Pyelonephritis
Reading File
Finding Sources
Searching PubMed
"pyelonephritis"[MeSH Terms] AND ("treatment" OR "management")
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed to write a comprehensive answer on pyelonephritis.
Pyelonephritis
Pyelonephritis is an infection of the upper urinary tract involving the renal parenchyma and pelvicalyceal system. It is classified as acute or chronic, and distinguished from lower UTI (cystitis) primarily by clinical and anatomical features.
1. Etiology and Pathogenesis
Routes of Infection
- Ascending route (most common): Fecal flora (especially E. coli) colonize the urethra and bladder, then ascend to the kidney. This is facilitated by a short female urethra, which explains the much higher incidence in women of reproductive age.
- Hematogenous route (less common): Bacteremia seeds the kidney; more likely with Staphylococcus aureus and gram-negative organisms in septicemic patients.
Causative Organisms
- E. coli - by far the most common (uropathogenic strains with P-fimbriae that adhere to uroepithelium)
- Klebsiella, Proteus, Enterobacter, Pseudomonas
- Enterococcus (especially in nosocomial/complicated cases)
- Fungi and mycobacteria cause granulomatous interstitial inflammation rather than the usual neutrophilic response
Predisposing Factors
| Factor | Mechanism |
|---|---|
| Vesicoureteral reflux (VUR) | Allows infected urine to ascend; present in 20-40% of children with UTI |
| Urinary tract obstruction | Stasis allows bacterial multiplication (BPH, stones, strictures) |
| Pregnancy | Uterine pressure causes stasis; 20-40% of untreated bacteriuria progresses to pyelonephritis |
| Diabetes mellitus | Increased susceptibility + neurogenic bladder dysfunction |
| Urinary catheterization / instrumentation | Direct introduction of organisms |
| Immunosuppression / immunodeficiency | Impaired bacterial clearance |
| Preexisting renal scarring | Intrarenal obstruction |
2. Pathology
Acute Pyelonephritis - Gross Appearance
One or both kidneys may be affected. The cortical surface shows discrete, yellowish raised abscesses. On cut section, the characteristic pattern is wedge-shaped areas of suppuration (not seen in cystitis) extending from the papilla to the cortex, reflecting the tubular spread of infection.
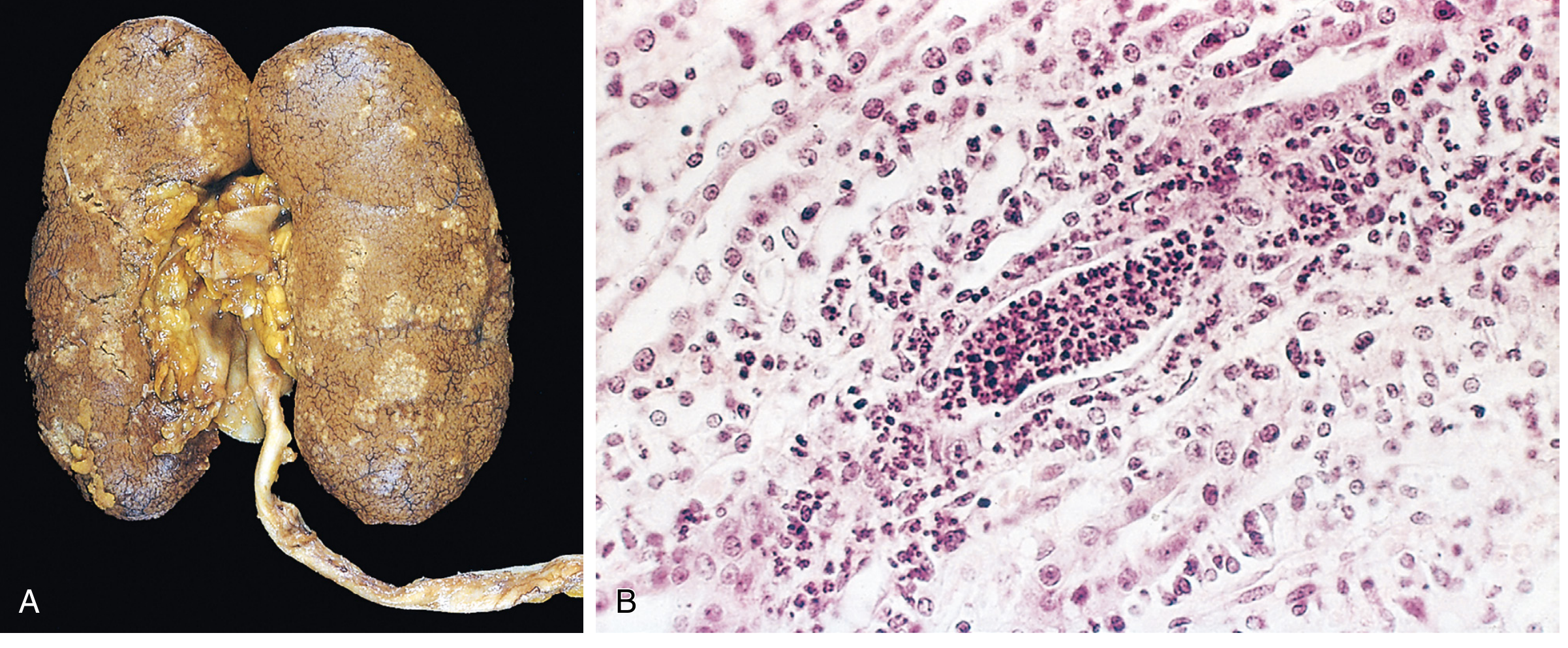
Acute Pyelonephritis - Microscopy
- Neutrophil-rich inflammation initially limited to tubules, then spreading to the interstitium
- Neutrophils extend into collecting ducts - producing WBC (pus) casts in urine (pathognomonic of upper tract disease - casts only form in tubules)
- Glomeruli typically spared in uncomplicated cases
- With obstruction: pus fills the renal pelvis and ureter = pyonephrosis
Complications of Acute Pyelonephritis
- Papillary necrosis: Ischemic + suppurative necrosis of papillary tips. Classic triad of predisposing conditions: diabetes, urinary tract obstruction, sickle cell anemia. Sloughed papillae can obstruct the ureter.
- Renal/perinephric abscess: Liquefaction of parenchyma; may require drainage if ≥3 cm
- Emphysematous pyelonephritis: Gas-forming infection in diabetics (usually E. coli or Klebsiella); life-threatening; diagnosed on CT
- Septicemia/urosepsis: ~10-19% of sepsis cases have a genitourinary source
Healing
