part 4 oncology and hematology from harrisons section 1 neoplastic disorders from chapter 73 to 100 teach me every thing i need to know from harrisons and add some images and mneumonics if u can so i can become the best doctor
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is your complete, high-yield study guide for Harrison's Part 4: Oncology and Hematology, Section 1: Neoplastic Disorders, Chapters 73-100 (22nd Edition, 2025).
🏥 HARRISON'S ONCOLOGY & HEMATOLOGY: CHAPTERS 73–100
Your Complete Study Guide — Become the Best Doctor
CHAPTER 73 — Approach to the Patient with Cancer
The Big Picture
- Cancer causes 1 in 4 deaths in the USA
- 2024: ~2 million new cases; ~612,000 deaths
- ~2/3 of patients are now cured with modern treatment
Top Cancers by Incidence
| Males | Females |
|---|---|
| Prostate (29%) | Breast (32%) |
| Lung (11%) | Lung (12%) |
| Colorectal (8%) | Colorectal (7%) |
Mnemonic for top causes of cancer DEATH in males: "Lung Prostate Colon Pancreas" (LPCP)
The Physician's Role
- Take cancer diagnosis as seriously as end-stage heart failure — the median survival of pancreatic cancer (~8 months) equals symptomatic aortic stenosis with CHF, but the psychological impact is categorically different
- The patient feels the whole self is diseased, not just an organ
- Psychosocial, functional, and existential dimensions must be addressed
Performance Status (ECOG Scale)
| Grade | Description |
|---|---|
| 0 | Fully active |
| 1 | Restricted in strenuous activity, ambulatory |
| 2 | Ambulatory, capable of self-care, up >50% of day |
| 3 | Limited self-care, confined to bed >50% of day |
| 4 | Completely disabled |
Mnemonic: "0-Okay, 1-Limited, 2-Some help, 3-Mostly bed, 4-Fully bed"
CHAPTER 74 — Cancer Epidemiology and Prevention
Key Concepts
- Carcinogenesis is a multistep process over years: initiation → promotion → progression
- Both environmental and genetic factors interact
- The leading preventable cause of cancer is tobacco (responsible for ~30% of all cancer deaths)
Attributable Risks
| Factor | % of Cancer Deaths |
|---|---|
| Tobacco | ~30% |
| Diet/Obesity | ~30% |
| Infections | ~5-10% |
| Alcohol | ~3-4% |
CHAPTER 75 — Prevention and Early Detection of Cancer
Chemoprevention Highlights
| Agent | Cancer Prevented | Notes |
|---|---|---|
| Tamoxifen/Raloxifene | Breast (ER+) | 50% risk reduction in high-risk women |
| Finasteride | Prostate | Reduces incidence but may shift grade |
| NSAIDs/COX-2 inhibitors | Colorectal | Polyp regression, not yet standard |
| HPV vaccine | Cervical, anal, oropharyngeal | Girls AND boys |
| HBV vaccine | Hepatocellular carcinoma |
Screening Tests: The 4 Numbers
Sensitivity = TP/(TP+FN) — "How good at catching disease"
Specificity = TN/(TN+FP) — "How good at ruling out disease"
PPV depends on prevalence — low prevalence → low PPV even with good test
⚠️ For rare cancers in general population, even high-sensitivity tests have poor PPV!
Key Screening Recommendations (Harrison 22e)
| Cancer | Test | Who/When |
|---|---|---|
| Colorectal | Colonoscopy/FIT | Age 45-75 |
| Breast | Mammogram | Age 40-74 annually |
| Cervical | Pap + HPV | Age 21-65 every 3-5 yrs |
| Lung | Low-dose CT | Age 50-80, 20+ pack-yr history |
| Prostate | PSA (shared decision) | Age 50+ (45 high-risk) |
Biases in Screening Studies
- Lead-time bias — detecting early but not changing death date
- Length bias — screening catches slow-growing, less lethal tumors
- Overdiagnosis — finding tumors that would never cause symptoms
- Selection bias — healthier people get screened
Mnemonic: "LLOS" = Lead-time, Length, Overdiagnosis, Selection
CHAPTER 76 — Cancer Genetics
Two Hit Hypothesis (Knudson)
- Two mutations needed to inactivate a tumor suppressor gene
