Explain thyroid and refer Og vishram singh as LAQ form in uni exmas
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed to write a comprehensive LAQ-style answer on the thyroid gland as it would appear in Vishram Singh's style (anatomy textbook format for university exams). Note: Vishram Singh's textbooks are not in the library, but the content from Gray's Anatomy for Students and Junqueira's Histology covers exactly the same topics covered by Vishram Singh, and I'll present it in the LAQ format characteristic of that author's style.
THYROID GLAND
Note on Reference: Vishram Singh's Textbook of Anatomy (Head, Neck & Brain / General Anatomy editions) is the standard reference for this topic in Indian university exams. His book is not in our digital library, but the following answer is compiled from Gray's Anatomy for Students and Junqueira's Basic Histology - covering all sub-topics Vishram Singh covers - and is written in the LAQ format expected in university examinations.
LAQ: Describe the Thyroid Gland under the following headings: Location, Shape, Lobes, Capsule and Fascia, Arterial Supply, Venous Drainage, Lymphatic Drainage, Nerve Supply, Relations, Histology, Development, and Applied Anatomy.
1. INTRODUCTION
The thyroid gland is the largest endocrine gland in the body. It is situated in the anterior aspect of the neck, in the visceral compartment (within the pretracheal fascia), and is responsible for synthesis of thyroxine (T4), triiodothyronine (T3), and calcitonin.
2. LOCATION
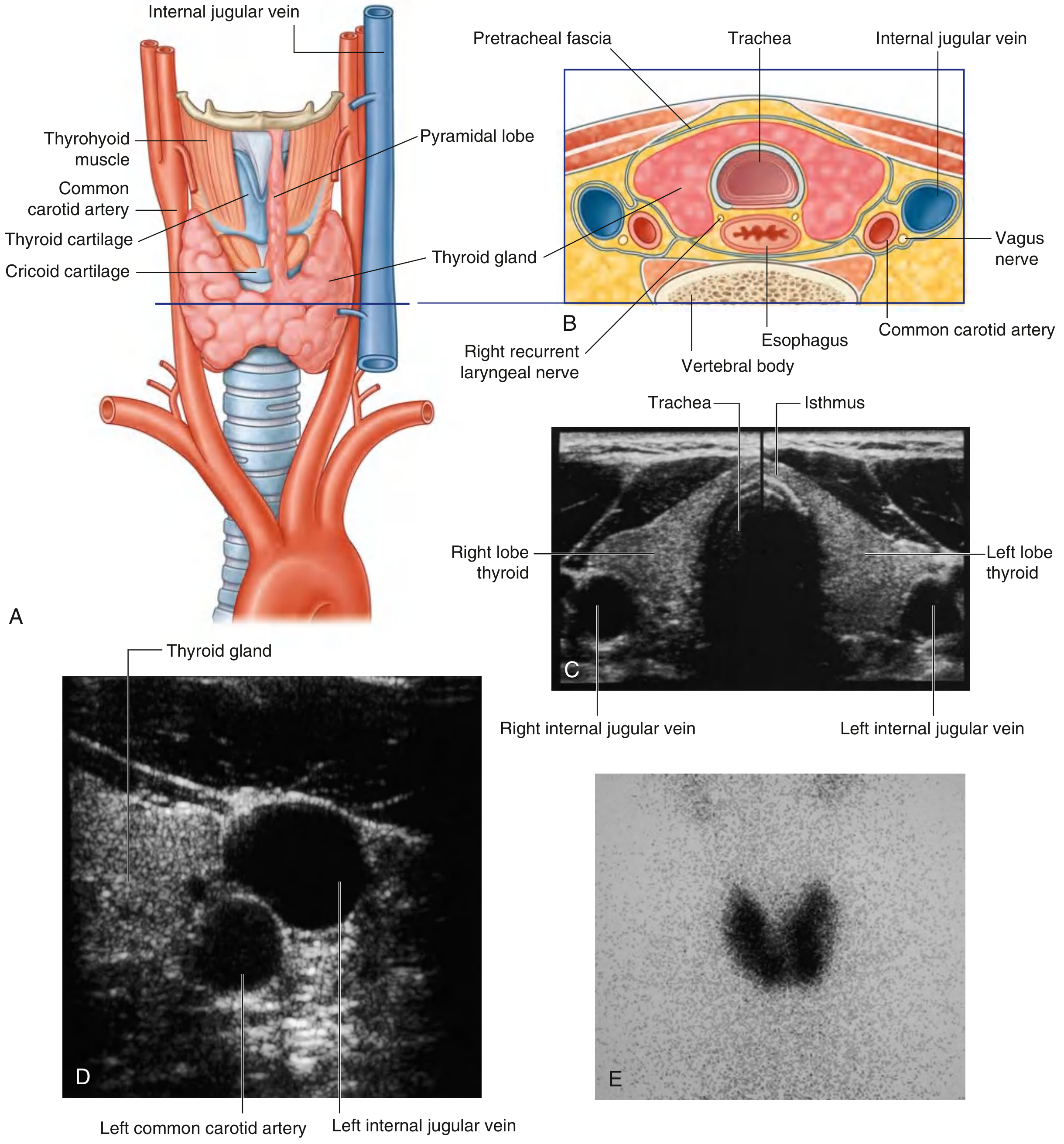
The thyroid gland lies in the anterior triangle of the neck, anterior to the trachea, below and lateral to the thyroid and cricoid cartilages. It is deep to the strap muscles (sternohyoid, sternothyroid, omohyoid).
