Nascis regimen 10 marks pg Orthopaedic answer include flow chart and images
Reading File
Finding Sources
Finding Sources
Searching PubMed
NASCIS methylprednisolone spinal cord injury
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching the Web
NASCIS regimen methylprednisolone spinal cord injury protocol flowchart 24 hours 48 hours
Loading Image
Loading Image
I now have all the content needed for a comprehensive 10-mark PG Orthopaedics answer. Let me compile the full answer.
NASCIS Regimen in Acute Spinal Cord Injury
Introduction
The National Acute Spinal Cord Injury Studies (NASCIS) were a series of three landmark prospective, double-blind, randomized controlled trials conducted in the 1990s that evaluated the role of high-dose methylprednisolone sodium succinate (MPSS) in acute blunt spinal cord injury (SCI). They remain the most comprehensive pharmacological trials in the history of SCI research.
Rationale / Mechanism of Action
Methylprednisolone is believed to exert neuroprotection via:
- Inhibition of free-radical-induced lipid peroxidation (primary mechanism) - prevents secondary injury cascade
- Increases spinal cord blood flow
- Increases extracellular calcium levels
- Prevents loss of potassium from injured cord tissue
- Crosses cell membranes more rapidly and completely than other steroids (hence preferred over dexamethasone)
The secondary injury cascade after primary SCI proceeds as:
Mechanical trauma → Local edema → Cellular apoptosis → Disorganized fibrosis → Hindered neuronal signaling & axonal regrowth
Pharmacologic therapy aims to halt or reverse this cascade.
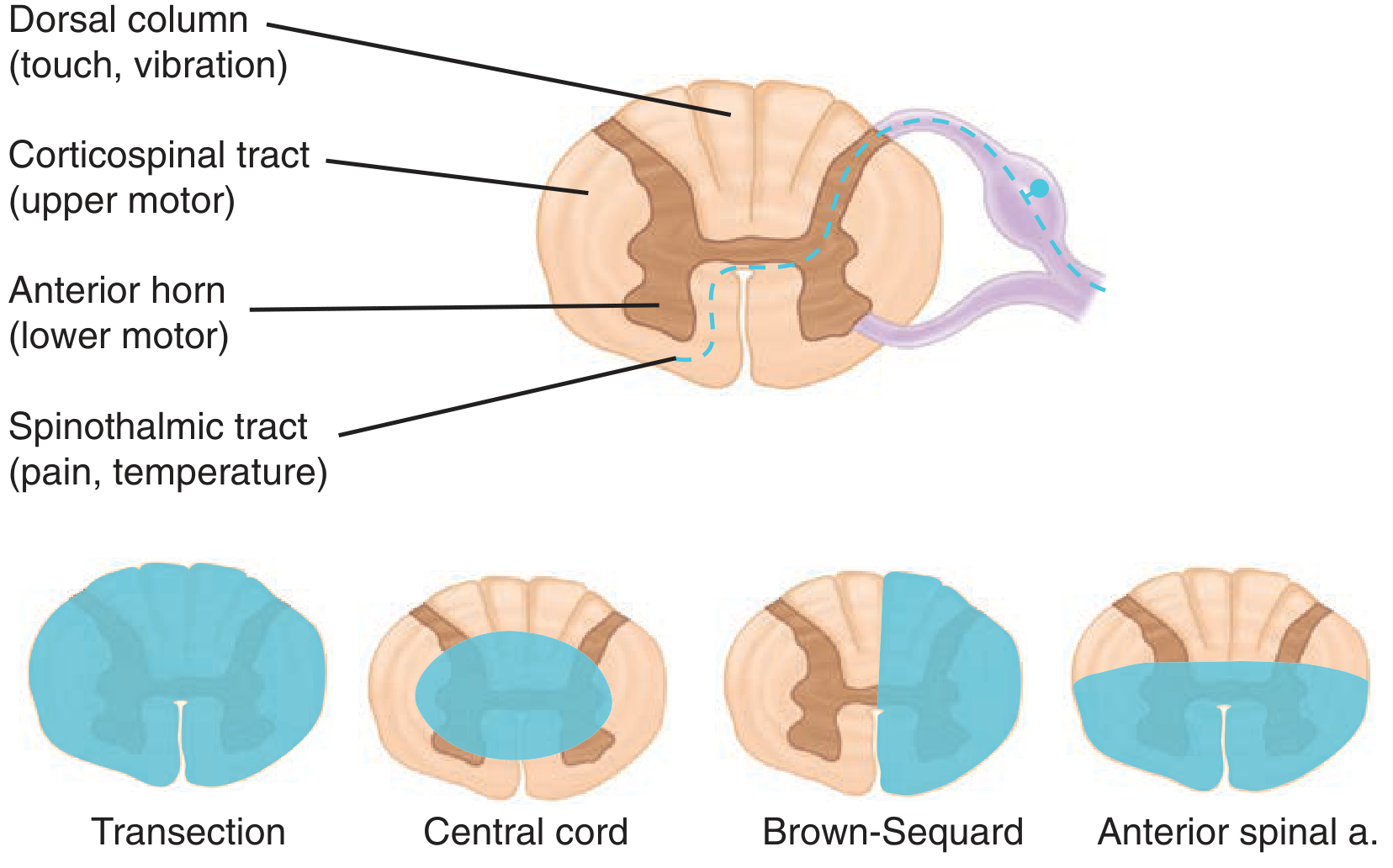
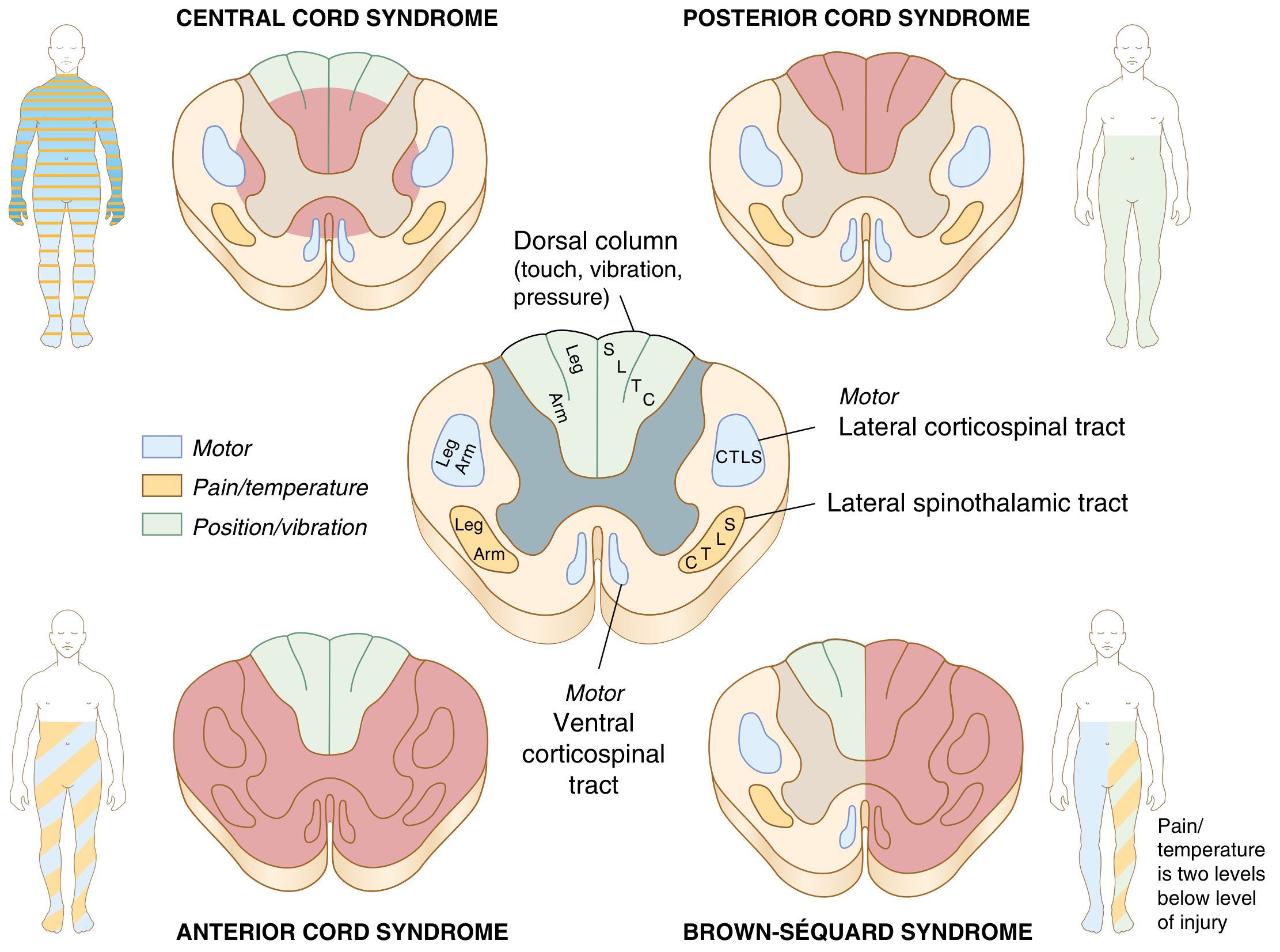
Spinal Cord Anatomy - Relevant to SCI Understanding
The Three NASCIS Trials
| Trial | Comparison Arms | n | Primary Result | Post-Hoc Finding |
|---|---|---|---|---|
| NASCIS I | Low-dose MPSS (100 mg bolus/day) vs High-dose MPSS (1000 mg bolus/day) | 330 | No difference in outcomes | - |
| NASCIS II | High-dose MPSS vs Naloxone vs Placebo | 427 | Negative (primary outcome) | Modest motor improvement if MPSS given within 8 hours |
| NASCIS III | MPSS 24h vs MPSS 48h vs Tirilazad mesylate 48h | 499 | Negative (primary outcome) | Extended 48h regimen improved outcomes if started 3-8 hours post injury |
NASCIS II Protocol (The Classic Regimen)
Indications:
- Blunt trauma with neurologic deficit referable to the spinal cord
- Treatment started within 8 hours of injury
