Diarrhoea
Reading File
Asking for Preferences
Finding Sources
Searching the Web
diarrhoea causes types pathophysiology overview
Reading File
Reading File
Reading File
Loading Image
Excellent content loaded. Now I have comprehensive material from Sleisenger & Fordtran's dedicated diarrhea chapter and Costanzo Physiology. Let me compile the full answer.
Diarrhoea - Overview: Causes, Types & Pathophysiology
Definition
Diarrhoea is a symptom, not a disease. Most patients consider increased fluidity of stool to be its essential characteristic. Formally, it is defined as:
- Stool weight > 200 g/day (the clinical gold standard)
- OR passage of 3 or more loose/watery stools per day
- Acute diarrhoea: lasts < 14 days
- Persistent diarrhoea: lasts 14-30 days
- Chronic diarrhoea: lasts > 4 weeks (affects ~6.6% of the population)
The word itself derives from Greek meaning "to run through."
Normal Intestinal Fluid Balance (Background)
The gut handles enormous fluid volumes daily. Of roughly 9 L of fluid entering the small intestine (from diet + secretions), over 98% is normally absorbed. Diarrhoea results when this balance tips toward net secretion or reduced absorption.
Pathophysiology - The Four Core Mechanisms
1. Osmotic Diarrhoea
Caused by non-absorbable solutes in the intestinal lumen that retain water osmotically.
How it works:
- When solutes that cannot be absorbed remain in the gut lumen, they exert an osmotic force that draws water into the lumen
- This overwhelms the absorptive capacity of the colon
Key features:
- Stops with fasting or stopping the offending agent
- Stool osmotic gap is high (> 125 mOsm/kg)
- Stool osmotic gap = 290 - 2 × (stool [Na+] + stool [K+])
Causes:
| Cause | Example |
|---|---|
| Disaccharidase deficiency | Lactase deficiency (lactose intolerance) - undigested lactose retained in lumen; colonic bacteria further ferment it into more osmotically active particles |
| Malabsorption syndromes | Coeliac disease, short bowel syndrome |
| Osmotic laxatives | Magnesium salts, lactulose, polyethylene glycol |
| Sugar alcohols | Sorbitol, mannitol (in "sugar-free" products) |
2. Secretory Diarrhoea
Caused by excessive active secretion of ions and water by intestinal crypt cells, or failure of villous absorption.
How it works (molecular mechanism):
The diagram below illustrates the key pathway using cholera as the prototype:
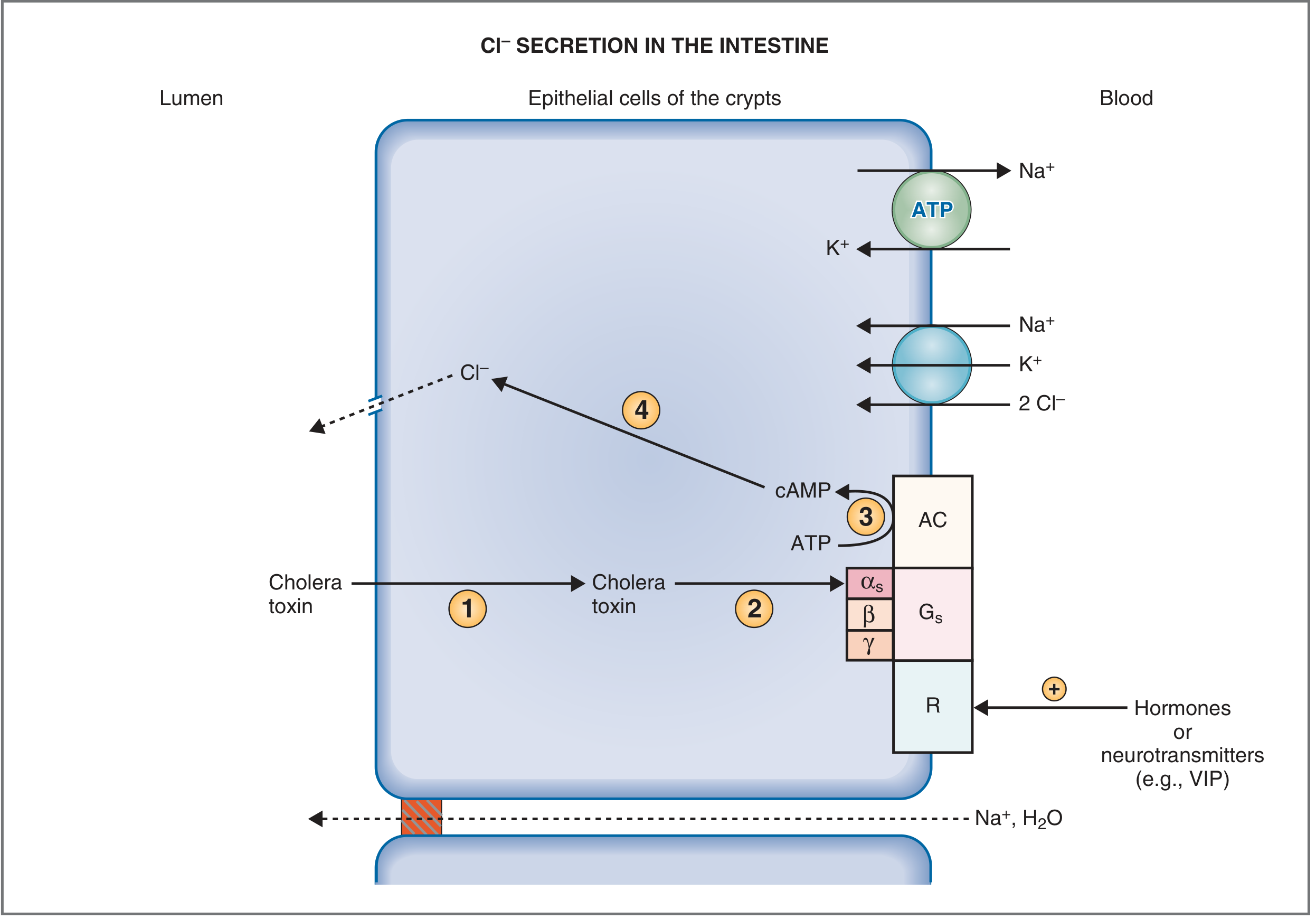
Fig: Mechanism of Cl- and fluid secretion by intestinal crypt epithelial cells (Costanzo Physiology)
Steps:
- Cholera toxin enters crypt cells via the apical membrane
- The A-subunit activates the Gs protein (α-subunit)
- This permanently activates adenylyl cyclase (AC), massively increasing intracellular cAMP
- Elevated cAMP opens CFTR Cl- channels in the apical membrane → Cl- pours into the lumen
- Na+ and water follow passively (paracellularly) → profuse watery diarrhoea
Other secretagogues (VIP, prostaglandins, bile acids) use similar cAMP/cGMP/Ca2+ second-messenger pathways.