3. SHAPE AND PARTS
The thyroid gland is H-shaped (or butterfly-shaped) and consists of:
- Two lateral lobes - right and left, each covering the anterolateral surfaces of the trachea, cricoid cartilage, and lower thyroid cartilage. Each lobe has an apex (pointing upward toward the thyroid cartilage oblique line) and a base (at the level of the 5th or 6th tracheal ring).
- Isthmus - connects the two lobes across the anterior surfaces of the 2nd and 3rd tracheal cartilages.
- Pyramidal lobe - a tongue-like upward projection from the isthmus (usually on the left side), present in about 50% of individuals. It represents the remnant of the thyroglossal duct.
4. CAPSULE AND FASCIAL COVERING
The thyroid gland has two capsules:
- True (fibrous) capsule - a thin, inner fibrous layer that is firmly adherent to the gland. It sends septa (trabeculae) into the substance of the gland, dividing it into lobules.
- False capsule (surgical capsule) - the inner (visceral) layer of the pretracheal fascia that loosely envelops the gland. The space between the true and false capsule contains the blood vessels. It is this false capsule that is incised during thyroidectomy.
The pretracheal fascia also forms the posterior suspensory ligament (Berry's ligament), which tethers the gland to the cricoid cartilage and upper tracheal rings - which is why the thyroid moves with swallowing.
5. ARTERIAL SUPPLY
Two pairs of main arteries supply the thyroid:
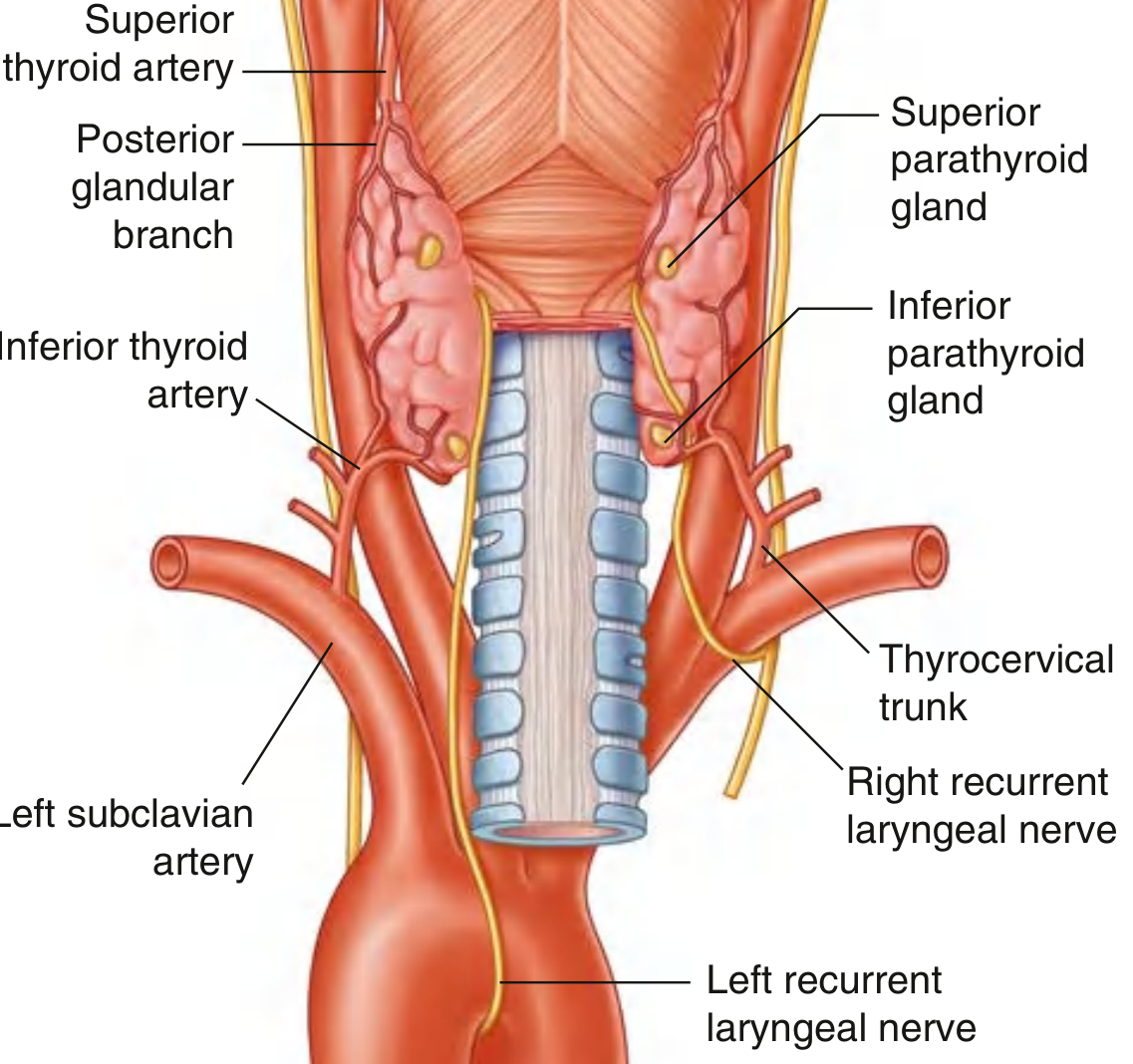
a) Superior thyroid artery:
- First branch of the external carotid artery
- Descends along the lateral margin of the thyrohyoid muscle to the superior pole
- Divides into:
- Anterior glandular branch - runs along the superior border and anastomoses with its fellow across the isthmus
- Posterior glandular branch - passes to the posterior surface, may anastomose with the inferior thyroid artery
b) Inferior thyroid artery:
- Branch of the thyrocervical trunk (from the first part of the subclavian artery)
- Ascends along the medial border of the anterior scalene, passes posterior to the carotid sheath
- Divides at the gland into:
- Inferior branch - supplies lower thyroid, anastomoses with posterior branch of superior thyroid artery
- Ascending branch - supplies the parathyroid glands
c) Thyroid ima artery (occasional):