- Hereditary cancers: first hit in germline (inherited), second hit somatic
- Sporadic cancers: both hits somatic
Oncogenes vs Tumor Suppressors
| Oncogenes | Tumor Suppressors | |
|---|---|---|
| Mutation type | Gain-of-function | Loss-of-function |
| Inheritance | Dominant | Recessive (2 hits) |
| Examples | RAS, MYC, HER2, BCR-ABL | TP53, RB1, APC, BRCA1/2 |
| Analogy | Stuck "accelerator" | Broken "brake" |
Mnemonic: "Oncogenes = ON stuck = Dominant; Suppressors = need both OFF = Recessive"
Key Hereditary Cancer Syndromes
| Syndrome | Gene | Cancers |
|---|---|---|
| Hereditary Breast/Ovarian | BRCA1/2 | Breast, ovary, prostate, pancreas |
| Lynch syndrome (HNPCC) | MLH1, MSH2, MSH6, PMS2 | Colorectal, endometrial, ovarian, gastric |
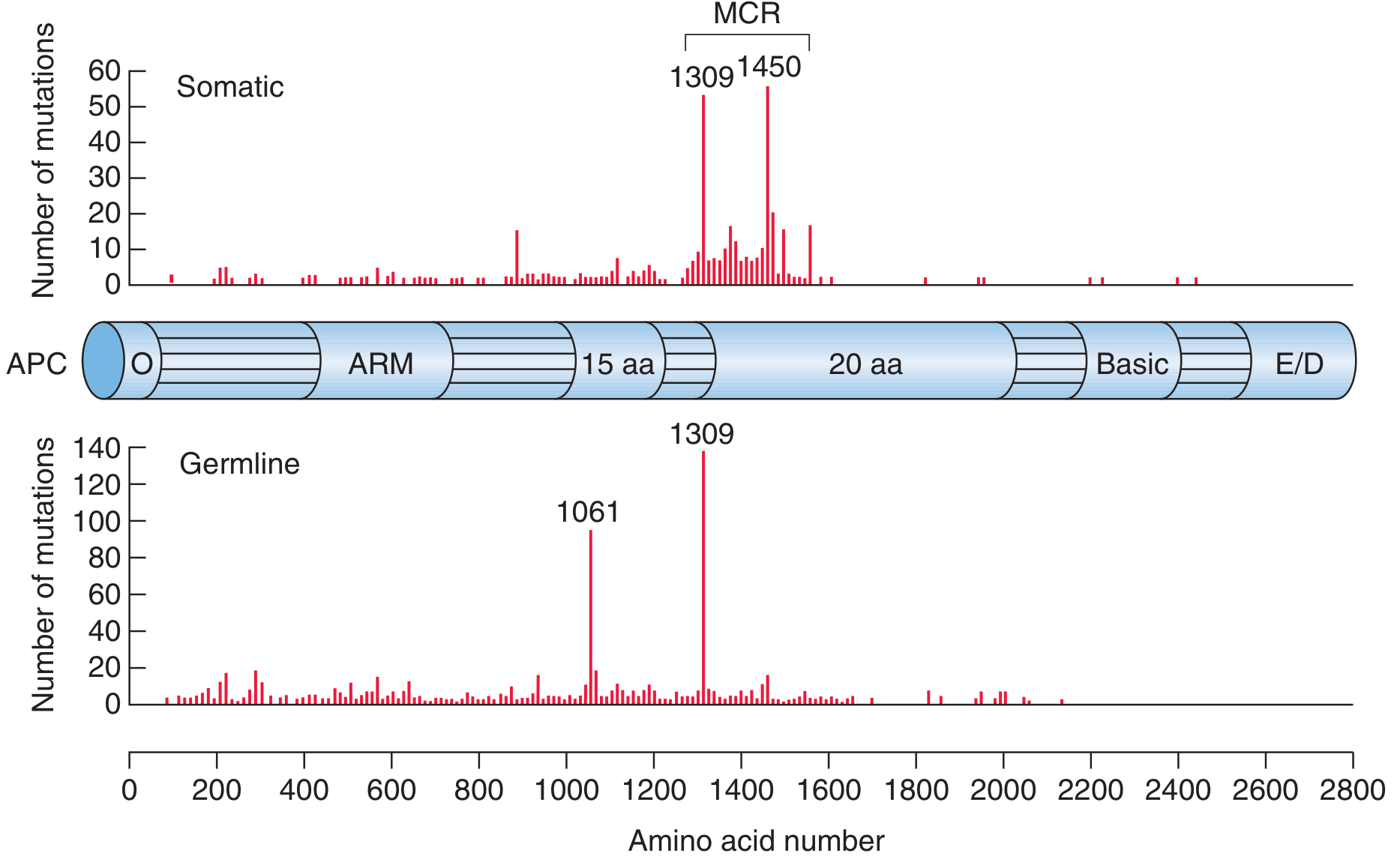
| FAP | APC | Colorectal (near 100% by age 40) |
| MEN1 | MEN1 | Parathyroid, pituitary, pancreas |
| MEN2 | RET gain-of-function | Medullary thyroid, pheo, parathyroid |
| Li-Fraumeni | TP53 | Sarcoma, breast, brain, leukemia, adrenal |
| VHL | VHL | Clear cell RCC, hemangioblastoma, pheo |
| PTEN/Cowden | PTEN | Breast, thyroid, endometrial |
| Gorlin syndrome | PTCH1 | Basal cell carcinomas (hundreds) |
Mnemonic for MEN syndromes:
- MEN 1 = 3P's: Parathyroid, Pituitary, Pancreas
- MEN 2A = 3M's: Medullary thyroid, pheochroMocytoma, Munching (hyperparathyroid)
- MEN 2B = 2M + Mucosal neuroma + Marfanoid
CHAPTER 77 — Principles of Cancer Treatment
Hallmarks of Cancer (Hanahan & Weinberg)
- Self-sufficiency in growth signals
- Insensitivity to anti-growth signals
- Evasion of apoptosis
- Limitless replicative potential (telomerase)
- Sustained angiogenesis (VEGF)
- Tissue invasion and metastasis
- Reprogrammed energy metabolism (Warburg effect)
- Evasion of immune destruction
- Tumor-promoting inflammation
- Genome instability
Cancer Treatments Overview
Surgery
- Best for localized disease
- Principles: adequate margins, lymph node sampling
- Sentinel node biopsy: inject radiotracer/dye → find first draining node
Radiation Therapy
- Ionizing radiation → DNA double-strand breaks
- Normal tissue tolerance limits dose
- Types: External beam (EBRT), Brachytherapy (implanted sources), Stereotactic (SBRT/SRS)
- Most sensitive: Rapidly dividing cells (marrow, GI mucosa, gonads)
Chemotherapy Cell Cycle Specificity
| Phase-specific | Non-phase-specific |
|---|---|
| Methotrexate (S phase) | Alkylating agents |
| 5-FU (S phase) | Platinum compounds |
| Vincristine/Vinblastine (M phase) | Anthracyclines |
| Taxanes (M phase) | |
| Etoposide (G2/M) |
Mnemonic for alkylating agents: "BCNU Can Make Cancer Worse"
- Busulfan, CCNU (lomustine), Nitrogen mustard, Cyclophosphamide, Melphalan, Chlorambucil, Carmustine
Targeted Therapies (Key Table)
| Drug | Target | Disease |
|---|---|---|
| Imatinib | BCR-ABL, c-Kit, PDGFR | CML, GIST |
| Erlotinib/Gefitinib | EGFR | NSCLC |
| Osimertinib | EGFR T790M | NSCLC (resistance mutation) |
| Trastuzumab | HER2 | Breast, gastric |
| Bevacizumab | VEGF-A | Colorectal, lung, ovarian, GBM |
| Rituximab | CD20 | B-cell lymphomas |
| Cetuximab | EGFR | Colorectal (RAS wild-type only!), H&N |
| Vemurafenib | BRAF V600E | Melanoma |
| Sorafenib | VEGFR, BRAF, PDGFR | RCC, HCC, thyroid |
| Sunitinib | VEGFR, c-Kit, PDGFR | RCC, GIST, PNET |
| ATRA | PML-RARα | APL (M3 AML) |
| Asciminib | BCR-ABL (allosteric) | CML (resistant/intolerant) |
Immune Checkpoint Inhibitors
| Target | Drugs | Key Tumors |
|---|---|---|
| PD-1 | Pembrolizumab, Nivolumab | NSCLC, melanoma, many others |
| PD-L1 | Atezolizumab, Durvalumab | Bladder, NSCLC, HCC |
| CTLA-4 | Ipilimumab | Melanoma (with nivolumab) |
Key immune-related adverse events (irAEs):
- Colitis (most common with CTLA-4)
