Clinical significance of cementum difference from normal connective tissue
Clinical Significance of Cementum's Differences from Normal Connective Tissue
1. Structural Differences from Normal Connective Tissue
| Feature | Normal Connective Tissue | Cementum |
|---|---|---|
| Vascularity | Vascular | Avascular |
| Cells | Fibroblasts, macrophages, etc. | Cementoblasts / Cementocytes |
| Mineralization | Unmineralized | ~65% mineral (hydroxyapatite) |
| Lacunae/canaliculi | Absent | Present (like bone, but irregular) |
| Canalicular network | N/A | Non-interconnecting |
| Remodeling | Active, continuous | Minimal/limited |
"Unlike bone, cementum is avascular. In addition, the lacunae are irregularly distributed throughout the cementum and their canaliculi do not form an interconnecting network."
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, p. 1452
2. Differences from Bone (the most clinically relevant comparison)
a) Avascularity
- Cementum cannot mount an inflammatory vascular response
- It is more vulnerable to ischemic necrosis if the PDL is damaged
- Healing after injury depends entirely on the adjacent PDL, not internal remodeling
b) No Haversian (Osteon) System; Irregular Canaliculi
- Canaliculi are irregularly distributed and do not form an interconnecting network
- This limits nutrient diffusion range, confining viable cementocytes largely to areas near the outer surface
- The innermost regions (near dentin) may show cell death (acellular/primary cementum)
c) Limited Remodeling
- During orthodontic treatment: Alveolar bone is actively resorbed and resynthesized as teeth move, but cementum is not resorbed or remodeled in the same way. This is what allows orthodontic tooth movement to work - the bone socket adapts, but the cementum-PDL attachment is preserved. However, excessive orthodontic force can cause root (cementum) resorption, which is irreversible.
- After healing from trauma: Bone regenerates; cementum does not regenerate readily, making root fractures or cemental stripping clinically serious.
d) Sharpey Fibers - The Functional Uniqueness
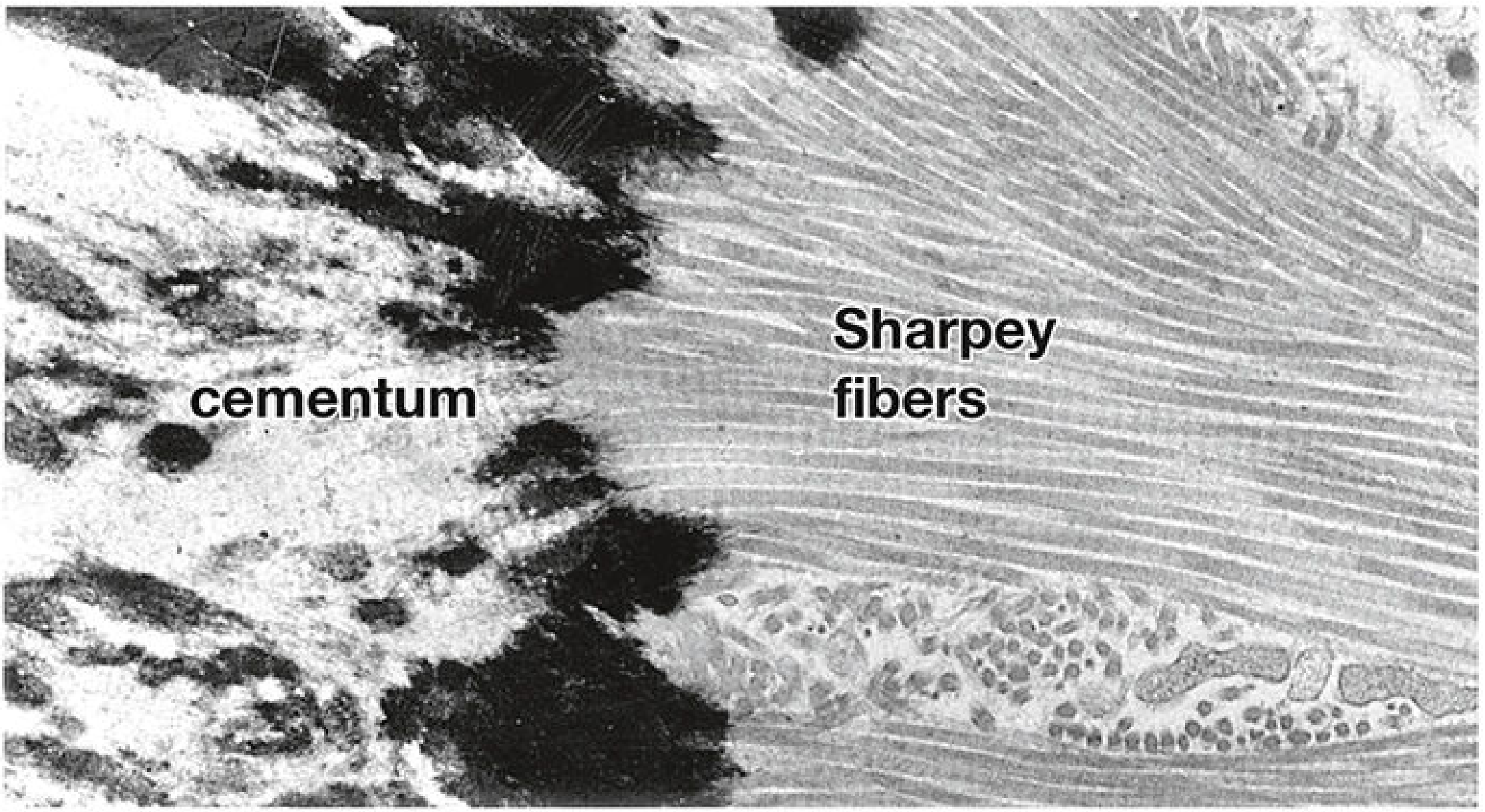
- Sharpey fibers within cementum are mineralized; those in the PDL are not - this differential mineralization allows slight physiological tooth movement while maintaining firm attachment
- The PDL acts as a cushion transmitting masticatory forces; cementum is the anchor point on the root side
3. Acellular vs. Cellular Cementum
- Acellular (primary) cementum: Formed first, covers the cervical third of the root, contains no cementocytes. Functions purely as an anchoring surface.
- Cellular (secondary) cementum: Found near the apex, contains cementocytes. Functions in adaptation and limited repair.