Key features:
- Persists with fasting (unlike osmotic diarrhoea)
- Large volumes (may be > 1 L/day)
- Stool osmotic gap is low (< 50 mOsm/kg) - stool electrolytes account for most osmolality
- Isotonic stool
Causes:
| Category | Examples |
|---|---|
| Bacterial toxins | Vibrio cholerae, enterotoxigenic E. coli (ETEC), Staph. aureus |
| Hormone-secreting tumours | VIPoma (Verner-Morrison), carcinoid (serotonin), gastrinoma (Zollinger-Ellison), medullary thyroid carcinoma (calcitonin) |
| Bile acid malabsorption | Terminal ileal disease/resection → bile acids reach colon → stimulate secretion |
| Microscopic colitis | Collagenous/lymphocytic colitis |
| Congenital | Congenital chloridorrhoea (defective Cl-/HCO3- exchanger) |
3. Inflammatory / Exudative Diarrhoea
Caused by mucosal damage and inflammation, leading to protein, blood, and pus loss into the lumen.
How it works:
- Destruction of villous absorptive cells → reduced absorption
- Release of prostaglandins and cytokines → stimulate secretion
- Mucosal ulceration → exudation of protein-rich fluid, RBCs, WBCs
Key features:
- Stool contains blood, mucus, or pus (dysentery pattern)
- Fever and systemic inflammatory signs common
- Fecal leukocytes positive
- Small-volume, frequent stools (if colonic involvement)
Causes:
| Category | Examples |
|---|---|
| Invasive bacteria | Shigella, Salmonella, Campylobacter, C. difficile, EIEC, E. coli O157:H7 |
| Parasites | Entamoeba histolytica |
| IBD | Crohn's disease, ulcerative colitis |
| Ischaemic colitis | |
| Radiation enteritis |
4. Motility-Related Diarrhoea (Decreased Absorptive Contact Time)
Caused by reduced transit time through the gut, preventing adequate absorption.
How it works:
- Rapid transit means luminal contents do not have sufficient contact with the absorptive mucosa
- Can also result from surgical reduction of absorptive surface area
Causes:
| Cause | Example |
|---|---|
| Surgical | Post-gastrectomy (dumping), bowel resection, vagotomy (postvagotomy diarrhoea) |
| Functional | IBS-diarrhoea predominant (IBS-D) |
| Hyperthyroidism | Increased GI motility |
| Diabetic autonomic neuropathy | Disrupted neural control |
| Drugs | Prokinetics, magnesium antacids |
Metabolic Consequences of Diarrhoea
Diarrhoeal fluid is rich in specific electrolytes, so large losses cause predictable disturbances:
| Electrolyte/Fluid | Loss | Consequence |
|---|---|---|
| Water + Na+ | Isotonic ECF loss | Hypovolaemia, hypotension, circulatory collapse |
| HCO3- | High in intestinal secretions | Hyperchloraemic normal anion gap metabolic acidosis |
| K+ | Flow-rate-dependent colonic K+ secretion | Hypokalaemia |
Clinical Classification Summary
| Feature | Osmotic | Secretory | Inflammatory |
|---|---|---|---|
| Volume | Moderate | Large | Small |
| Blood/mucus | No | No | Yes |
| Fasting effect | Stops | Persists | Persists |
| Osmotic gap | High (>125) | Low (<50) | Variable |
| Examples | Lactose intolerance | Cholera, VIPoma | Shigellosis, IBD |
Common Causes by Duration
Acute (< 14 days) - usually infectious:
- Viral: Norovirus, Rotavirus (most common globally in children)
- Bacterial: Salmonella, Campylobacter, Shigella, ETEC, C. difficile
- Parasitic: Giardia lamblia, Cryptosporidium
Chronic (> 4 weeks):
- IBD (Crohn's disease, ulcerative colitis)
- IBS-D (functional)
- Malabsorption (coeliac disease, pancreatic exocrine insufficiency)
- Microscopic colitis
- Endocrine (hyperthyroidism, Addison's, VIPoma, carcinoid)
- Medications (metformin, antibiotics, PPIs, SSRIs)
- Post-surgical (short bowel syndrome, bile acid diarrhoea)
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter on Diarrhea; Costanzo Physiology 7th Edition, pp. 392-393
This is a shared conversation. Sign in to Orris to start your own chat.