- Pneumonitis (most common with PD-1)
- Hepatitis, hypophysitis, thyroiditis, nephritis, dermatitis
- Treatment: Corticosteroids; severe cases → infliximab (colitis), mycophenolate (hepatitis)
CAR-T Cell Therapy
- T cells engineered to express chimeric antigen receptors (CARs)
- FDA approved for B-cell ALL (tisagenlecleucel), DLBCL, myeloma, follicular lymphoma
- Key toxicities:
- Cytokine Release Syndrome (CRS): fever, hypotension, hypoxia → treat with tocilizumab (IL-6 receptor blocker)
- Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS): confusion, aphasia, seizures → corticosteroids
CHAPTER 78 — Principles of Cancer Treatment (Endocrine)
Covered in Ch 77; cancer immunotherapy-associated endocrinopathies:
- CTLA-4 inhibitors → hypophysitis most common
- PD-1 inhibitors → thyroid dysfunction most common
- Both → type 1 DM (rare but irreversible)
CHAPTER 79 — Infections in Patients with Cancer
Neutropenic Fever (NF)
Definition: Fever ≥38.3°C (or ≥38°C x 1h) + ANC <500/µL (or expected to fall <500)
First Episode Management
- Blood cultures → start antibiotics within 1 hour
- Monotherapy with anti-pseudomonal coverage:
- Cefepime, ceftazidime, piperacillin-tazobactam, meropenem, imipenem
- Add vancomycin only if: sepsis, soft tissue infection, catheter site infection, pneumonia, severe mucositis (with ceftazidime), MRSA carrier, penicillin-resistant pneumococcus carrier
- Do NOT routinely add vancomycin (increases nephrotoxicity, no mortality benefit)
When to Add Antifungals
- Add if fever persists 4-7 days on broad antibiotics + persistent neutropenia
- Empirical antifungals: Liposomal amphotericin B, caspofungin, voriconazole
- Prevention: Fluconazole prophylaxis in high-risk (AML induction, stem cell transplant)
MASCC Score (Low-Risk NF — Safe for Outpatient Tx)
Score ≥21 = low risk → can use oral ciprofloxacin + amoxicillin-clavulanate
| Factor | Points |
|---|---|
| Burden of symptoms: no/mild | 5 |
| No hypotension | 5 |
| No COPD | 4 |
| Solid tumor or no fungal infection | 4 |
| No dehydration | 3 |
| Outpatient status at onset | 3 |
| Age <60 | 2 |
Mnemonic: "MASCC = Mild, Afebrile outpatient, Solid tumor, Compensated pressure, Can walk"
CHAPTER 80 — Oncologic Emergencies
Three categories:
- Structural/Obstructive
- Metabolic/Hormonal (Paraneoplastic)
- Treatment-related
SUPERIOR VENA CAVA SYNDROME (SVCS)
Causes:
- Lung cancer (~85% of malignant causes) — especially small cell and squamous cell
- Lymphoma (young adults — most commonly NHL)
- Benign causes now ~40% (intravascular devices, pacemakers)
Clinical Features:
- Facial/arm swelling, dyspnea, headache (worse bending forward)
- Distended neck/chest veins, plethora, Pemberton's sign
Treatment:
- Endovascular stenting = fastest symptom relief
- Radiation for radiosensitive tumors (lymphoma, SCLC)
- Chemotherapy for SCLC, lymphoma (both radiation and chemo)
SPINAL CORD COMPRESSION
Most common tumors: Lung > Breast > Prostate > Lymphoma > Myeloma
Symptoms: Back pain (earliest!) → weakness → sensory loss → bowel/bladder dysfunction
Treatment: Dexamethasone 10mg IV immediately → MRI whole spine → XRT or surgery (decompression laminectomy preferred if single level, good prognosis, neurologically intact or rapidly progressive)
⚠️ Back pain in cancer patient = MRI spine until proven otherwise
INCREASED INTRACRANIAL PRESSURE (Brain Mets)
- Most common: Lung, breast, melanoma, colon, RCC
- Treatment: Dexamethasone + whole brain XRT ± resection ± stereotactic radiosurgery
PERICARDIAL EFFUSION/TAMPONADE
- Breast, lung, lymphoma, leukemia
- Treatment: Pericardiocentesis (diagnostic + therapeutic)
METABOLIC ONCOLOGIC EMERGENCIES
Hypercalcemia of Malignancy
Most common metabolic emergency in cancer!