After the acute phase, neutrophils are replaced by macrophages, plasma cells, and lymphocytes, eventually forming irregular cortical scars (fibrous depressions). Microscopically: tubular atrophy, interstitial fibrosis, lymphocytic infiltrate in a patchy, jigsaw pattern with intervening preserved parenchyma. The scar is always associated with inflammation and deformation of the underlying calyx/pelvis.
Chronic Pyelonephritis
- Chronic tubulointerstitial inflammation and calyceal/pelvic scarring - the hallmark that distinguishes it from other chronic interstitial nephritides
- Reflux-associated (most common): Recurrent ascending infections via VUR; predominantly affects upper and lower poles where intrarenal reflux is highest
- Obstructive: Bilateral when from congenital urethral anomalies; may affect the entire kidney
- Microscopically: "thyroidization" of tubules (colloid-like eosinophilic casts), periglomerular fibrosis, glomerulosclerosis secondary to loss of renal mass
- End result: progressive CKD
3. Clinical Features
Acute Pyelonephritis
- Sudden onset of flank pain / costovertebral angle (CVA) tenderness
- Fever, chills, rigors
- Nausea, vomiting, malaise (systemic symptoms)
- May or may not have concomitant lower urinary tract symptoms (dysuria, frequency, urgency)
- Urine culture: ≥10⁵ CFU/mL (positive urine culture required for diagnosis)
A missed diagnosis of cystitis is unlikely to lead to patient deterioration; in contrast, missed pyelonephritis could lead to untreated sepsis. - Tintinalli's Emergency Medicine
Special Populations - Watch for Atypical Presentations
- Spinal cord injury: No flank pain; may manifest as increased spasticity, autonomic dysreflexia, sense of unease
- Elderly: Altered mental status, weakness, malaise (fever/pain may be absent)
- Immunocompromised: Signs of infection may be blunted
4. Diagnosis
Urinalysis / Dipstick
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Leukocyte esterase | 62-98% | 55-96% | Detects pyuria |
| Urine nitrite | ~50% | >90% | Only detects bacteria that reduce nitrates (E. coli, coliforms); NOT Enterococcus, Pseudomonas |
| Pyuria >5 WBC/HPF (centrifuged) | Moderate | Moderate | May be absent in obstructed kidney or leukopenia |
- WBC casts (pus casts) on microscopy = upper tract disease (formed only in tubules) - this differentiates pyelonephritis from cystitis
- Urine culture is the diagnostic gold standard; negative nitrite does NOT exclude infection
Blood Tests
- CBC: leukocytosis with left shift
- Blood cultures: obtain in hospitalized/severe cases (bacteremia in 15-30%)
- Creatinine/BMP: AKI occurs in up to 25% of gestational pyelonephritis cases
Imaging
- Not routinely required for uncomplicated cases
- CT (non-contrast then contrast): Best for complications - renal/perinephric abscess, emphysematous pyelonephritis, papillary necrosis, obstruction
- Ultrasound: For pregnancy (avoids radiation); identifies obstruction, hydronephrosis, abscess; less sensitive than CT for early parenchymal changes
- Indications: failure to improve after 48-72h of antibiotics, recurrent pyelonephritis, suspected abscess, diabetes
5. Treatment
Decision: Inpatient vs. Outpatient
Admit if:
- Severely ill (high fever, rigors, prostration)
- Unable to tolerate oral fluids/medications
- Pregnancy
- Diabetes or immunocompromise
- Suspected complication (abscess, obstruction, emphysematous pyelonephritis)
- Unclear diagnosis
Antibiotic Regimens
Oral (outpatient - uncomplicated):