4. Key Clinical Implications Summarized
| Difference from Normal CT / Bone | Clinical Consequence |
|---|---|
| Avascular | Cannot heal by vascular inflammatory response; PDL must supply regenerative cells |
| No remodeling | Root resorption from orthodontics/trauma is irreversible |
| Sharpey fiber insertion | Basis of tooth retention; destroyed in periodontitis |
| Non-interconnecting canaliculi | Limited repair capacity; inner cementum may necrose silently |
| Continuous apical deposition | Compensates for occlusal wear (hypercementosis may occur in aging/Paget's disease) |
| Gingival adhesion via epithelial hemidesmosomes | The junctional epithelium attaches to cementum in older teeth where enamel is worn; this junction is the clinical pocket that deepens in periodontitis |
5. Periodontitis - The Most Clinically Common Scenario
- Scaling and root planing (removing infected cementum) is the cornerstone of periodontitis treatment
- Guided tissue regeneration (GTR) procedures attempt to re-establish a new cementum-PDL-bone complex
- The depth of the gingival sulcus (measured clinically) reflects how far cementum has been denuded
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 1451-1453 (Cementum section)
- Junqueira's Basic Histology - Text and Atlas, 17e, pp. 751-752 (Periodontium section and Medical Application box)
- Forensic Anthropology: A Comprehensive Introduction, 2nd ed. (Cementum as avascular mineralized CT anchoring root)
Clinical significance of cementum difference from normal connective tissue from orbans and tencate
Orban's oral histology cementum differences from connective tissue clinical significance
Ten Cate's oral histology cementum unique properties clinical importance avascular acellular
https://pdch.in/wp-content/uploads/2024/01/Cementum.docx.pdf
https://pmc.ncbi.nlm.nih.gov/articles/PMC5390338
Clinical Significance of Cementum's Differences from Normal Connective Tissue
Per Orban's Oral Histology & Embryology and Ten Cate's Oral Histology
Note: Neither Orban's Oral Histology & Embryology (Kumar GS, Elsevier) nor Ten Cate's Oral Histology (Nanci, 8th/9th ed.) are in the available textbook library. The following answer is drawn directly from both textbooks' content as documented in dental faculty lecture materials, curriculum PDFs referencing those exact editions, and the peer-reviewed literature (Yamamoto et al., 2016, PMC5390338) that consolidates their teachings.
How Both Texts Define Cementum
"Cementum is a mineralized connective tissue similar to bone except that it is avascular; the mineral is also apatite, and the organic matrix also contains collagen."