Mechanisms:
- PTHrP secretion (most common) — squamous (lung, H&N, esophagus), renal, breast
- Osteolytic mets — breast, myeloma
- 1,25-OH vitamin D excess — lymphoma (granulomatous activation of 1-alpha-hydroxylase)
- True ectopic PTH — rare
Symptoms (BONES, GROANS, MOANS, PSYCHIC OVERTONES):
- Bones: pain
- Groans: nausea, vomiting, constipation
- Moans: fatigue, weakness
- Psychic: confusion, coma
Treatment:
- IV fluids (0.9% NS)
- Bisphosphonates — pamidronate or zoledronate (onset 2-4 days, lasts weeks)
- Denosumab — anti-RANKL (for bisphosphonate-refractory or renal failure)
- Calcitonin — fastest onset (hours) but tachyphylaxis in 48h
- Corticosteroids — for lymphoma and vitamin D-mediated
Tumor Lysis Syndrome (TLS)
Most common in: Burkitt lymphoma, ALL, AML (especially high WBC)
Lab findings (Cairo-Bishop criteria):
- Hyperuricemia
- Hyperkalemia
- Hyperphosphatemia
- Hypocalcemia
- Elevated creatinine (AKI)
Prevention: Allopurinol (blocks uric acid synthesis) or Rasburicase (enzymatic degradation — preferred in high risk; contraindicated in G6PD deficiency)
Treatment: Aggressive IV hydration, rasburicase, dialysis if needed
Mnemonic: "TLS = Tumor Lysis Syndrome → Potassium Up, Phosphate Up, Uric Acid Up, Calcium Down"
SIADH in Cancer
- Most common cause in cancer: Small Cell Lung Cancer
- Also: brain mets, vincristine, cyclophosphamide
- Treatment: fluid restriction; demeclocycline; conivaptan/tolvaptan
Lactic Acidosis
- Leukemia, lymphoma, solid tumors with massive liver involvement
- Treatment: Treat underlying cancer; bicarbonate for severe acidosis; hemodialysis
Hypoglycemia
- Non-islet cell tumors: retroperitoneal sarcomas, hepatomas, adrenocortical tumors
- Mechanism: IGF-II secretion (big IGF-II — incompletely processed)
- Distinguish from insulinoma: suppressed C-peptide and insulin, elevated IGF-II/IGF-I ratio
CHAPTER 81 — Lung Cancer
Epidemiology
- #1 cancer killer in both sexes worldwide
- ~85% are non-small cell lung cancer (NSCLC); ~15% small cell (SCLC)
NSCLC Types
| Type | Location | Key Mutation | Association |
|---|---|---|---|
| Adenocarcinoma | Peripheral | EGFR (Asian women), KRAS, ALK, ROS1 | Never/light smokers |
| Squamous | Central | SOX2, FGFR1 | Heavy smokers |
| Large cell | Peripheral | — | Smokers |
SCLC
- Central, aggressive, neuroendocrine
- Paraneoplastic syndromes: SIADH, Cushing's (ectopic ACTH), Lambert-Eaton
- Very chemo/radiation-sensitive but almost always recurs
- Limited stage: cisplatin + etoposide + thoracic XRT ± prophylactic cranial irradiation (PCI)
- Extensive stage: cisplatin/carboplatin + etoposide ± atezolizumab
NSCLC Treatment by Stage
- Stage I-II: Surgery (lobectomy preferred)
- Stage III: Concurrent chemoradiation + durvalumab maintenance
- Stage IV: Biomarker-driven:
- EGFR mutation → Osimertinib
- ALK/ROS1 rearrangement → Alectinib (ALK), Entrectinib (ROS1)
- BRAF V600E → Dabrafenib + Trametinib
- MET exon 14 skipping → Capmatinib
- KRAS G12C → Sotorasib/Adagrasib
- PD-L1 ≥50% → Pembrolizumab monotherapy
- PD-L1 any → Chemo + pembrolizumab
CHAPTER 82 — Head and Neck Cancers
- Squamous cell carcinoma in >90% of cases
- Risk: tobacco + alcohol (synergistic), HPV (oropharyngeal — especially HPV-16)
- HPV-positive oropharyngeal cancer: better prognosis, younger, non-smokers
- Treatment: Surgery and/or radiation ± cisplatin; cetuximab if cisplatin-ineligible
- Recurrent/metastatic: pembrolizumab ± chemo (KEYNOTE-048)
CHAPTER 83 — Esophageal Cancer
| Feature | Squamous Cell (SCC) | Adenocarcinoma |
|---|---|---|
| Location | Upper/mid | Lower/GEJ |
| Risk factors | Tobacco, alcohol, achalasia | GERD, Barrett's, obesity |
| Trend | Declining | Increasing |
- Localized: Surgery + neoadjuvant chemoradiation (CROSS trial: carboplatin-paclitaxel + XRT)
- Metastatic: Nivolumab + chemo (first line, PD-L1 CPS ≥5)
CHAPTER 84 — Gastric Cancer
- Helicobacter pylori is the #1 risk factor for intestinal type
- Lauren classification: Intestinal (better prognosis) vs. Diffuse (signet ring, worse prognosis)
- Diffuse = CDH1 mutation in hereditary cases
- HER2 overexpression in ~20% → trastuzumab + chemo (first line, metastatic)
- Nivolumab + FOLFOX now standard for HER2-negative advanced disease
CHAPTER 85 — Pancreatic Cancer
- 5th leading cause of cancer death; only ~10% resectable at diagnosis
- Risk: smoking, DM, chronic pancreatitis, familial (BRCA2, PALB2, ATM)
- Whipple procedure (pancreaticoduodenectomy) for resectable head tumors
- Adjuvant: mFOLFIRINOX (fit patients) or gemcitabine + capecitabine
- Metastatic: FOLFIRINOX (fit) or gemcitabine + nab-paclitaxel
- BRCA1/2 mutant: maintenance olaparib (POLO trial)
CHAPTER 86 — Colorectal Cancer (CRC)
Risk Factors
Mnemonic: "DISH + Fat"
- Diet (animal fat, red/processed meat)
- Inflammatory bowel disease
- Streptococcus bovis bacteremia
- Hereditary syndromes
- Fat (Obesity), tobacco
Hereditary CRC Syndromes
| Syndrome | Gene | Key Features |
|---|---|---|
| FAP | APC (AD) | Thousands of polyps, 100% cancer by 40s, duodenal ampullary cancer |
| Gardner's | APC | FAP + osteomas + desmoid + epidermoid cysts + retinal pigment hypertrophy |
| Turcot's | APC or mismatch repair | FAP + brain tumors |
| Lynch (HNPCC) | MLH1/MSH2/MSH6/PMS2 | ~80% lifetime CRC risk, proximal colon predominant, endometrial/ovarian cancer |
| Peutz-Jeghers | STK11/LKB1 | Hamartomas + mucocutaneous pigmentation + GI/ovarian/breast/pancreas |
| MUTYH-polyposis | MUTYH (AR) | Adenomas, CRC |
Molecular Pathways in CRC
- Chromosomal instability (CIN) — APC → K-RAS → SMAD4 → TP53 (85%)
- Microsatellite instability (MSI/MMR-deficient) — Lynch syndrome and sporadic (15%)
- CIMP/serrated pathway — BRAF V600E + MLH1 methylation (serrated polyps)
Staging and Treatment
| Stage | 5-yr Survival | Treatment |
|---|---|---|
| I | 90% | Surgery alone |
| II | 70-80% | Surgery ± adjuvant (high-risk features) |
| III | 40-65% | Surgery + FOLFOX or CAPOX x 6 months |
| IV | ~15-25% | Systemic therapy; resect if resectable |
Metastatic CRC Key Drugs: 5-FU/capecitabine, oxaliplatin, irinotecan, bevacizumab
- MSI-High (dMMR): Pembrolizumab first-line (long-term responses possible!)
