- Activating them (agonist) - produces a response
- Blocking them (antagonist) - prevents a response
Dose-Response Relationship
- ED50 - the dose that produces 50% of the maximum effect
- Therapeutic window - the range between the effective dose and the toxic dose
- Therapeutic index - ratio of toxic dose to effective dose; a narrow therapeutic index (e.g. digoxin, warfarin, lithium) means careful monitoring is needed
6. Routes of Administration - A Nursing Quick-Reference
| Route | Onset | Key Notes |
|---|---|---|
| IV (intravenous) | Fastest (seconds-minutes) | 100% bioavailable; no absorption step |
| IM (intramuscular) | Minutes | Good for some vaccines and emergencies |
| SC (subcutaneous) | Slower than IM | Used for insulin, heparin |
| Oral (PO) | Slowest (30-60 min) | Most convenient; first-pass metabolism |
| Sublingual | Fast (minutes) | Bypasses first-pass (e.g. nitroglycerin) |
| Transdermal | Very slow (hours) | Sustained release (e.g. nicotine patch) |
7. First-Pass Effect (Hepatic First-Pass Metabolism)
When a drug is taken orally, it is absorbed from the gut and travels first to the liver via the portal vein before reaching systemic circulation. The liver may metabolise a large fraction of the drug before it even reaches its target.
- Drugs with high first-pass effect (e.g. morphine, nitroglycerin) have low oral bioavailability
- This is why nitroglycerin is given sublingually (under the tongue) - it bypasses the liver
8. Drug Interactions - Basics
-
Pharmacokinetic interactions - one drug alters the absorption, distribution, metabolism, or excretion of another
- Example: rifampicin induces CYP enzymes → lowers levels of other drugs metabolised by the same enzymes
- Example: fluconazole inhibits CYP enzymes → raises levels of other drugs (risk of toxicity)
-
Pharmacodynamic interactions - two drugs have additive, synergistic, or antagonistic effects at their receptors
- Example: two CNS depressants (opioids + benzodiazepines) together cause additive respiratory depression
9. Special Populations (Important for Nursing!)
| Population | Key Concern |
|---|---|
| Elderly patients | Reduced renal/hepatic function; increased drug sensitivity; start low, go slow |
| Renal failure | Reduced excretion; drugs accumulate; dose adjustment needed |
| Hepatic failure | Reduced metabolism; active drug builds up |
| Pregnant patients | Drug may cross placenta; fetal harm risk; check pregnancy category |
| Paediatric patients | Different weight-based dosing; immature enzyme systems |
Where to Go Next
Once you're comfortable with these basics, good next topics to study are:
- Autonomic pharmacology (sympathomimetics, beta-blockers, anticholinergics)
- Analgesics (opioids, NSAIDs)
- Antibiotics (mechanisms and resistance)
- Cardiovascular drugs (antihypertensives, antiarrhythmics, diuretics)
- Drug calculations (doses, drip rates, unit conversions)
Would you like me to go deeper into any of these sections, or move on to a specific drug class you'll be encountering in clinical practice?
Explain drug calculations and dosing for clinical practice
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent content from both Katzung and Lippincott. Now I have everything needed for a thorough, practical guide.
Drug Calculations & Dosing for Clinical Practice
Based on Katzung's Basic & Clinical Pharmacology 16e and Lippincott Illustrated Reviews: Pharmacology
Part 1 - The Master Formula (The Foundation of All Drug Calculations)
The single most important formula in nursing practice:
$$\text{Volume to give} = \frac{\text{Desired Dose}}{\text{Available Dose}} \times \text{Available Volume}$$
Example:
- Doctor orders: 250 mg of amoxicillin
- On hand: amoxicillin 500 mg / 5 mL suspension
$$\text{Volume} = \frac{250\text{ mg}}{500\text{ mg}} \times 5\text{ mL} = \mathbf{2.5 mL}$$
Part 2 - Weight-Based Dosing (mg/kg)
Used for most paediatric drugs, heparin, antibiotics, chemotherapy, and many critical care drugs.
$$\text{Total Dose} = \text{Weight (kg)} \times \text{Dose (mg/kg)}$$
Example:
- Child weighs 20 kg, doctor orders amoxicillin 25 mg/kg/day in 2 divided doses
- Total daily dose = 20 × 25 = 500 mg/day
- Each dose = 500 ÷ 2 = 250 mg twice daily
Then apply the master formula to calculate the volume to draw up.