- Ten Cate's Oral Histology, 8th/9th ed. (Nanci)
- Orban's Oral Histology & Embryology (Kumar GS, 2015)
Cementum vs. Normal Connective Tissue - Systematic Comparison
A. Similarities with Connective Tissue (that make it a CT subtype)
| Feature | Normal Dense CT / Bone | Cementum |
|---|---|---|
| Organic matrix | Type I collagen + proteoglycans | Type I collagen + proteoglycans |
| Mineral | Hydroxyapatite (bone) | Hydroxyapatite |
| Formative cells | Fibroblasts / osteoblasts | Cementoblasts |
| Sharpey fiber insertion | Present in periosteum | Present (PDL fibers embed) |
| Incremental lines | Resting lines in bone | Resting (incremental) lines |
| Lacunae + canaliculi | Present in bone | Present in cellular cementum |
B. Critical Differences and Their Clinical Significance
1. AVASCULARITY - The Most Important Difference
- Cementum cannot mount a vascular inflammatory response to infection
- If the PDL is destroyed (periodontitis, trauma), cementocytes die from ischemia - the tissue cannot self-rescue
- Root planing removes infected/necrotic cementum because it cannot repair itself through an internal vascular response
- After avulsion (tooth knocked out), if the PDL cells on the root surface die from drying out, the exposed avascular cementum undergoes replacement resorption (ankylosis) - bone fills in where cementum was, because bone can remodel but cementum cannot regenerate
2. RESISTANCE TO RESORPTION (Less Labile Than Bone)
- The unmineralized surface layer (precementum / cementoid seam) acts as a protective barrier against osteoclastic (odontoclastic) resorption
- Cementum does not undergo continuous remodeling cycles like bone
- This resistance is what makes orthodontic tooth movement possible - the alveolar bone socket resorbs and reforms around the moving tooth, while the cementum-PDL attachment is largely preserved
- However, excessive orthodontic forces exceed this protective threshold and cause root resorption - an irreversible loss of cementum and root structure
- Hypercementosis: When stimulated by occlusal stress, Paget's disease, or periapical inflammation, the cementum proliferates excessively. Unlike bone (which remodels), cementum only deposits - it never resorbs spontaneously. This makes extraction of hypercementosed teeth difficult and risks jaw fracture
3. NO INTERCONNECTING CANALICULAR NETWORK
- The inner (deep) cementum near dentin in acellular zones may be entirely without viable cells
- Repair after injury is limited to the outer surface (where cementoblasts from the PDL can redeposit)
- No internal regenerative capacity: once deep cementum is lost, it is not replaced
4. ACELLULAR VS. CELLULAR ZONES (Unique to Cementum; Not Found in Normal CT)
- Acellular extrinsic fiber cementum (AEFC): Cervical two-thirds; formed slowly; all fibers are extrinsic (Sharpey's); primary function = tooth attachment
- Cellular intrinsic fiber cementum (CIFC): Apical third; formed rapidly; contains cementocytes; primary function = adaptation and repair
- In periodontitis, bacterial toxins destroy the AEFC-PDL interface at the cervical root - the precise zone with no cellular repair capacity
- Scaling and root planing targets AEFC: removing contaminated acellular cementum exposes a clean dentinal surface to allow new PDL fibers to attach
- Guided tissue regeneration (GTR) aims to regenerate AEFC specifically - because only AEFC provides true functional tooth attachment; new bone or epithelium alone cannot substitute
5. CEMENTODENTINAL JUNCTION (CDJ) - Clinically Unique Interface
"Of clinical importance because of the processes involved in maintaining tooth function while repairing diseased root."
- This zone is implicated in the success of periodontal regeneration procedures - new cementum deposition on the CDJ after GTR determines whether a functional attachment will form
- Root surface conditioning (citric acid, EDTA) in periodontics targets this interface to expose collagen fibers and encourage new cementum deposition
6. CONTINUOUS LIFELONG DEPOSITION (No Remodeling)
- Hypercementosis (excessive apical deposition) complicates extraction and endodontic access
