how central chemoreceptor respond to increase in co2
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
I now have everything needed for a thorough, textbook-based answer. Here is the complete response:
How Central Chemoreceptors Respond to Increased CO2
Location
Central chemoreceptors sit within the brain parenchyma, predominantly on the anterolateral (ventrolateral) surface of the medulla oblongata - including the retrotrapezoid nucleus (RTN), medullary raphe nuclei, nucleus ambiguus, nucleus tractus solitarius (NTS), and the locus coeruleus. They are bathed in brain extracellular fluid (BECF) and CSF.
The Core Mechanism (Step by Step)
Step 1 - CO2 crosses the blood-brain barrier (BBB)
The BBB is highly permeable to small neutral molecules like CO2, but nearly impermeable to ions (H+, HCO3-, Na+, Cl-). So when arterial PCO2 rises, CO2 freely diffuses across the BBB into the BECF and CSF. Importantly, H+ and HCO3- cannot cross as readily.
Step 2 - CO2 is hydrated to H+ in the CSF/BECF
CO2 + H2O ↔ H+ + HCO3-
This reaction (catalyzed by carbonic anhydrase) lowers the pH of the CSF and BECF. Because the CSF/BECF has far less protein than blood plasma, its non-bicarbonate buffering power is much lower - so for a given rise in PCO2, the pH drop in the CSF is larger and faster than in blood. This amplifies the stimulus.
Step 3 - Chemoreceptors detect the H+ rise (not CO2 directly)
The actual stimulus to central chemoreceptors is the fall in pH (rise in [H+]) in the BECF/CSF - not CO2 per se. Evidence: perfusing the cerebral ventricles with an acidic solution (even at normal PCO2) increases ventilation; conversely, metabolic acidosis (low pH at fixed PCO2) has a much weaker ventilatory effect because H+ cannot cross the BBB as readily.
Step 4 - Neuronal activation and output
Chemosensitive neurons (many are serotonergic; others are glutamatergic) are excited by the local acidosis. GABAergic neurons are inhibited. These neurons project to the medullary respiratory centers (central pattern generator), which then increase the rate and depth of breathing (alveolar ventilation) to blow off excess CO2 and restore pH.
Ventilatory Response Curve
This is the normal CO2-ventilation response curve:
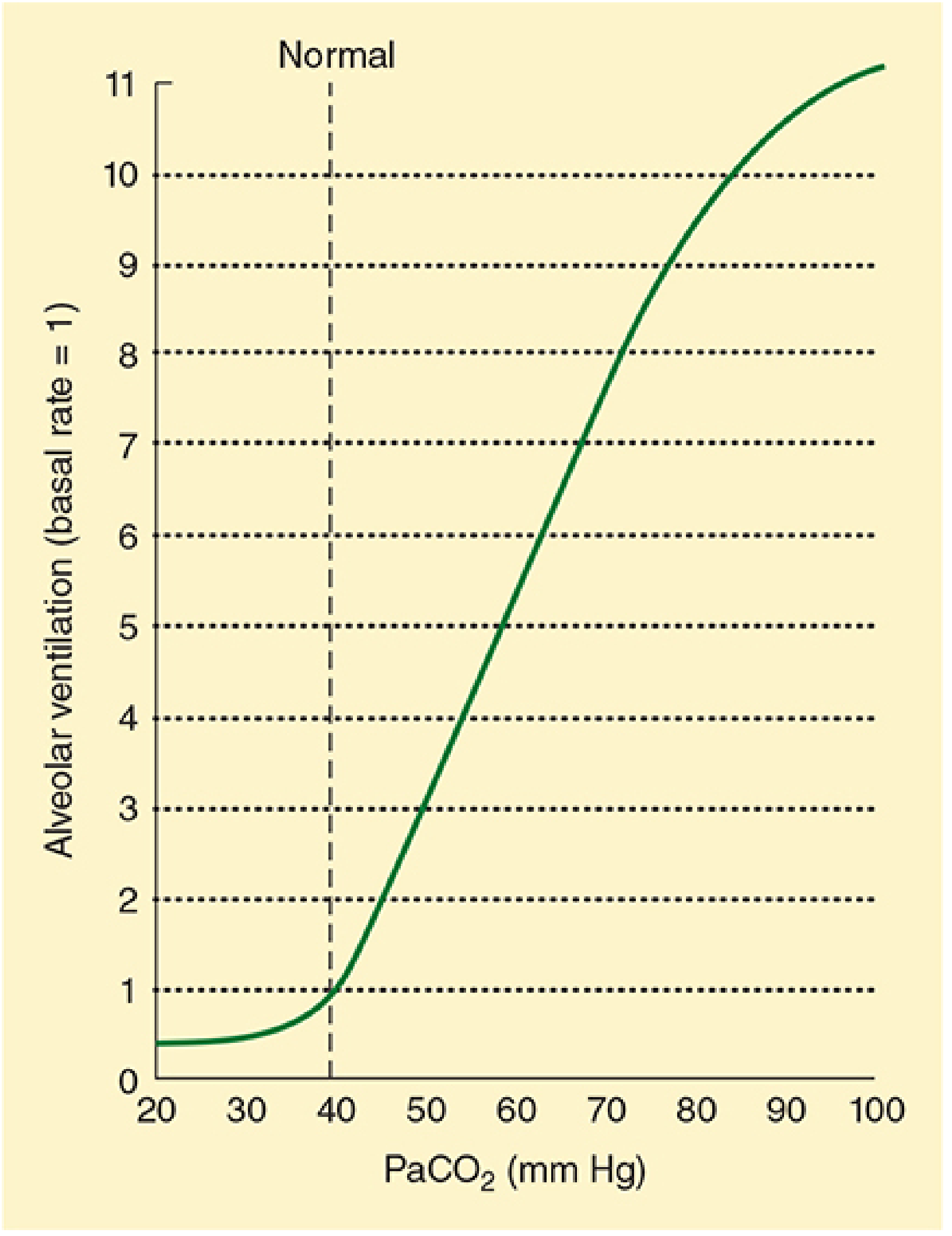
Key features:
- The relationship between PaCO2 and minute ventilation is nearly linear over the physiological range (40-70 mmHg)
- A rise in PaCO2 from 40 to ~45 mmHg (just ~12.5% increase) doubles ventilation - showing extreme sensitivity
- The full response takes 5-10 minutes to develop (due to delay in pH change at the chemosensory site, chemotransduction time, and CPG response lag)