- Ciprofloxacin 500 mg twice daily × 5-7 days ← first choice where resistance <20%
- Levofloxacin 750 mg once daily × 5-7 days
- If fluoroquinolone resistance suspected: TMP-SMX DS, cefpodoxime, or amoxicillin-clavulanate × 7-14 days
- Note: nitrofurantoin and fosfomycin do NOT achieve adequate renal tissue levels and are not appropriate for pyelonephritis
Parenteral (inpatient):
- Initial empiric IV: aminoglycoside (gentamicin) ± ampicillin; or IV ceftriaxone
- Transition to oral at 24-48h once clinically improved
- Total duration: 7-14 days (5-7 days adequate for fluoroquinolones)
- Severe complicated: IV meropenem 1g q8h, or piperacillin-tazobactam, or IV plazomicin 15 mg/kg once daily - Goldman-Cecil Medicine
Pregnancy-Specific Treatment
- Hospital admission recommended (outpatient management acceptable only for mild cases)
- IV antibiotics until afebrile, then oral to complete 14 days
- Safe choices: cephalosporins, penicillins (avoid fluoroquinolones and tetracyclines in pregnancy)
- Prophylactic suppressive antibiotics until delivery to prevent recurrence and reduce risk of preterm labor
- Recurrence rate: 6-8%; AKI complicates up to 25% of gestational pyelonephritis
- Associated with IUGR, premature labor, sepsis - NKF Primer on Kidney Diseases, 8e
Complicated Pyelonephritis / Abscesses
- Renal/perinephric abscesses ≥3 cm should be drained
- 4-6 weeks total antibiotics for abscess
- If obstructed + infected and not responding to antibiotics: percutaneous nephrostomy
- Emphysematous pyelonephritis: usually requires nephrectomy in addition to antibiotics
6. Chronic Pyelonephritis and Reflux Nephropathy
Chronic pyelonephritis results from repeated renal inflammation (usually due to VUR or obstruction) producing progressive renal scarring. It is the second most common cause of end-stage renal disease in children (after glomerulonephritis in some populations).
Key features:
- Asymmetric, coarse, irregular scarring (especially at poles) on imaging
- Clubbing/blunting of calyx underlying each scar (calyceal deformity is required to diagnose chronic pyelonephritis radiologically)
- May progress to hypertension and CKD
- "Thyroidization" of tubules on histology (colloid-like casts)
7. Summary Table: Acute vs. Chronic Pyelonephritis
| Feature | Acute | Chronic |
|---|---|---|
| Onset | Sudden | Insidious |
| Pathology | Neutrophilic tubulointerstitial inflammation, abscesses | Fibrosis, tubular atrophy, calyceal scarring |
| WBC casts | Present (neutrophilic) | Occasional |
| Gross appearance | Yellowish abscesses, cortical surface | Coarse irregular scars (polar) |
| Key predisposing factor | VUR, obstruction, DM, catheterization | VUR (reflux nephropathy), obstruction |
| Complication | Urosepsis, papillary necrosis, abscess | CKD, hypertension, ESRD |
Recent evidence note: A 2025 living systematic review and meta-analysis (PMID 40228579) supports shorter antibiotic courses for pyelonephritis in line with current guidelines (5-7 days for fluoroquinolones). A 2025 network meta-analysis (PMID 39817442) evaluated efficacy across treatment options for complicated UTI including acute pyelonephritis; no major changes to standard recommendations identified.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine International Edition; Tintinalli's Emergency Medicine; Comprehensive Clinical Nephrology 7e; NKF Primer on Kidney Diseases 8e; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.