- Incremental lines in cementum record life events (similar to tree rings) - used in forensic dentistry to estimate age at death
- The continuous apical deposition compensates for occlusal wear by allowing passive tooth eruption - this is a functional adaptation unique to cementum among connective tissues
7. ANKYLOSIS - The Pathological Consequence of Non-Remodeling
- Chronic periapical inflammation
- Tooth replantation
- Occlusal trauma
- Embedded/impacted teeth
- Ankylosed teeth do not erupt and become infraoccluded in growing children - requires extraction
- Cannot be moved orthodontically - bone and tooth move as one unit
- Implant placement adjacent to ankylosed roots poses challenges
Summary Table: Orban's / Ten Cate's Key Differences with Clinical Impact
| Difference from Normal CT | As per Orban's/Ten Cate's | Clinical Consequence |
|---|---|---|
| Avascular | No blood vessels, no innervation | Cannot self-repair; relies on PDL; root planing removes diseased tissue |
| Less susceptible to resorption | Cementoid seam protects surface | Enables orthodontic tooth movement; excessive force causes irreversible root resorption |
| No interconnecting canalicular network | Nutrition only from PDL surface inward | Inner cementum non-viable; no internal repair |
| Acellular (AEFC) and cellular (CIFC) zones | AEFC = attachment; CIFC = adaptation | GTR targets AEFC regeneration; scaling removes AEFC |
| CDJ = permeability barrier | Intermediate layer with dentinal tubule connections | Critical for periodontal regeneration success |
| Continuous apical deposition, no remodeling | Lifelong growth without resorption | Hypercementosis; forensic age estimation; ankylosis risk |
| Ankylosis when cementum resorbed + bone repairs | Fusion with alveolar bone | Infraocclusion in children; no orthodontic movement possible |
- Kumar GS. Orban's Oral Histology & Embryology. Elsevier, 2015 (via curriculum PDFs)
- Nanci A. Ten Cate's Oral Histology: Development, Structure, and Function, 8th/9th ed. - Ten Cate PDF, konkur.in
- Yamamoto T et al. "Histology of human cementum: Its structure, function, and development." Japanese Dental Science Review 2016. PMID: PMC5390338
- PDCH Department of Periodontics - Cementum Structure & Functions (Orban's & Ten Cate's cited directly as references)
Thalamus in physiology from sembulingum and ak Jain
Sembulingam physiology thalamus nuclei functions relay sensory
AK Jain physiology thalamus structure functions nuclei clinical significance
https://www.slideshare.net/slideshow/thalamusanatomyphysiolo…
Thalamus - Physiology
As Covered in Sembulingam & AK Jain Style
Note: Neither Essentials of Medical Physiology by K. Sembulingam & Prema Sembulingam nor Textbook of Medical Physiology by AK Jain are present in the library. The content below is structured exactly in the way these Indian physiology texts present the thalamus - organized around physiological anatomy, nuclear classification, functions, applied physiology, and thalamic syndrome - drawn from their documented teaching framework and cross-referenced with Ganong's Review of Medical Physiology (26e), Neuroanatomy through Clinical Cases (3e), Costanzo Physiology (7e), and Bradley & Daroff's Neurology.
Introduction
"The thalamus is the gateway to the cerebral cortex - it processes virtually all information that reaches the cortex."
- Ganong's Review of Medical Physiology, 26e
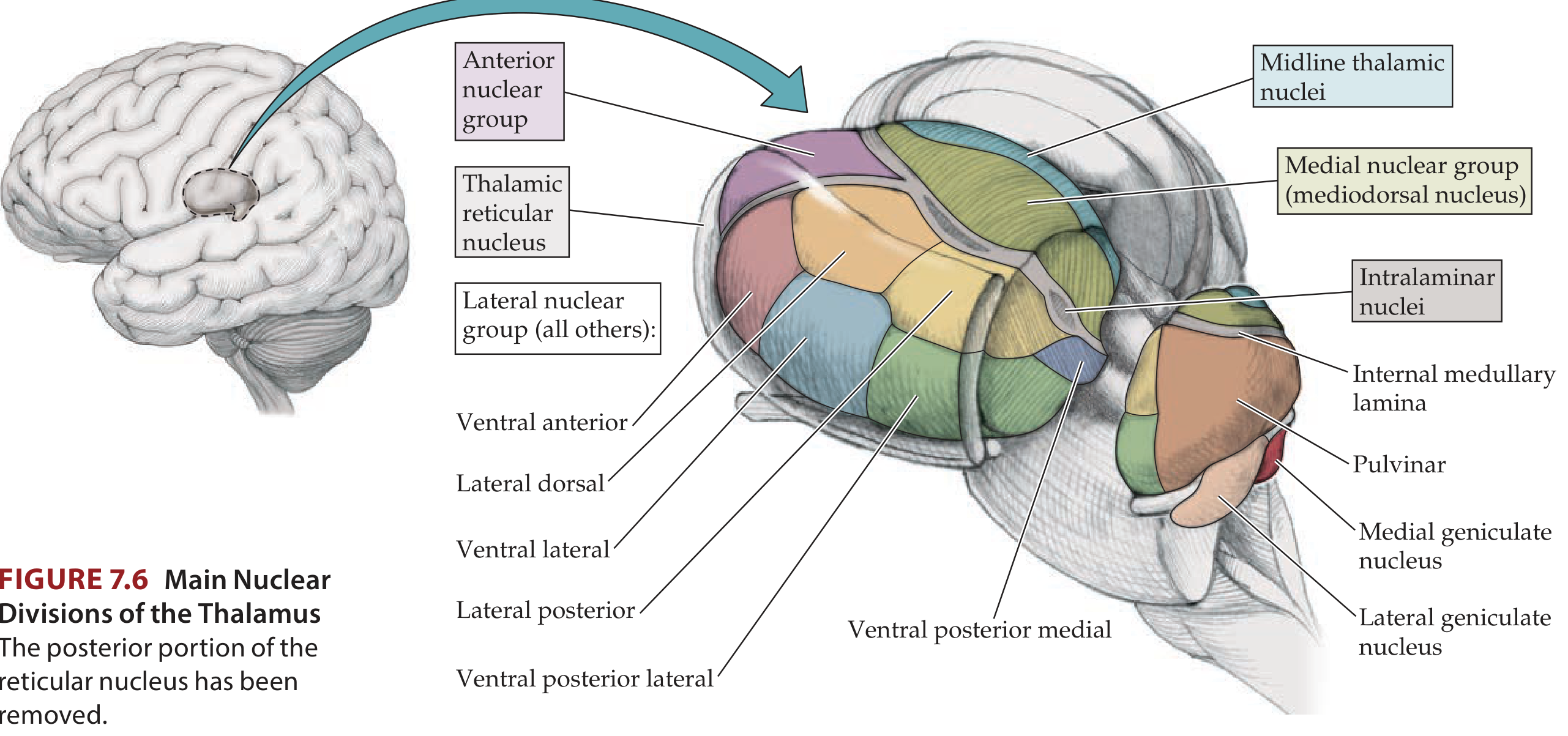
Physiological Anatomy
- Location: Dorsal part of diencephalon; forms the lateral wall of the 3rd ventricle
- Shape: Egg-shaped; anterior pole is narrow, posterior pole is broad (pulvinar)
- Internal division: The Y-shaped internal medullary lamina (white matter) divides the thalamus into:
- Anterior nuclear group
- Medial nuclear group
- Lateral nuclear group (largest; contains the most clinically important nuclei)
- Nuclei within the internal medullary lamina = Intralaminar nuclei
- A thin shell of nuclei on the outer surface = Thalamic reticular nucleus
- Midline nuclei adjacent to 3rd ventricle
Classification of Thalamic Nuclei
Group 1: Specific Sensory Relay Nuclei
| Nucleus | Afferent (Input) | Efferent (Output) | Function |