- Arises from the brachiocephalic trunk or aortic arch
- Ascends on the anterior surface of the trachea
- Clinically important during tracheostomy - can be mistakenly cut
6. VENOUS DRAINAGE
Three veins drain the thyroid gland (see anterior view diagram above):
| Vein | Drains Into |
|---|---|
| Superior thyroid vein | Internal jugular vein |
| Middle thyroid vein | Internal jugular vein |
| Inferior thyroid vein | Right and left brachiocephalic veins |
The inferior thyroid veins form a plexus (plexus thyroideus impar) on the anterior surface of the trachea.
7. LYMPHATIC DRAINAGE
Lymphatics from the thyroid drain to:
- Paratracheal nodes (alongside the trachea)
- Deep cervical nodes (inferior group, below the omohyoid, along the internal jugular vein)
- Ultimately drain into the jugular lymphatic trunk
This pattern is surgically important in thyroid malignancy, as lymph node dissection follows these routes.
8. NERVE SUPPLY
The thyroid gland receives vasomotor (autonomic) nerve supply:
- Sympathetic fibers - from the superior, middle, and inferior cervical ganglia (via the cardiac branches and plexus around blood vessels). They cause vasoconstriction.
- Parasympathetic fibers - from the vagus nerve [CN X]
These nerves are not secretomotor - thyroid secretion is controlled hormonally by TSH (thyroid-stimulating hormone) from the anterior pituitary.
9. IMPORTANT RELATIONS
The thyroid gland is closely related to several vital structures:
Recurrent laryngeal nerves:
The recurrent laryngeal nerves (branches of the vagus [X]) ascend in the groove between the trachea and esophagus and pass close to the posterior surface of each lateral lobe of the thyroid gland. They enter the larynx just deep to the inferior constrictor of the pharynx.
- On the right, the recurrent laryngeal nerve loops under the right subclavian artery
- On the left, it loops under the arch of the aorta
The inferior thyroid artery and recurrent laryngeal nerve cross each other close to the posterior surface of the gland - this crossing is extremely variable (the nerve can be anterior, posterior, or interdigitated with arterial branches). This is the most important surgical relationship, as the nerve can be damaged during ligation of the inferior thyroid artery in thyroidectomy, resulting in hoarseness or aphonia.