Part 3 - IV Infusion Rate Calculations
3a. mL per Hour
Used when a pump is available (most modern wards):
$$\text{Rate (mL/hr)} = \frac{\text{Volume to infuse (mL)}}{\text{Time (hours)}}$$
Example: Infuse 1000 mL of normal saline over 8 hours
$$\text{Rate} = \frac{1000}{8} = \mathbf{125 \text{ mL/hr}}$$
3b. Drops per Minute (Manual Drip - no pump)
Used in settings without infusion pumps. You need to know the drop factor of the IV giving set:
- Standard giving set: 20 drops/mL
- Blood/high-viscosity giving set: 15 drops/mL
- Micro-drip/paediatric giving set: 60 drops/mL
$$\text{Drops/min} = \frac{\text{Volume (mL)} \times \text{Drop factor}}{\text{Time (minutes)}}$$
Example: 500 mL over 4 hours using a standard set (20 drops/mL)
$$\text{Drops/min} = \frac{500 \times 20}{4 \times 60} = \frac{10000}{240} \approx \mathbf{42 \text{ drops/min}}$$
3c. Drug Infusion Rate (mcg/kg/min)
Common in ICU - for vasopressors (dopamine, noradrenaline), heparin, insulin infusions:
$$\text{Infusion rate (mL/hr)} = \frac{\text{Dose (mcg/kg/min)} \times \text{Weight (kg)} \times 60}{\text{Concentration (mcg/mL)}}$$
Example: Dopamine ordered at 5 mcg/kg/min for a 70 kg patient. Bag = dopamine 400 mg in 250 mL (concentration = 400,000 mcg ÷ 250 mL = 1600 mcg/mL)
$$\text{Rate} = \frac{5 \times 70 \times 60}{1600} = \frac{21000}{1600} \approx \mathbf{13.1 \text{ mL/hr}}$$
Part 4 - Loading Dose vs Maintenance Dose
This is a key clinical concept. According to Katzung:
"In most clinical situations, drugs are administered so as to maintain a steady state of drug in the body, where the amount given with each dose replaces the drug eliminated since the preceding dose."
Maintenance Dose
Keeps the drug at a stable therapeutic level (steady-state concentration, or Css).