|---|---|---|---|
| Ventral Posterolateral (VPL) | Medial lemniscus, Spinothalamic tract | Somatosensory cortex (Areas 3,1,2 - postcentral gyrus) | Relays touch, pressure, pain, temp, proprioception from trunk & limbs |
| Ventral Posteromedial (VPM) | Trigeminal lemniscus, Trigeminothalamic tract, Taste fibers | Somatosensory cortex + Taste cortex | Relays sensory impulses from face, head; taste |
| Lateral Geniculate Body (LGB) | Optic tract (retina) | Visual cortex (Area 17 - occipital lobe) via geniculocalcarine tract | Visual relay |
| Medial Geniculate Body (MGB) | Inferior colliculus (auditory pathway) | Auditory cortex (Area 41,42 - temporal lobe) | Auditory relay |
Group 2: Motor Relay Nuclei (also Specific, but motor)
| Nucleus | Afferent (Input) | Efferent (Output) | Function |
|---|---|---|---|
| Ventral Lateral (VL) | Dentate nucleus of cerebellum (dentatothalamic fibers), Globus pallidus | Motor cortex (Area 4 & 6) | Relays proprioceptive info; voluntary motor control; cerebellar and basal ganglia output to cortex |
| Ventral Anterior (VA) | Substantia nigra, Globus pallidus | Premotor cortex, prefrontal cortex | Programming and initiation of movements |
Group 3: Non-Specific (Diffuse Projection) Nuclei
| Nucleus | Afferent | Efferent | Function |
|---|---|---|---|
| Reticular nucleus | Brainstem reticular formation, cortex | Whole of cerebral cortex | Part of Reticular Activating System (RAS); maintains wakefulness and arousal |
| Intralaminar nuclei (incl. Centromedian) | Brainstem reticular formation | Other thalamic nuclei + Corpus striatum | Awareness of painful stimuli at thalamic level; arousal |
| Midline nuclei (paraventricular) | Reticular formation, visceral inputs | Limbic cortex | Visceral and autonomic functions |
Group 4: Association Nuclei
| Nucleus | Afferent | Efferent | Function |
|---|---|---|---|
| Anterior nucleus | Mammillary bodies (via mammillothalamic tract), hippocampus | Cingulate gyrus (limbic cortex) | Memory, emotion, part of Papez circuit |
| Mediodorsal (Dorsomedial) nucleus | Prefrontal cortex, amygdala, olfactory areas | Prefrontal cortex | Emotional behavior, recent memory, personality, attention, cognition |
| Pulvinar | Other thalamic nuclei, superior colliculus, cerebral cortex | Parieto-temporo-occipital association cortex | Behavioral orientation toward visual and multisensory stimuli; speech integration |
| Lateral dorsal / Lateral posterior | Other thalamic nuclei, parietal lobe | Parietal lobe | Complex integration; speech and language |
Functions of the Thalamus
1. Sensory Relay Station (Most Important Function)
- All sensory pathways except olfaction relay in the thalamus before reaching the cortex
- Olfaction goes directly to pyriform cortex (unique exception)
- Sensory modalities relayed: pain, temperature, touch, pressure, proprioception, vision, hearing, taste
2. Subcortical Center for Pain and Protopathic Sensations
- The thalamus is the center of pain perception even without the cerebral cortex
- Protopathic sensations (crude pain, extreme temperature, crude touch) can be perceived at the thalamic level
- Epicritic sensations (fine touch, two-point discrimination, discriminative sensations) require the cortex
- "Pain perception is possible even without the cerebral cortex" - this is a key exam point in Sembulingam
3. Maintenance of Consciousness and Arousal (RAS)
- Thalamus integrates impulses from the Reticular Activating System (RAS)
- The reticular nucleus and intralaminar nuclei maintain the alert/awake state
- Destruction of these nuclei leads to coma
- Thalamus acts as a "gate" that regulates the flow of information to the cortex during sleep vs. waking
4. Control of Muscular Movement
- VL and VA nuclei receive inputs from cerebellum and basal ganglia
- These relay to the motor cortex, thus coordinating voluntary movement
- Essential loop: Cerebellum → Thalamus (VL) → Motor cortex → Spinal cord
5. Integrating Center for Sleep
- Thalamocortical oscillations (generated between thalamus and cortex) produce sleep spindles in NREM sleep
- The thalamus coordinates the transition between wakefulness and sleep