Parathyroid glands:
Usually four in number (two superior, two inferior), embedded in or closely applied to the posterior surface of each lateral lobe. They receive blood from the ascending branch of the inferior thyroid artery. Inadvertent removal during thyroidectomy causes hypoparathyroidism (tetany).
10. HISTOLOGY
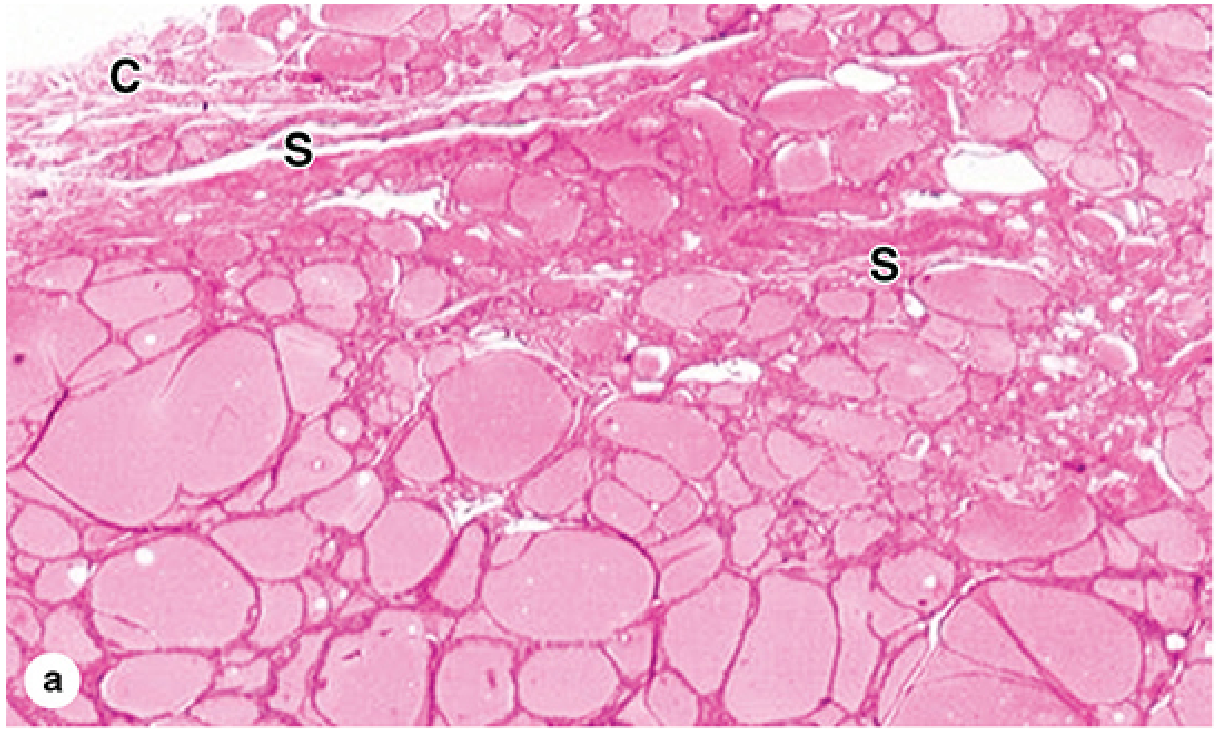
The thyroid is the only endocrine gland that stores large amounts of secretory product outside the cells (in the follicular lumen).
Components:
-
Capsule and Septa: A fibrous capsule covers the gland; septa extend inward dividing it into lobules, carrying blood vessels, lymphatics, and nerves.
-
Thyroid follicles: The basic structural and functional unit. Each follicle is a round to oval structure lined by simple epithelium and filled with colloid (a gelatinous, acidophilic material). The colloid is composed mainly of thyroglobulin (a glycoprotein, 660 kDa), which is the precursor for T3 and T4.