- It takes 4-5 half-lives to reach steady state from zero
- Formula: Dosing Rate = Clearance (CL) × Target Concentration (TC)
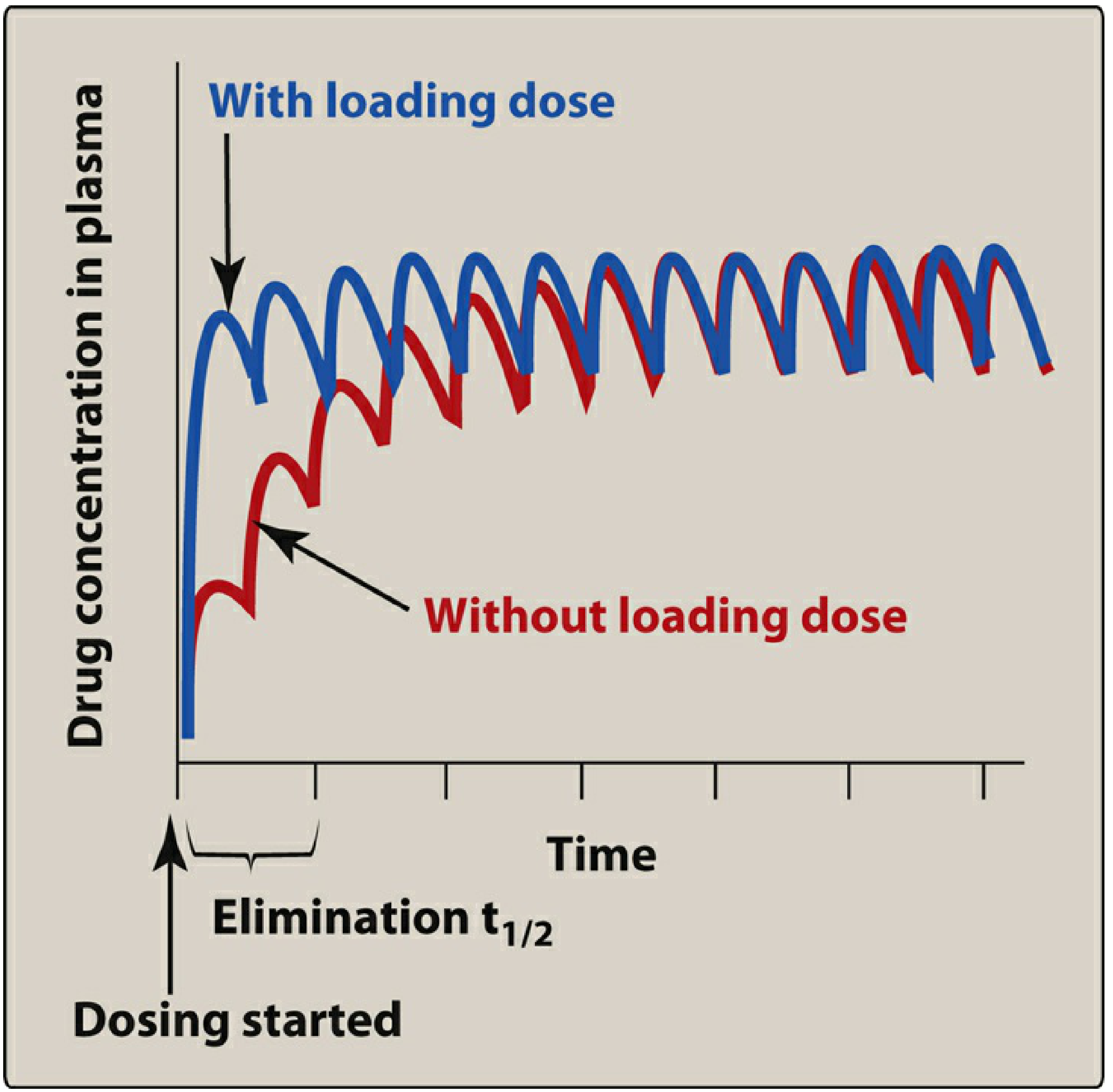
Loading Dose
Given when you need to reach therapeutic levels quickly - particularly for drugs with long half-lives (e.g. digoxin, amiodarone, phenytoin).
$$\text{Loading Dose} = V_d \times \text{Target Concentration (TC)}$$
Example from Katzung (theophylline):
- Target plasma level = 10 mg/L
- Volume of distribution (Vd) = 35 L (for a 70 kg person)
- Loading dose = 35 × 10 = 350 mg (given as a single dose to rapidly reach target)
- Maintenance dose = 350 mg every 12 hrs orally to keep that level
Nursing caution: Loading doses carry increased toxicity risk. IV loading doses must be given slowly (e.g. over an hour, NOT by rapid bolus) to prevent dangerously high initial concentrations - especially for phenytoin, digoxin, and amiodarone.
Part 5 - Therapeutic Drug Monitoring (TDM)
Some drugs have a narrow therapeutic index - the gap between the effective dose and the toxic dose is small. These drugs must be monitored with blood levels.
| Drug | Therapeutic Range | Toxic Signs to Watch For |
|---|---|---|
| Digoxin | 0.5-2 ng/mL | Nausea, bradycardia, visual changes |
| Lithium | 0.6-1.2 mEq/L | Tremor, confusion, arrhythmia |
| Warfarin | INR 2-3 (most indications) | Bleeding |
| Phenytoin | 10-20 mcg/mL | Nystagmus, ataxia, confusion |
| Gentamicin | Peak 5-10 mcg/mL | Nephrotoxicity, ototoxicity |
| Theophylline | 10-20 mcg/mL | Nausea, seizures, arrhythmia |
From Lippincott Illustrated Reviews: Pharmacology - "If the therapeutic window of the drug is small (for example, digoxin or lithium), extra caution should be taken in selecting a dosage regimen, and drug levels should be monitored."