- At very high PaCO2 (>80-100 mmHg), the response reverses - CO2 narcosis causes CNS depression and respiratory failure
Why Central > Peripheral for CO2
| Feature | Central Chemoreceptors | Peripheral Chemoreceptors |
|---|---|---|
| Location | Ventrolateral medulla | Carotid & aortic bodies |
| Primary stimulus | CSF/BECF [H+] (from CO2) | PaO2, PaCO2, arterial pH |
| Response to hypercapnia | Dominant (~70-80% of response) | Contributes ~20-30% |
| Response to hypoxia | Depressed by hypoxia | Stimulated by hypoxia |
| Speed | Slower (5-10 min full response) | Faster |
Why Metabolic Acidosis Has a Weaker Effect
Even though metabolic acidosis lowers blood pH, the H+ ions cannot freely cross the BBB. The choroid plexus actively maintains CSF pH. So metabolic acid-base disturbances alter steady-state brain pH only 10-35% as much as equivalent respiratory disturbances. This is why ventilation correlates with BECF pH, not arterial blood pH per se.
Compensation Over Time
With chronic hypercapnia, the choroid plexus and BBB actively transport HCO3- into the CSF, partially restoring CSF pH. This is the metabolic compensation to respiratory acidosis - it explains why patients with chronic CO2 retention have a blunted ventilatory drive over days.
Sources:
- Medical Physiology (Boron & Boulpaep), pp. 1065-1066 - detailed mechanism of BBB permeability and BECF acidosis
- Morgan and Mikhail's Clinical Anesthesiology, p. 972-973 - clinical overview of central vs. peripheral sensors and CO2-narcosis threshold
- Medical Physiology, N32-19/N32-22 - RTN neurons, serotonergic chemoreceptors, and SIDS implications
why central chemoreceptors are depressed by hypoxia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
why central chemoreceptors depressed by hypoxia mechanism adenosine neuronal metabolism
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC4802370
I now have enough from the textbooks and supplementary sources to give a thorough, accurate answer. Here it is:
Why Central Chemoreceptors Are Depressed by Hypoxia
This is one of the most important contrasts in respiratory physiology - and the answer operates at several levels.
1. The Key Experimental Proof
When peripheral chemoreceptors are denervated in animals and the animal is then made hypoxic, hypoxia actually depresses respiratory output rather than stimulating it. This shows that the net central effect of hypoxia is inhibitory - the only reason hypoxia normally increases breathing is because peripheral chemoreceptors (carotid bodies) overcome and dominate this central depression.