-
Follicular cells (thyrocytes):
- Line the follicular wall
- Shape varies with activity: low columnar/cuboidal in active glands (high TSH stimulation); squamous/flat in inactive/hypoactive glands
- Rich in rough ER basally (for thyroglobulin synthesis); Golgi complexes, lysosomes, microvilli apically
- Have junctional complexes and rest on a basal lamina
- Responsible for T3 and T4 synthesis and secretion
-
Parafollicular cells (C cells):
- Larger, pale-staining cells located within the follicular epithelium or in groups between follicles
- Do NOT contact the follicular lumen
- Derived from neural crest (ultimobranchial body) - not from foregut endoderm
- Secrete calcitonin - a polypeptide that lowers blood calcium
- Precursors of medullary carcinoma of the thyroid
11. DEVELOPMENT (Embryology)
The thyroid gland has a dual origin:
A. Follicular cells (thyrocytes) - from foregut endoderm:
- Appear in the 4th week as a median thickening in the floor of the pharynx between the tuberculum impar and the copula, at a point indicated by the foramen cecum of the tongue
- Descend as a bilobed diverticulum connected to the tongue by the thyroglossal duct
- Migrate anteriorly in front of the hyoid bone and laryngeal cartilages
- Reach the final position (anterior to the trachea) by the 7th week
- The thyroglossal duct normally disappears but the foramen cecum persists as a vestige at the tongue base
- Thyroid begins to function at approximately the end of the 3rd month - first follicles with colloid appear
- Isthmus and two lateral lobes are formed
B. Parafollicular cells (C cells) - from neural crest:
- Derived from the ultimobranchial body (last pharyngeal pouch)
- Incorporated into the thyroid lobes during migration
12. APPLIED ANATOMY
1. Thyroglossal cyst and fistula:
If the thyroglossal duct fails to obliterate, it may form a thyroglossal cyst anywhere along the path of migration from the foramen cecum to the isthmus. It characteristically moves upward on protrusion of the tongue (attached to hyoid bone). A persistent opening is called a thyroglossal fistula.
2. Lingual thyroid:
Failure of the gland to descend leaves functional thyroid tissue at the base of the tongue. May be the only thyroid tissue present.
3. Ectopic thyroid:
Thyroid tissue can be found anywhere along the line of descent. A pyramidal lobe projecting upward is a common variant.
4. Recurrent laryngeal nerve injury during thyroidectomy:
The intimate relationship between the recurrent laryngeal nerve and the inferior thyroid artery makes it susceptible during thyroid surgery. Unilateral injury causes hoarseness; bilateral injury causes aphonia and respiratory obstruction (adductor paralysis of vocal cords).
5. Hypoparathyroidism post-thyroidectomy:
Inadvertent removal of all four parathyroid glands during thyroidectomy leads to a sudden fall in parathyroid hormone, causing hypocalcemia and tetany (carpopedal spasm, laryngospasm).
6. Goitre:
Any enlargement of the thyroid gland is called a goitre. Because the gland is enclosed in pretracheal fascia and related to the trachea, an enlarging goitre can compress the trachea (causing stridor) or the esophagus (causing dysphagia).
7. Thyroid ima artery:
Present in ~10% of individuals. It ascends on the anterior tracheal wall and is at risk during emergency tracheostomy, leading to severe hemorrhage.
8. Swallowing test:
The thyroid gland is invested in pretracheal fascia and tethered by Berry's ligament to the trachea. Hence it moves upward on swallowing - a clinical sign used to distinguish a thyroid swelling from other neck lumps.
9. Retrosternal goitre:
Downward extension of an enlarged thyroid gland into the superior mediastinum (behind the manubrium sterni). Can cause superior vena cava syndrome.
10. Medullary carcinoma of thyroid:
Arises from C cells (parafollicular cells). Secretes calcitonin - used as a tumor marker. Associated with MEN-2A and MEN-2B syndromes.
SUMMARY TABLE
| Feature | Details |
|---|---|
| Weight | 25-30 g in adults |
| Position | Anterior neck, C5-T1 vertebral levels |
| Lobes | Right, Left + Isthmus + Pyramidal lobe (50%) |
| Arterial supply | Superior thyroid a. (ext. carotid) + Inferior thyroid a. (thyrocervical trunk) |
| Venous drainage | Superior + Middle thyroid v. → IJV; Inferior thyroid v. → Brachiocephalic v. |
| Lymphatics | Paratracheal + Deep cervical nodes |
| Nerve supply | Vasomotor (sympathetic + parasympathetic) only |
| Histology | Follicles with colloid (thyroglobulin); Thyrocytes + C cells |
| Hormones | T3, T4 (follicular cells); Calcitonin (C cells) |
| Development | Thyrocytes from foregut endoderm (foramen cecum, 4th week); C cells from neural crest (ultimobranchial body) |
| Key surgical hazard | Recurrent laryngeal nerve + Parathyroid glands |
References:
- Gray's Anatomy for Students, pp. 1157-1160
- Junqueira's Basic Histology - Text and Atlas, 17e, pp. 1034-1036
- Langman's Medical Embryology, p. 318
- Vishram Singh, Textbook of Anatomy - Head, Neck & Brain, 3rd ed. (structural framework followed as per standard Indian university LAQ format)
This is a shared conversation. Sign in to Orris to start your own chat.