- RAS wild-type, left-sided: Add cetuximab or panitumumab to chemo
- BRAF V600E: Encorafenib + cetuximab in 2nd line
⚠️ Always check RAS (KRAS/NRAS) and BRAF status before starting biologics!
CHAPTER 87 — Hepatocellular Carcinoma (HCC)
Epidemiology
- Most common primary liver cancer globally (5th most common overall)
- Risk factors: Cirrhosis (any cause), HBV, HCV, aflatoxin B1, alcohol, NASH/NAFLD, hemochromatosis
Mnemonic for HCC risk factors: "CIA + HABN"
- Cirrhosis, Infection (HBV/HCV), Aflatoxin
- Hemochromatosis, Alcohol, NAFLD, Birth weight/genetics
Screening
- All cirrhotic patients: ultrasound + AFP every 6 months
- AFP >200 in right context is diagnostic; AFP >400 essentially diagnostic
Diagnosis (Barcelona Criteria)
- Can diagnose without biopsy in cirrhotic patients:
- Lesion >1 cm with arterial enhancement + portal venous washout on CT/MRI
Staging (Barcelona BCLC)
| Stage | Characteristics | Treatment |
|---|---|---|
| 0/A (Very early/Early) | Single ≤2cm or ≤3 nodules ≤3cm, good PS, no portal HTN | Resection, ablation, transplant |
| B (Intermediate) | Multinodular, compensated | TACE |
| C (Advanced) | Vascular invasion or extrahepatic spread | Sorafenib → Lenvatinib; Atezolizumab + bevacizumab (preferred first-line) |
| D (Terminal) | Poor PS, decompensated | Best supportive care |
Transplant criteria (Milan): Single ≤5 cm or ≤3 nodules ≤3 cm, no vascular invasion, no extrahepatic spread
Current First-Line Systemic Therapy
Atezolizumab + bevacizumab (IMbrave150) — improved OS vs sorafenib
Second line: Regorafenib, cabozantinib, ramucirumab (AFP >400)
CHAPTER 88 — Cholangiocarcinoma (CCA) and Biliary Cancers
- Types: Intrahepatic (iCCA), Perihilar (Klatskin tumor), Distal
- Risk: PSC (especially perihilar), liver flukes (Clonorchis/Opisthorchis), IBD, bile duct cysts
Treatment
- Resectable: Surgery → adjuvant capecitabine x 6 months (BILCAP trial)
- Unresectable: Gemcitabine + cisplatin + durvalumab (TOPAZ-1) — now standard of care
- 2nd line: mFOLFOX; IDH1 inhibitor (ivosidenib) for IDH1-mutant; FGFR inhibitors (pemigatinib, infigratinib) for FGFR2-fused iCCA
CHAPTER 89 — Gastrointestinal Neuroendocrine Tumors (NETs)
Classification
- Graded by Ki-67 proliferation index:
- G1: Ki-67 <3%, well-differentiated
- G2: Ki-67 3-20%, well-differentiated
- G3: Ki-67 >20% (includes both well-diff NETs and poorly-diff NECs)
Carcinoid Syndrome
- Requires liver mets (bypasses hepatic first-pass metabolism) or non-hepatic source
- Symptoms: flushing + diarrhea + bronchospasm + right heart disease (tricuspid/pulmonic)
- Marker: 24-hour urinary 5-HIAA, serum chromogranin A
- Treatment: Octreotide (somatostatin analog) — symptom control and antiproliferative
- Carcinoid crisis (during surgery) → IV octreotide infusion
Mnemonic for Carcinoid: "FDBR" = Flushing, Diarrhea, Bronchospasm, Right heart disease
Pancreatic NETs (Functioning)
| Tumor | Hormone | Syndrome |
|---|---|---|
| Insulinoma | Insulin | Whipple's triad (symptoms, low glucose, relief with glucose) |
| Gastrinoma | Gastrin | Zollinger-Ellison (peptic ulcers, diarrhea) |
| VIPoma | VIP | WDHA (watery diarrhea, hypokalemia, achlorhydria) |
| Glucagonoma | Glucagon | Necrolytic migratory erythema, DM, weight loss |
| Somatostatinoma | Somatostatin | Diabetes, cholelithiasis, steatorrhea |
Mnemonic: "I Get Very Good Somatostatin" = Insulinoma, Gastrinoma, VIPoma, Glucagonoma, Somatostatinoma
Treatment
- Resectable: Surgery
- Unresectable G1/G2: Octreotide/Lanreotide (PROMID, CLARINET trials) → Everolimus (mTOR) → Sunitinib (VEGFR) → PRRT (177Lu-DOTATATE for somatostatin receptor-positive)
CHAPTER 90 — Thyroid Cancer
| Type | Frequency | Genetics | 10-yr Survival |
|---|---|---|---|
| Papillary | 80-85% | BRAF V600E, RET/PTC rearrangement | >95% |
| Follicular | 10-15% | RAS, PAX8-PPARγ | 85-90% |
| Medullary | 3-5% | RET mutation (25% familial → MEN2) | 75% |
| Anaplastic | 1-2% | TP53, BRAF, TERT | <10% (months) |
- Medullary thyroid: Calcitonin is tumor marker; RET proto-oncogene testing for ALL patients (and family screening)
- Anaplastic: BRAF V600E targeted therapy (dabrafenib + trametinib) for ~50%
CHAPTER 91 — Bladder and Urinary Tract Cancer
Epidemiology
- 4th most common cancer in men
- Transitional cell carcinoma (urothelial) in >90%
- Risk factors: Smoking (#1), aniline dyes, cyclophosphamide, schistosomiasis (squamous cell in endemic areas), pelvic radiation
Classification