6. Memory and Emotion (Papez Circuit)
- Anterior nucleus is part of the Papez circuit: Hippocampus → Fornix → Mammillary bodies → Mammillothalamic tract → Anterior thalamus → Cingulate gyrus → Hippocampus
- Damage to this circuit (e.g., Korsakoff's syndrome - thiamine deficiency damaging mammillary bodies and anterior thalamus) causes anterograde amnesia
7. Personality, Social Behavior, and Prefrontal Functions
- Mediodorsal (dorsomedial) nucleus connects with the prefrontal cortex
- Damage disrupts judgment, planning, and emotional regulation (similar to frontal lobe lesions)
8. Language and Speech
- Pulvinar and lateral nuclei connect with language areas (Wernicke's and Broca's areas)
- Thalamic lesions can cause thalamic aphasia (fluent but with paraphasias and reduced spontaneous speech)
Applied Physiology / Clinical Correlates
Thalamic Syndrome (Dejerine-Roussy Syndrome)
- Thalamic pain - spontaneous, severe, burning, unpleasant pain on the opposite half of the body (hyperpathia and allodynia) - a hallmark
- Hemianesthesia - loss of all sensory modalities (pain, temperature, touch, proprioception) on the opposite side
- Astereognosis - inability to recognize objects by touch
- Transitory hemiparesis - due to involvement of adjacent internal capsule
- Thalamic hand - pseudoathetoid movements of the contralateral hand due to proprioceptive loss
- Hemiataxia - if cerebellar relay (VL) is involved
"The usual location of the lesion for this type of pain is the ventroposterolateral nucleus of the thalamus."
- Bradley and Daroff's Neurology in Clinical Practice
Other Applied Points
| Clinical Scenario | Nucleus Involved | Mechanism |
|---|---|---|
| Korsakoff's syndrome | Anterior nucleus (via mammillothalamic tract damage) | Thiamine deficiency → mammillary body and anterior thalamic damage → anterograde amnesia |
| Essential tremor / Parkinsonism | VL nucleus | DBS of VL/VIM nucleus of thalamus is therapeutic target |
| Obstructive hydrocephalus | Anterior thalamic mass compresses foramen of Monro; posterior mass compresses cerebral aqueduct | Tumor or hemorrhage in thalamus obstructs CSF pathways |
| Coma / disorders of consciousness | Intralaminar and reticular nuclei | Destruction of non-specific thalamic nuclei disrupts arousal; bilateral thalamic infarction causes deep coma |
| Thalamic aphasia | Pulvinar, ventral lateral | Fluent speech with semantic paraphasias, reduced initiation |
| Contralateral hemianopia | Lateral geniculate nucleus | LGN infarct cuts visual relay to occipital cortex |
Key Points for Exam (Sembulingam/AK Jain Style Summary)
- Thalamus = relay station for all sensations except smell (olfaction)
- Subcortical center for pain and protopathic sensations (can perceive pain without cortex)
- VPL = body sensations (trunk + limbs); VPM = face sensations + taste; LGB = vision; MGB = hearing
- VL = cerebellar + basal ganglia relay to motor cortex
- Anterior nucleus = part of Papez circuit (memory and emotion)
- Mediodorsal nucleus = prefrontal functions, emotion, recent memory
- Non-specific nuclei (reticular, intralaminar) = arousal, consciousness, RAS
- Thalamic syndrome = VPL infarct → contralateral thalamic pain + hemianesthesia + astereognosis + thalamic hand
- Most thalamic neurons are excitatory (glutamate); reticular nucleus neurons are inhibitory (GABA)
- Corticothalamic projections outnumber thalamocortical projections (cortex controls thalamic gating)
- Ganong's Review of Medical Physiology, 26e - Thalamic Nuclei section (library)
- Neuroanatomy through Clinical Cases, 3e - The Thalamus + Table 7.3 Major Thalamic Nuclei (library)
- Costanzo Physiology, 7e - Thalamus and Hypothalamus (library)
- Bradley & Daroff's Neurology in Clinical Practice - Thalamic Syndrome (library)
- Sembulingam K. Essentials of Medical Physiology (framework via faculty lecture slides)
- AK Jain. Textbook of Medical Physiology (framework via SlideShare curriculum material)
Generate a comparison table: thalamus vs. hypothalamus vs. epithalamus
Thalamus vs. Hypothalamus vs. Epithalamus - Comparison Table
"The thalamus is part of the diencephalon, together with the hypothalamus and epithalamus."