Part 6 - Dose Adjustments in Special Populations
Renal Impairment
- Kidneys are the primary route of excretion for most drugs
- Reduced clearance → drug accumulates → toxicity risk
- Key dose reduction formula using creatinine clearance (CrCl) - calculated by the Cockcroft-Gault equation:
$$\text{CrCl (mL/min)} = \frac{(140 - \text{age}) \times \text{weight (kg)}}{72 \times \text{serum creatinine (mg/dL)}} \times (0.85 \text{ if female})$$
- If CrCl is reduced, the dose is reduced or the interval is extended
- Drugs needing renal dose adjustment include: gentamicin, metformin, digoxin, many antibiotics
Hepatic Impairment
- Liver metabolises most drugs via CYP enzymes
- Reduced metabolism → higher drug levels → toxicity
- Particularly relevant for: morphine, warfarin, statins, antifungals
Elderly Patients
- Reduced renal AND hepatic function
- Lower body weight and higher fat/muscle ratio changes Vd
- Principle: "Start low, go slow"
Paediatric Patients
- Immature liver enzymes (especially in neonates)
- Always dose by weight (mg/kg) - never extrapolate adult doses
- Dose adjustment reference: Harriet Lane Handbook
Part 7 - The 5 Rights of Medication Administration (Never Skip These)
Before giving any drug, verify:
| Right | What to Check |
|---|---|
| Right Patient | Two identifiers (name + DOB or ID) |
| Right Drug | Correct medication name (generic vs brand confusion is common) |
| Right Dose | Recalculate - never assume someone else's calculation |
| Right Route | Oral, IV, IM, sublingual, topical, etc. |
| Right Time | Correct frequency and timing relative to meals/other drugs |
Some institutions add: Right Documentation, Right Reason, Right Response.
Part 8 - Quick Reference: Unit Conversions for Drug Calculations
| From | To | Multiply by |
|---|---|---|
| grams (g) | milligrams (mg) | × 1,000 |
| milligrams (mg) | micrograms (mcg / μg) | × 1,000 |
| micrograms (mcg) | nanograms (ng) | × 1,000 |
| kilograms (kg) | pounds (lb) | × 2.2 |
| litres (L) | millilitres (mL) | × 1,000 |
Common trap: Orders may be written in mcg but your drug vial may be labelled in mg. Always convert to the same unit before calculating.
Practice Questions
Try these to test yourself:
Q1. A doctor orders gentamicin 80 mg IV. On hand: gentamicin 40 mg/mL. How many mL do you draw up?
Q2. Infuse 500 mL of D5W over 6 hours. What is the rate in mL/hr?
Q3. A child weighs 15 kg. The order is paracetamol 15 mg/kg. The suspension is 250 mg/5 mL. What volume do you give?
Q4. Heparin infusion running at 25,000 units in 500 mL. Patient needs 1,000 units/hr. What is the pump rate in mL/hr?
(Answers: Q1 = 2 mL, Q2 = 83.3 mL/hr, Q3 = 4.5 mL, Q4 = 20 mL/hr)
Would you like me to go deeper on any of these areas - for example, heparin/insulin infusion calculations, paediatric dosing, or practice a set of worked examples together?
Which drug should be given together
Asking for Preferences
Not be given together
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Excellent - I now have rich, textbook-backed content across all the major dangerous drug combinations. Here's a comprehensive guide:
Dangerous Drug Combinations - What Must NOT Be Given Together
Based on Tintinalli's Emergency Medicine, Katzung's Basic & Clinical Pharmacology 16e, Goodman & Gilman's, and The Washington Manual
The Big Categories of Dangerous Drug Interactions
There are two main types of interactions that cause harm:
- Pharmacokinetic - one drug changes how the body processes another (absorption, metabolism, excretion) - leading to toxic levels or sub-therapeutic levels
- Pharmacodynamic - two drugs have additive or opposing effects at the same receptors - leading to exaggerated or dangerous responses
1. MAOIs + Serotonergic Drugs → Serotonin Syndrome (Life-Threatening)
This is one of the most dangerous combinations in all of pharmacology.