"In an animal with denervated peripheral chemoreceptors, hypoxia actually depresses respiratory output."
- Medical Physiology (Boron & Boulpaep), p. 1070
2. Mechanisms of Central Depression by Hypoxia
There are three overlapping mechanisms:
A. Direct Neuronal Metabolic Failure (Primary mechanism)
The medullary neurons that act as central chemoreceptors (serotonergic neurons in raphe, RTN neurons, NTS neurons) are highly aerobic and oxygen-dependent. When O2 drops:
- Mitochondrial oxidative phosphorylation is impaired
- ATP production falls
- Neurons cannot maintain their membrane potential or firing rates
- The result is generalised CNS depression, just as hypoxia causes confusion and loss of consciousness at the cortical level - the brainstem is not immune
This is the same mechanism by which severe hypoxia causes loss of consciousness - neurons simply fail when deprived of oxygen.
B. Adenosine Release - The "Sleep Chemical" Effect
During hypoxia, ATP breakdown accelerates and adenosine accumulates in brain tissue. Adenosine is a potent neuroinhibitor - it acts via A1 receptors to:
- Hyperpolarise neurons
- Reduce neurotransmitter release
- Suppress firing of medullary chemosensitive neurons
This is why caffeine (an adenosine receptor antagonist) is used clinically in neonatal apnea - it blocks this adenosine-mediated central respiratory depression.
C. Hypoxia Does Not Change CSF [H+] the Way CO2 Does
Central chemoreceptors detect H+ in the BECF/CSF, not O2 directly. Hypoxia alone:
- Does not appreciably raise PCO2 (in fact, hyperventilation from peripheral receptors lowers PCO2)
- If anything, the hypocapnia induced by peripheral-chemoreceptor-driven hyperventilation raises CSF pH (less H+)
- Less H+ = less stimulus to the central chemoreceptors
So even if the neurons were fully functional, falling CO2 (from reflex hyperventilation) removes the acid stimulus that central chemoreceptors depend on.
3. The Biphasic Hypoxic Ventilatory Response
This explains the classic two-phase response to sustained hypoxia:
| Phase | Time | Driver | What happens |
|---|---|---|---|
| Early stimulation | 0-2 min | Peripheral carotid bodies (O2-sensitive) | Rapid increase in ventilation |
| Late depression | 2-20 min | Central depression overrides | Ventilation falls back partway toward baseline |
The late "roll-off" (hypoxic ventilatory decline) reflects the gradual dominance of central neuronal depression overcoming the peripheral drive.
4. Contrast with Peripheral Chemoreceptors
| Feature | Central Chemoreceptors | Peripheral (Carotid Bodies) |
|---|---|---|
| Response to hypoxia | Depressed | Strongly stimulated |
| Primary stimulus | CSF/BECF H+ (from CO2) | PaO2, pH, PCO2 |
| Why different? | Metabolically vulnerable neurons; no O2 sensor | Glomus (type I) cells have specialized O2-sensing via TASK channels and HIF pathways |
| Hypoxia + CO2 interaction | Already depressed; CO2 signal attenuated | Hypoxia potentiates CO2 response (synergistic) |
5. Clinical Relevance
-
Chronic CO2 retainers (COPD): When central chemoreceptors adapt to chronic hypercapnia (CSF pH normalises), hypoxic drive from peripheral receptors becomes the primary breathing stimulus. Giving high-flow O2 removes this drive → hypoventilation → CO2 narcosis → death. This is why careful O2 titration (target SpO2 88-92%) is used in these patients.
-
Neonatal apnea: Infants have an exaggerated central depression to hypoxia (immature serotonergic neurons) - this is why caffeine/theophylline are used to block adenosine and stimulate the respiratory center.
-
SIDS: Abnormalities of serotonin neurons in the medullary raphe (the same neurons that are central chemoreceptors) may cause an exaggerated inability to respond to hypoxia during sleep.
Sources:
- Medical Physiology (Boron & Boulpaep), pp. 1069-1070 - denervation experiments proving central depression
- Morgan & Mikhail's Clinical Anesthesiology, p. 972-973 - clinical overview; "central chemoreceptor activity is depressed by hypoxia"
- Cummings Otolaryngology, p. 3498 - biphasic response and neonatal hypoxic depression
- Central Chemoreceptors: Locations and Functions, PMC4802370 - adenosine/ATP and glial mechanisms
This is a shared conversation. Sign in to Orris to start your own chat.