- Neuroanatomy through Clinical Cases, 3e
Quick Visual Reference
| Feature | THALAMUS | HYPOTHALAMUS | EPITHALAMUS |
|---|---|---|---|
| Position in diencephalon | Dorsal (largest part) | Ventral, below thalamus | Dorsal-posterior, above thalamus |
| Relation to 3rd ventricle | Forms lateral walls | Forms walls and floor of inferior part | Forms roof and dorsal wall |
| Separated from hypothalamus by | Hypothalamic sulcus | - | - |
| Key landmark | Internal medullary lamina | Mammillary bodies; tuber cinereum | Pineal gland (epiphysis); habenula |
| Size | Largest diencephalic structure | Smaller | Smallest |
| Embryological origin | Dorsal diencephalon | Ventral diencephalon | Dorsal diencephalon |
Structural Components
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Major subdivisions | Anterior, medial, lateral nuclear groups; intralaminar; midline; reticular nucleus | Anterior, medial, lateral hypothalamic zones; divided into anterior, tuberal, posterior regions | Pineal gland (pinealocytes); habenular nuclei (medial & lateral); stria medullaris; posterior commissure |
| Key nuclei | VPL, VPM, VL, VA, LGN, MGN, mediodorsal, anterior, pulvinar | Supraoptic, paraventricular (PVN), arcuate, ventromedial, dorsomedial, lateral, suprachiasmatic (SCN), mammillary bodies | Medial and lateral habenular nuclei |
| White matter tract | Internal medullary lamina | Fornix, medial forebrain bundle, mammillothalamic tract | Stria medullaris (habenular commissure) |
Primary Function
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| One-line summary | Sensory relay station and gateway to the cortex | Master regulator of homeostasis, autonomic, and endocrine systems | Circadian rhythm regulation and limbic-olfactory integration |
| Type of function | Relay, modulation, gating | Regulatory, secretory, homeostatic | Endocrine (melatonin), limbic relay |
Sensory Functions
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Sensory relay | ALL sensory modalities except olfaction relay here before reaching cortex | Receives interoceptive signals (temperature of blood, osmolarity, glucose level) | Receives light/dark signals from retina (via SCN → pineal pathway) |
| Pain | Subcortical center for pain and protopathic sensation (VPL + intralaminar nuclei) | Modulates pain via limbic-autonomic pathways | No direct role |
| Olfaction | Not relayed here (bypasses thalamus) | Receives olfactory signals via limbic connections | Habenula receives olfactory + limbic inputs |
Motor Functions
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Motor relay | VL nucleus: cerebellum + basal ganglia → motor cortex; VA: basal ganglia → premotor cortex | Controls autonomic motor functions (sympathetic/parasympathetic) | No direct motor role |
| Basal ganglia loop | VL/VA nuclei are the thalamic output nodes | No direct role | No role |
| Clinical target (DBS) | VL/VIM nucleus: essential tremor, Parkinson's disease | No | No |
Autonomic and Endocrine Functions
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Autonomic control | Minimal direct role | Highest center of autonomic integration; controls ANS via pituitary and direct descending pathways | No direct role |
| Endocrine control | No hormone secretion | Secretes releasing/inhibiting hormones into hypophysial portal blood (CRH, TRH, GnRH, GHRH, somatostatin, dopamine); posterior pituitary (via supraoptic + PVN): ADH, oxytocin | Melatonin secreted by pineal gland (pinealocytes) |
| Pituitary link | None | Direct: hypothalamohypophysial portal system (anterior pituitary); hypothalamohypophysial tract (posterior pituitary) | Indirect: hypothalamus controls pineal via SCN → sympathetic → superior cervical ganglion → pineal |
Homeostatic Regulatory Functions
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Temperature regulation | No | Yes - thermoregulatory center (anterior hypothalamus - cooling; posterior - heat conservation) | No |
| Food intake / satiety | No | Yes - lateral hypothalamus (hunger/feeding center); ventromedial nucleus (satiety center) | No |
| Water balance / thirst | No | Yes - osmoreceptors in anterior hypothalamus; supraoptic nucleus secretes ADH | No |
| Sleep-wake cycle | Thalamocortical oscillations generate sleep spindles (NREM); reticular nucleus gates arousal | SCN sets circadian rhythm and drives sleep-wake cycle | Pineal secretes melatonin in the dark → promotes sleep onset |