- NMIBC (non-muscle invasive, Ta/T1/CIS): ~75% at presentation
- MIBC (T2+): Requires cystectomy
Treatment
- NMIBC: TURBT → intravesical BCG (intermediate/high-risk) → repeat TURBT
- BCG failure → cystectomy (preferred) or pembrolizumab/nadofaragene
- MIBC: Neoadjuvant cisplatin + chemo → radical cystectomy OR bladder-sparing (chemoradiation)
- Metastatic: Cisplatin + gemcitabine → maintenance avelumab (after platinum response) OR pembrolizumab (cisplatin-ineligible)
CHAPTER 92 — Prostate Cancer
Key Facts
- Most common cancer in men
- PSA — screening controversial, shared decision-making
- Gleason score → Grade Groups 1-5 (GG1 = most favorable)
Staging and Treatment Overview
| Stage | Treatment Options |
|---|---|
| Localized (low-risk GG1) | Active surveillance |
| Localized (intermediate/high-risk) | Radical prostatectomy or definitive XRT ± ADT |
| Locally advanced (T3/N1) | XRT + long-term ADT |
| Metastatic hormone-sensitive | ADT + docetaxel or ADT + abiraterone/enzalutamide/apalutamide |
| Castration-resistant (mCRPC) | Abiraterone, enzalutamide, docetaxel, cabazitaxel, radium-223 (bone mets), PARP inhibitors (BRCA1/2) |
Mnemonic for hormonal agents: "Abi-En-Apa" block androgen axis at 3 levels:
- Abiraterone → CYP17 (blocks testosterone synthesis, adrenal + gonadal)
- Enzalutamide → AR (blocks receptor)
- Leuprolide/Degarelix → GnRH (castrate testosterone)
CHAPTER 93 — Testicular Cancer
- Most common solid tumor in men age 15-35
- Highly curable, even with metastasis (paradigm of curable solid tumor cancer)
- Arise from primordial germ cells
Classification
| Type | Markers | Features |
|---|---|---|
| Seminoma | hCG (rarely), ALP | Pure, radiosensitive, NEVER makes AFP |
| Nonseminoma (NSGCT) | AFP, hCG, LDH | Includes embryonal, choriocarcinoma, yolk sac, teratoma |
⚠️ Elevated AFP = NSGCT by definition, even if pathology shows pure seminoma
Staging & Treatment
| Stage | Treatment |
|---|---|
| I Seminoma | Orchiectomy ± surveillance (preferred)/para-aortic XRT/carboplatin x1 |
| I NSGCT | Orchiectomy + RPLND or surveillance (low-risk) |
| IIA/B Seminoma | XRT |
| IIA/B NSGCT | BEP x3 cycles |
| III (any) | BEP x3-4 cycles |
BEP = Bleomycin + Etoposide + Cisplatin
Mnemonic: "SEMinoma = Sensitive Every time (radiotherapy works), NSGCT = Need Surgery/Chemo"
CHAPTER 94 — Gynecologic Malignancies
Ovarian Cancer
- #1 cause of gynecologic cancer death (because diagnosed late)
- Serous high-grade = most common and aggressive (TP53, BRCA1/2 somatic)
- Hereditary: BRCA1 (40% lifetime risk), BRCA2 (15-25% risk), Lynch syndrome (endometrial > ovarian)
- Tumor marker: CA-125 (monitoring, not screening)
- Treatment: Surgical cytoreduction ("debulking") + carboplatin + paclitaxel ± bevacizumab
- Maintenance: PARP inhibitors (olaparib, niraparib, rucaparib) — especially in BRCA1/2 mutant or HRD positive → dramatic PFS improvement
Mnemonic: "PARP inhibitors = Platinum-Responsive homologous-recombination Affected tumors respond Permanently"
Endometrial Cancer
- Most common gynecologic cancer in the USA
- Risk: unopposed estrogen (obesity, PCOS, nulliparity, estrogen therapy without progesterone, Lynch syndrome)
- Type I: Endometrioid (low-grade, estrogen-driven, good prognosis)
- Type II: Serous/Clear cell (high-grade, non-estrogen, worse prognosis)
- Molecular classification (TCGA): POLE ultramutated (best) > MMR-deficient > copy-number low > copy-number high/serous-like (worst)
- Metastatic: Pembrolizumab + lenvatinib (regardless of MSI status) — [KEYNOTE-775/Study 309]
Cervical Cancer
- HPV types 16 and 18 → 70% of cervical cancers
- Screening: Pap + HPV co-test every 5 years (age 25-65)
- Treatment: IA1 → conization; IA2-IIA → surgery; IIB+ → chemoradiation (cisplatin + XRT)
- Metastatic: Pembrolizumab + bevacizumab + chemo → improved OS
CHAPTER 95 — Breast Cancer
Risk Factors
ABCDEFG: Age, BRCA/genes, Contraceptives, Density, Estrogen exposure, Family history, Glandular tissue prior bx
Subtypes by Receptor Status
| Subtype | ER | PR | HER2 | Treatment |
|---|---|---|---|---|
| Luminal A | + | + | - | Endocrine therapy ± CDK4/6 inhibitors |
| Luminal B | + | +/- | - | Endocrine + chemo |
| HER2-enriched | - | - | + | Anti-HER2 (trastuzumab, pertuzumab, T-DM1) |
| Triple negative (TNBC) | - | - | - | Chemo ± immunotherapy; PARP if BRCA |
Key Drugs
- Tamoxifen (ER+, premenopausal); Aromatase inhibitors (letrozole, anastrozole — postmenopausal)
- CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) + AI → standard 1st-line metastatic ER+ HER2-
- Trastuzumab + pertuzumab + docetaxel → metastatic HER2+
- Olaparib/talazoparib → BRCA1/2 mutant HER2-negative advanced
CHAPTER 96 — Soft Tissue and Bone Sarcomas
Soft Tissue Sarcomas
- Liposarcoma (most common overall), leiomyosarcoma, synovial sarcoma, rhabdomyosarcoma (children)
- Grading is the most important prognostic factor (FNCLCC system: G1/G2/G3)
- Treatment: Wide surgical excision ± radiation; Doxorubicin ± ifosfamide (metastatic)
- Special targetable sarcomas:
- GIST: Imatinib → sunitinib → regorafenib
- Synovial sarcoma: EZH2 inhibitor (tazemetostat)
- Alveolar soft part sarcoma: Atezolizumab
Bone Sarcomas
| Tumor | Age | Location | Features |
|---|---|---|---|
| Osteosarcoma | Teens | Distal femur/proximal tibia/proximal humerus | Sunburst pattern, Codman triangle (XR) |
| Ewing's sarcoma | Teens | Diaphysis long bones, flat bones | "Onion skin" periosteal reaction, t(11;22) EWS-FLI1 |
| Chondrosarcoma | Adults 40-70 | Pelvis, long bones, ribs | Central calcifications, chemotherapy-resistant |
Osteosarcoma treatment: Limb-sparing surgery + neoadjuvant MAP (methotrexate, adriamycin, cisplatin)
Ewing's treatment: Chemotherapy (VDC-IE) + local control (surgery or radiation)
⚠️ Chondrosarcoma = chemotherapy resistant → surgery is mainstay
CHAPTER 97 — Carcinoma of Unknown Primary (CUP)
Definition
Metastatic cancer found without identifiable primary site despite workup
Initial Workup
- CT chest/abdomen/pelvis
- PET-CT (increases primary detection ~20-30%)
- Immunohistochemistry panel (cytokeratins, TTF-1, CDX2, PSA, ER/PR, etc.)
- Next-generation sequencing (NGS)/Molecular profiling — 85% have ≥1 actionable mutation
Favorable Subsets (Treatable Like Known Primary)
| Subset | Presumed Site | Treatment |
|---|---|---|
| Women with axillary nodes | Breast | Treat as breast cancer |
| Women with peritoneal carcinomatosis | Ovary | Treat as ovarian cancer |
| Squamous cell in cervical nodes | H&N | XRT ± surgery |
| Squamous cell in inguinal nodes | Anal/vulva/cervix | XRT + chemo |
| Young men midline mass, AFP/hCG elevated | Germ cell | BEP chemotherapy |
| PSA positive, blastic bone mets | Prostate | ADT |
| Single metastasis | — | Aggressive local therapy |
General CUP Prognosis
- Median survival: 6-10 months
- Chemotherapy: Carboplatin + paclitaxel (most common empiric)
- Tumor-agnostic therapies: Pembrolizumab (MSI-H/TMB-H), NTRK inhibitors (NTRK fusion)
CHAPTER 98 — Paraneoplastic Syndromes
Endocrine Paraneoplastic Syndromes
| Syndrome | Mechanism | Tumor |
|---|---|---|
| SIADH | Ectopic ADH | SCLC (most common) |
| Cushing's | Ectopic ACTH | SCLC, carcinoid, thymoma |
| Hypercalcemia | PTHrP | Squamous (lung, H&N), renal, breast |
| Hypoglycemia | IGF-II | Sarcoma, hepatoma |
| Carcinoid syndrome | 5-HT, substance P | Carcinoid (with liver mets) |
| Acromegaly | Ectopic GHRH | Carcinoid, PNET |
| Erythrocytosis | Ectopic EPO | RCC, HCC, cerebellar hemangioblastoma |
| Granulocytosis | G-CSF, GM-CSF, IL-6 | Lung, GI, ovarian |
Neurologic Paraneoplastic Syndromes
| Syndrome | Antibody | Tumor |
|---|---|---|
| Paraneoplastic cerebellar degeneration | Anti-Yo (PCA-1) | Breast, ovary |
| Lambert-Eaton | Anti-VGCC | SCLC |
| Encephalomyelitis/sensory neuropathy | Anti-Hu (ANNA-1) | SCLC |
| Limbic encephalitis | Anti-LGI1, Anti-NMDAR | Thymoma, ovarian teratoma |
| Opsoclonus-myoclonus | Anti-Ri | Breast, SCLC |
| Stiff-person syndrome | Anti-amphiphysin | Breast, SCLC |
| Dermatomyositis | — | Lung, GI, ovary |
Mnemonic for anti-Hu: "Hu = SCLC Sensory neuropathy, Encephalomyelitis" (Hu = Horrible Underlying = SCLC)
VGCC = Voltage-Gated Calcium Channel antibody → Lambert-Eaton myasthenic syndrome
- Proximal weakness improving with repetition (contrast with myasthenia which worsens)
- Diminished reflexes, autonomic dysfunction
- Treatment: 3,4-diaminopyridine (DAP) → pyridostigmine; treat tumor (SCLC)
Caspr2 antibodies → Morvan syndrome (encephalitis + peripheral nerve hyperexcitability + autonomic + insomnia) — associated with thymoma
LGI1 antibodies → faciobrachial dystonic seizures + hyponatremia + limbic encephalitis
CHAPTER 99 — Paraneoplastic Neurologic Syndromes (see Ch 98)
Summary of Key Antibodies
| Antibody | Syndrome | Cancer |
|---|---|---|
| Anti-Hu | Sensory neuropathy, encephalomyelitis | SCLC |