MAOIs (Monoamine Oxidase Inhibitors):
- Phenelzine, tranylcypromine, isocarboxazid (antidepressants)
- Selegiline (Parkinson's)
- Linezolid (antibiotic - often forgotten!)
- Methylene blue (used in surgeries - often forgotten!)
NEVER combine MAOIs with:
| Drug | Why Dangerous |
|---|---|
| SSRIs (fluoxetine, sertraline, etc.) | Massive serotonin excess |
| SNRIs (venlafaxine, duloxetine) | Massive serotonin excess |
| Meperidine (pethidine) | Fatal serotonin syndrome |
| Tramadol | Serotonin + seizure risk |
| Dextromethorphan (cough syrups) | Serotonin syndrome |
| Cocaine, MDMA, methamphetamine | Severe serotonergic + adrenergic crisis |
What happens: Fever, agitation, muscle rigidity, tremor, diarrhoea, fast heart rate, seizures, and death.
Washout rule (from Tintinalli's): SSRIs/SNRIs must be stopped 2 weeks before starting an MAOI. Fluoxetine needs 4 weeks (long half-life). After stopping an MAOI, wait 2 weeks before starting any serotonergic drug - because it takes 2 weeks for MAO enzyme activity to recover 50%.
2. Opioids + Benzodiazepines → Fatal Respiratory Depression
This is the most common drug combination contributing to overdose deaths.
Examples:
- Morphine/oxycodone/codeine/fentanyl + diazepam/midazolam/lorazepam/alprazolam
Why so dangerous: Both drug classes independently depress the central nervous system and slow breathing. Together, the effect is additive to synergistic - patients stop breathing.
From Rosen's Emergency Medicine: "Among opioid overdose deaths, one-third have benzodiazepine present."
Nursing alert: If a patient on both drugs becomes drowsy or their respiratory rate drops below 12/min, act immediately. Have naloxone (Narcan) ready.
Also avoid combining opioids with:
- Alcohol
- Antihistamines (promethazine, diphenhydramine)
- Muscle relaxants (cyclobenzaprine)
- Antipsychotics
- Any other CNS depressant
3. Warfarin + NSAIDs → Severe Bleeding
| Why it's dangerous | Mechanism |
|---|---|
| NSAIDs inhibit platelet function | Pharmacodynamic - impairs clotting |
| NSAIDs displace warfarin from plasma proteins | Pharmacokinetic - raises free warfarin levels |
| NSAIDs cause gastric ulcers | Increases GI bleeding risk directly |
From Rosen's: "NSAIDs displace protein-bound warfarin and cause subsequent increases in prothrombin times at a constant warfarin dose. NSAID use is generally avoided in patients who are taking warfarin."
Practical rule: Patients on warfarin should use paracetamol (acetaminophen) for pain relief instead of ibuprofen/naproxen/aspirin (except low-dose aspirin when specifically prescribed for cardiac protection - which itself requires careful monitoring).
4. ACE Inhibitors/ARBs + Potassium-Sparing Diuretics → Life-Threatening Hyperkalemia
The dangerous combination:
- ACE inhibitors (lisinopril, enalapril, ramipril) OR ARBs (losartan, valsartan)
- PLUS potassium-sparing diuretics (spironolactone, amiloride) or potassium supplements
Why: ACE inhibitors reduce aldosterone → retain potassium. Potassium-sparing diuretics also retain potassium. Together, potassium can rise to dangerous levels causing life-threatening cardiac arrhythmias.
Also avoid ACE inhibitor/ARB + ACE inhibitor/ARB (double blockade - causes severe hypotension and acute kidney injury)
From The Washington Manual: "Oral potassium supplements, potassium salt substitutes, and potassium-sparing diuretics should be used with caution during treatment with an ACE inhibitor."
5. QT-Prolonging Drugs Taken Together → Torsades de Pointes (Fatal Arrhythmia)
Many drugs independently prolong the QT interval on an ECG. Combining them multiplies the risk of a fatal ventricular arrhythmia called Torsades de Pointes.