NASCIS II Dosing Protocol
┌─────────────────────────────────────────────────────────────┐
│ NASCIS II PROTOCOL │
│ │
│ STEP 1: Loading Bolus │
│ Methylprednisolone 30 mg/kg IV over 15 minutes │
│ ↓ │
│ STEP 2: Pause │
│ Wait 45 minutes │
│ ↓ │
│ STEP 3: Maintenance Infusion │
│ Methylprednisolone 5.4 mg/kg/hr IV for 23 hours │
│ │
│ TOTAL DURATION = 24 hours │
└─────────────────────────────────────────────────────────────┘
NASCIS III Protocol (Time-Stratified Regimen)
NASCIS III refined the duration based on time from injury:
FLOWCHART: NASCIS Regimen Decision Algorithm
┌─────────────────────────────────────────────────────────────────────┐
│ ACUTE BLUNT SPINAL CORD INJURY │
│ (Neurologic deficit present) │
└───────────────────────────┬─────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ SCREEN FOR CONTRAINDICATIONS │
│ │
│ ABSOLUTE CONTRAINDICATIONS: │
│ • Penetrating wound (esp. gunshot) │
│ • Injury > 8 hours old │
│ • Peripheral nerve / root injury (brachial plexus, cauda equina) │
│ • Age < 13 years │
│ • Pregnancy │
│ • Concomitant active infection │
│ • Uncontrolled diabetes mellitus │
└───────────────────────────┬─────────────────────────────────────────┘
│
No contraindication?