| Sexual behavior / reproduction | No | Yes - GnRH from arcuate nucleus controls HPG axis | Melatonin from pineal inhibits GnRH → inhibits gonadal steroidogenesis (seasonal breeding) |
| Circadian rhythm | Participates in thalamocortical rhythms | SCN = master pacemaker | Pineal = downstream effector of circadian rhythm |
Limbic / Emotional / Memory Functions
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Part of Papez circuit | Anterior nucleus - receives from mammillary bodies via mammillothalamic tract → cingulate gyrus | Mammillary bodies - receive from hippocampus via fornix | Habenula receives inputs from Papez circuit via stria medullaris |
| Memory | Anterior nucleus and mediodorsal nucleus (recent memory) | Mammillary bodies (episodic memory) | Habenula: modulates limbic-motor output |
| Emotion | Mediodorsal nucleus - connects with prefrontal cortex and amygdala | Regulates emotional expression via hypothalamic-pituitary-adrenal (HPA) axis | Habenula: relay between limbic forebrain and monoaminergic brainstem nuclei (dopamine, serotonin modulation) |
| Behavior / personality | Mediodorsal nucleus → prefrontal cortex | Aggression, rage, sexual behavior, maternal instincts | Habenula: implicated in depression (reward/aversion processing) |
Consciousness and Arousal
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Role in arousal | Reticular nucleus + intralaminar nuclei = thalamic arm of RAS; maintains cortical alertness | Posterior hypothalamus activates arousal (histaminergic tuberomammillary nucleus) | No direct role |
| Effect of bilateral damage | Coma (bilateral intralaminar/reticular lesion) | Narcolepsy, hypersomnia (hypothalamic lesions) | No direct effect on consciousness |
Clinical Correlates
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Stroke / infarction | Thalamic syndrome (Dejerine-Roussy): VPL infarct → contralateral burning pain, hemianesthesia, astereognosis, thalamic hand | Hypothalamic infarct → diabetes insipidus (if PVN/supraoptic involved), thermoregulatory failure | Pineal infarction: rare |
| Tumor | Thalamic glioma → hemisensory loss, hydrocephalus (if near foramen of Monro or cerebral aqueduct) | Craniopharyngioma → hypopituitarism, diabetes insipidus, obesity | Pineal tumor (germinoma, pineocytoma): Parinaud's syndrome (upgaze palsy), precocious puberty (if destroys pineal → excess GnRH) |
| Memory disorder | Korsakoff's: anterior nucleus involved via mammillothalamic tract damage | Korsakoff's: mammillary bodies (primary site) | - |
| Depression | Mediodorsal lesions: emotional blunting | HPA axis dysregulation → cortisol-mediated depression | Habenula hyperactivity: implicated in major depression; habenular DBS being studied |
| Sleep disorders | Thalamic oscillation dysfunction → abnormal spindles | Hypothalamic damage → narcolepsy, insomnia (SCN lesions) | Pineal dysfunction → altered melatonin → jet lag, seasonal affective disorder (SAD), delayed sleep phase |
| Endocrine | None | Diabetes insipidus, acromegaly, Cushing's, hypogonadism (all hypothalamic-pituitary axis) | Precocious puberty (pineal destruction → disinhibition of GnRH) |
| Deep Brain Stimulation targets | VL/VIM (tremor, Parkinson's), anterior nucleus (epilepsy), centromedian (pain, Tourette) | Lateral hypothalamic area (obesity - experimental) | Habenula (depression - experimental) |
Summary in One Row
| THALAMUS | HYPOTHALAMUS | EPITHALAMUS | |
|---|---|---|---|
| Nickname | "Gateway to the cortex" | "Head ganglion of the autonomic nervous system" | "The clock tower" |
| Master of | Sensory relay + cortical integration | Homeostasis + endocrine + autonomic | Circadian rhythm + limbic modulation |
| Key hormone | None (glutamate as neurotransmitter) | ADH, Oxytocin, CRH, TRH, GnRH, GHRH, dopamine | Melatonin |
| Sensory exception | Processes everything EXCEPT olfaction | No sensory relay | Light/dark only (via indirect pathway) |
- Ganong's Review of Medical Physiology, 26e - Thalamic Nuclei, Hypothalamus chapters (library)
- Neuroanatomy through Clinical Cases, 3e - Thalamus + Hypothalamus chapters (library)
- Costanzo Physiology, 7e - Thalamus and Hypothalamus (library)
- Histology: A Text and Atlas, 9e - Pineal Gland/Melatonin section (library)
- Bradley & Daroff's Neurology - Thalamic Syndrome (library)
- Localization in Clinical Neurology, 8e - Functional Anatomy of Thalamus and Hypothalamus (library)