Common QT-prolonging drugs to NOT combine:
| Drug Class | Examples |
|---|---|
| Antiarrhythmics | Amiodarone, sotalol, quinidine |
| Antipsychotics | Haloperidol, quetiapine, ziprasidone |
| Antibiotics | Azithromycin, ciprofloxacin, clarithromycin |
| Antifungals | Fluconazole, ketoconazole |
| Antiemetics | Ondansetron (especially IV, high dose), domperidone |
| Antidepressants | Citalopram (high doses), tricyclics |
High-risk combinations to flag: Azithromycin + ondansetron, amiodarone + fluconazole, haloperidol + ciprofloxacin.
Nursing action: Check a baseline ECG before starting these drugs. Report QTc > 500 ms to the prescriber.
6. Azathioprine + Allopurinol → Severe Bone Marrow Toxicity
From Fitzpatrick's Dermatology: "A major drug interaction occurs between azathioprine and allopurinol. When allopurinol must be used concurrently with azathioprine, the azathioprine dose should be decreased by 75%."
Why: Allopurinol inhibits xanthine oxidase, the enzyme that breaks down azathioprine. Azathioprine accumulates to toxic levels, suppressing the bone marrow → dangerous fall in white cells, red cells, and platelets.
7. Methotrexate + NSAIDs → Methotrexate Toxicity
NSAIDs reduce kidney blood flow and compete with methotrexate for renal tubular secretion. Methotrexate builds up → bone marrow suppression, mucositis, liver and kidney damage.
Rule: NSAIDs are generally avoided in patients on methotrexate, especially high-dose regimens.
8. Other Important Combinations to Avoid
| Combination | Risk |
|---|---|
| Statins + strong CYP3A4 inhibitors (e.g., clarithromycin, itraconazole) | Statin toxicity → rhabdomyolysis (muscle breakdown) |
| Digoxin + amiodarone or verapamil | Digoxin toxicity (raised blood levels) |
| Lithium + NSAIDs or thiazide diuretics | Lithium toxicity (reduced renal excretion) |
| Metformin + IV contrast dye | Lactic acidosis (metformin must be held 48 hrs before/after contrast) |
| Valproic acid + lamotrigine | Doubles lamotrigine levels → toxicity |
| Alcohol + metronidazole or tinidazole | Disulfiram-like reaction (flushing, vomiting, tachycardia) |
| Sildenafil (Viagra) + nitrates | Severe, potentially fatal hypotension |
| Linezolid + SSRIs/SNRIs | Serotonin syndrome (linezolid is a weak MAOI!) |
Quick Summary Table - Critical Interactions
| Drug A | Drug B | Danger |
|---|---|---|
| MAOIs | SSRIs / meperidine / tramadol | Serotonin syndrome - FATAL |
| Opioids | Benzodiazepines | Respiratory arrest - FATAL |
| Warfarin | NSAIDs | Severe bleeding |
| ACE inhibitor | Potassium-sparing diuretics | Dangerous hyperkalemia |
| QT drugs | Other QT drugs | Torsades - fatal arrhythmia |
| Azathioprine | Allopurinol | Bone marrow failure |
| Sildenafil | Nitrates | Severe hypotension |
| Alcohol | Metronidazole | Disulfiram reaction |
| Methotrexate | NSAIDs | Methotrexate toxicity |
| Digoxin | Amiodarone / verapamil | Digoxin toxicity |
Nursing Safety Checklist Before Giving Any Drug
- Check the full medication list - look at ALL drugs the patient is on
- Flag high-risk drugs - warfarin, digoxin, lithium, methotrexate, MAOIs, opioids, QT-prolonging drugs
- Ask about OTC drugs and herbal supplements - patients often don't volunteer this (St John's Wort is a major CYP inducer that interacts with many drugs)
- Check renal and liver function - many interactions are worse in organ impairment
- Use a drug interaction checker - apps like Lexicomp, Epocrates, or Micromedex are standard in clinical practice
Would you like me to go deeper into any specific combination - such as IV drug compatibilities (what can share the same IV line), or move on to another pharmacology topic like antibiotics or cardiac drugs?
This is a shared conversation. Sign in to Orris to start your own chat.