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ ADMINISTER LOADING BOLUS (BOTH ARMS) │
│ Methylprednisolone 30 mg/kg IV over 15 minutes │
│ Then wait 45 minutes (pause phase) │
└───────────────────────────┬─────────────────────────────────────────┘
│
▼
┌───────────────────────────────┐
│ TIME SINCE INJURY? │
└───────┬───────────────┬───────┘
│ │
< 3 hours 3 - 8 hours
│ │
▼ ▼
┌───────────────┐ ┌───────────────────┐
│ NASCIS II │ │ NASCIS III │
│ 24-hour arm │ │ 48-hour arm │
│ │ │ │
│ MPSS 5.4 mg/ │ │ MPSS 5.4 mg/ │
│ kg/hr x 23h │ │ kg/hr x 47h │
└───────┬───────┘ └─────────┬─────────┘
│ │
▼ ▼
Total = 24 hours Total = 48 hours
Summary of Dosing
| Parameter | Value |
|---|---|
| Loading bolus dose | 30 mg/kg methylprednisolone IV |
| Bolus infusion duration | Over 15 minutes |
| Pause between bolus & maintenance | 45 minutes |
| Maintenance infusion rate | 5.4 mg/kg/hr IV |
| If started < 3 hours after injury | Continue maintenance for 23 hours (total = 24h) |
| If started 3-8 hours after injury | Continue maintenance for 47 hours (total = 48h) |
| If > 8 hours after injury | Do NOT give - not beneficial and potentially harmful |
Tirilazad Mesylate (NASCIS III, Third Arm)
- A 21-aminosteroid (lazaroid) - potent inhibitor of lipid peroxidation without glucocorticoid activity
- Given at 2.5 mg/kg IV every 6 hours for 48 hours (after the standard MPSS bolus)
- Post-hoc analysis: similar efficacy to 24-hour MPSS if started within 3 hours
- Advantage: Fewer infectious complications than 48-hour MPSS
- Current status: Not widely adopted; considered equivalent but not superior
Complications of High-Dose MPSS
These were documented in all three NASCIS trials and are the primary reason the regimen remains controversial:
| Complication | Significance |
|---|---|
| Severe sepsis | Significantly higher in 48h arm |
| Severe pneumonia | Significantly higher in 48h arm |
| Wound infection and delayed healing | Increased risk |
| Deep vein thrombosis / Pulmonary embolism | Increased risk |
| GI bleeding / peptic ulceration | Requires GI prophylaxis |
| Hyperglycemia | Requires monitoring |
| Death | No significant difference (p = 0.97) |
GI prophylaxis (PPI/H2 blocker) should always be co-administered with the NASCIS regimen.
Criticisms of the NASCIS Trials
- Post-hoc subgroup analysis - primary outcomes were negative; benefits only emerged in subgroups defined after data collection
- Artificiality of the 3-hour and 8-hour time windows - methodologically questioned
- Imbalance in injury severity between treatment groups
- Small effect size for neurologic improvement vs large complication burden
- Multiple reanalyses by independent authors failed to replicate the significance
Current Guidelines (2025 Status)
| Organization | Recommendation |
|---|---|
| AANS/CNS 2013 | Recommended AGAINST methylprednisolone use in acute SCI |
| AOSpine / AANS/CNS (recent) | Weak evidence - 24h infusion may be offered as an option within 8 hours; 48h infusion is not recommended |
| Rockwood & Green (2025) | Use only in carefully selected patients after informed discussion of risks and benefits |
Key quote from AANS/CNS 2013: "There is no consistent or compelling medical evidence of any beneficial effect of methylprednisolone in acute SCI."
Despite this, some centers continue use due to medicolegal concerns - surveys show the majority of SCI patients still prefer to receive MPSS even for small potential benefits.
Memory Aid
"30-45-5.4" Rule:
- 30 mg/kg bolus
- 45 minute pause
- 5.4 mg/kg/hr maintenance
"3 and 8" Rule:
- Within 3 hours → 24-hour regimen
- 3 to 8 hours → 48-hour regimen
- Beyond 8 hours → Do NOT give
Quick Summary Table
| Feature | NASCIS II | NASCIS III |
|---|---|---|
| Year | 1990 | 1997 |
| Arms | MPSS vs Naloxone vs Placebo | MPSS 24h vs MPSS 48h vs Tirilazad 48h |
| n | 427 | 499 |
| Positive primary outcome | No | No |
| Key post-hoc finding | <8h → better motor | 3-8h → 48h arm better at 6 months |
| Window for 24h regimen | <8h (and <3h per NASCIS III) | <3h |
| Window for 48h regimen | - | 3-8h |
Sources:
- Miller's Review of Orthopaedics, 9th Edition, pp. 791-792
- Rockwood and Green's Fractures in Adults, 10th Edition (2025), pp. 2418-2420
- Tintinalli's Emergency Medicine, Comprehensive Study, pp. 1754-1755 (Table 258-8)
- Schwartz's Principles of Surgery, 11th Edition, p. 1874
- Bracken MB et al. NASCIS III. JAMA. 1997;277(20):1597-604. PMID: 9168289
This is a shared conversation. Sign in to Orris to start your own chat.