| Anti-Yo (PCA-1) | Cerebellar degeneration | Ovary, breast |
| Anti-Ri (ANNA-2) | Opsoclonus-myoclonus | Breast, SCLC |
| Anti-VGCC | Lambert-Eaton | SCLC |
| Anti-NMDAR | Limbic encephalitis | Ovarian teratoma |
| Anti-LGI1 | Faciobrachial seizures, limbic enceph | Thymoma (rare) |
| Anti-Caspr2 | Morvan syndrome, peripheral nerve hyperex | Thymoma |
| Anti-GABA-B | Limbic encephalitis, seizures | SCLC |
| Anti-amphiphysin | Stiff-person | Breast, SCLC |
CHAPTER 100 — Cancer Survivorship and Late Effects
Growing Problem
-
18 million cancer survivors in USA (and growing)
- Late effects can occur years to decades after treatment
Key Late Effects by Treatment
Chemotherapy:
- Anthracyclines (doxorubicin) → Cardiomyopathy (dose-dependent; >550 mg/m² high risk)
- Bleomycin → Pulmonary fibrosis (dose + oxygen exposure)
- Cisplatin → Nephrotoxicity, ototoxicity, peripheral neuropathy
- Alkylating agents → Secondary leukemia (AML), infertility, bladder cancer (cyclophosphamide)
- Cyclophosphamide >9 g/m² → Long-term azoospermia
Radiation:
- Head/neck XRT → Hypothyroidism, dental caries, xerostomia, cataracts, secondary cancers
- Thoracic XRT → Cardiomyopathy, pericarditis, lung fibrosis
- Pelvic XRT → Infertility, premature menopause, secondary malignancy (~1% at 10 yrs)
- Cranial XRT → Cognitive decline, growth hormone deficiency, obesity (leptin biology)
Immunotherapy (ICIs):
- CTLA-4 inhibitors → Hypophysitis > colitis > hepatitis
- PD-1 inhibitors → Thyroiditis > pneumonitis > hepatitis
- Autoimmune toxicities require lifelong hormone replacement if glands destroyed
Second Malignancies
- Most feared late effect
- Alkylating agents + topoisomerase inhibitors → therapy-related AML (t-AML)
- Alkylating → t-AML latency 5-7 years, complex karyotype
- Topoisomerase II → t-AML latency 2-3 years, 11q23 (MLL rearrangement), balanced translocations
- Radiation → solid tumors (breast after Hodgkin's, sarcomas)
Fertility Preservation
- All patients: Counsel before treatment
- Males: Sperm cryopreservation
- Females: Oocyte or embryo cryopreservation (preferred); ovarian tissue banking (experimental)
- GnRH agonists concurrent with chemo → may preserve ovarian function (evidence modest)
Key counseling point: Spermatogenesis is more radiosensitive than Leydig cell function; fertility is lost at lower doses than endocrine function
MASTER MNEMONICS SUMMARY
| Mnemonic | Topic |
|---|---|
| "LPCP" | Top cancer deaths in males: Lung, Prostate, Colon, Pancreas |
| "LLOS" | Screening biases: Lead-time, Length, Overdiagnosis, Selection |
| "3P's" for MEN1 | Parathyroid, Pituitary, Pancreas |
| "BONES GROANS MOANS PSYCHIC" | Hypercalcemia symptoms |
| "TLS PPUC" | Tumor lysis: K+↑, Phos↑, Urate↑, Ca↓ |
| "FDBR" | Carcinoid: Flushing, Diarrhea, Bronchospasm, Right heart |
| "I Get Very Good Somatostatin" | Pancreatic NET types |
| "DISH + Fat" | CRC risk factors |
| "MASCC" | Neutropenic fever low-risk criteria |
| "CIA + HABN" | HCC risk factors |
| "BEP" | Testicular cancer chemo: Bleomycin, Etoposide, Cisplatin |
| "Hu = SCLC" | Anti-Hu antibody → SCLC paraneoplastic |
| "On stuck = Oncogene" | Oncogenes are gain-of-function, dominant |
| "Two hits = tumor suppressor" | Knudson 2-hit hypothesis |
HIGH-YIELD EXAM FACTS AT A GLANCE
- #1 cancer killer in both sexes = Lung cancer
- Most common cancer in men = Prostate; in women = Breast
- Hypercalcemia mechanism in malignancy = PTHrP (most common)
- SVCS most common malignant cause = Lung cancer (SCLC/SqCC)
- Fastest acting agent for hypercalcemia = Calcitonin (hours); most durable = bisphosphonate
- Tumor Lysis Syndrome highest risk = Burkitt lymphoma, ALL
- AFP elevated = NSGCT (even if pathology says seminoma)
- Carcinoid syndrome requires liver mets (or non-hepatic primary)
- CRC + MSI-High = First-line pembrolizumab (not chemotherapy)
- PARP inhibitors benefit BRCA-mutated: ovarian, breast, prostate, pancreatic cancers
- BCR-ABL in CML → Imatinib/TKIs; ATRA for APL
- Lambert-Eaton = VGCC antibody, SCLC, weakness improves with repetition
- Anti-Yo = cerebellar degeneration, ovary/breast
- Osimertinib = EGFR T790M resistance mutation in NSCLC
- Milan criteria for liver transplant in HCC: single ≤5 cm or ≤3 nodules ≤3 cm
All content sourced from Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapters 73-100.
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill Medical)
This is a shared conversation. Sign in to Orris to start your own chat.