Metabolic response to injury
Reading File
Finding Sources
Searching PubMed
metabolic response to injury surgery
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative surgical textbooks and two key diagrams. Let me compile the full answer.
Metabolic Response to Injury
The metabolic response to injury is a coordinated, whole-body reaction to tissue damage that involves neuroendocrine, inflammatory, and immunological changes. It is designed to preserve homeostasis and promote survival and repair, but when excessive or prolonged, it causes catabolism, organ failure, and death.
1. The Phases: Ebb and Flow (Cuthbertson, 1930s)
Sir David Cuthbertson first described two distinct phases:
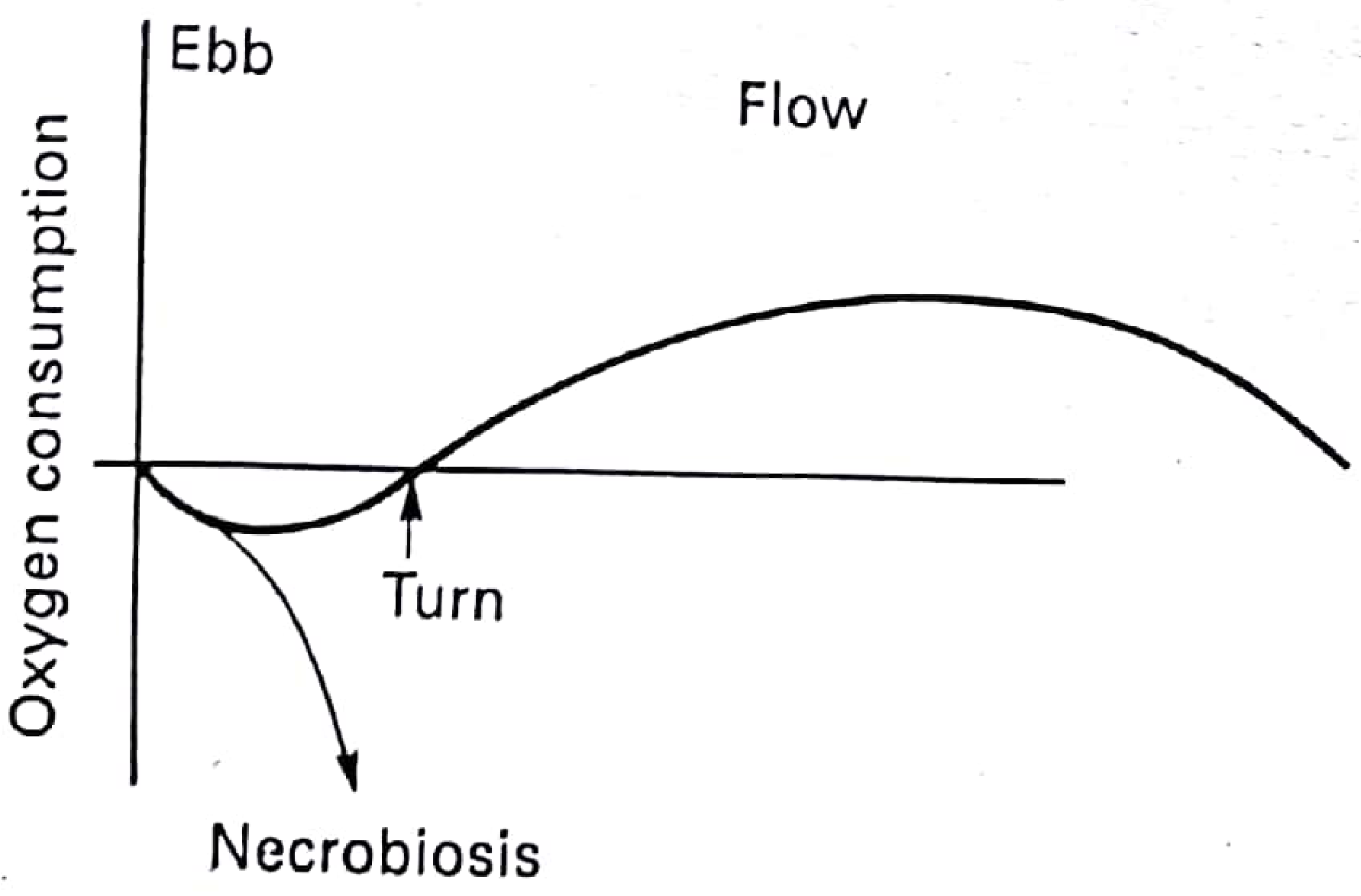
| Phase | Timing | Features |
|---|---|---|
| Ebb phase | First few hours post-injury | Fall in oxygen consumption, hypometabolism, hypothermia, reduced cardiac output, shock. If the patient is not resuscitated, this continues to death (necrobiosis). |
| Turn | After successful resuscitation | Transition point where metabolic trajectory reverses |
| Flow phase | Hours to weeks post-injury | Hypermetabolism, increased O2 consumption, fever, catabolism, sodium/water retention, potassium and protein loss |
The magnitude of the response is graded - proportional to the severity of injury:
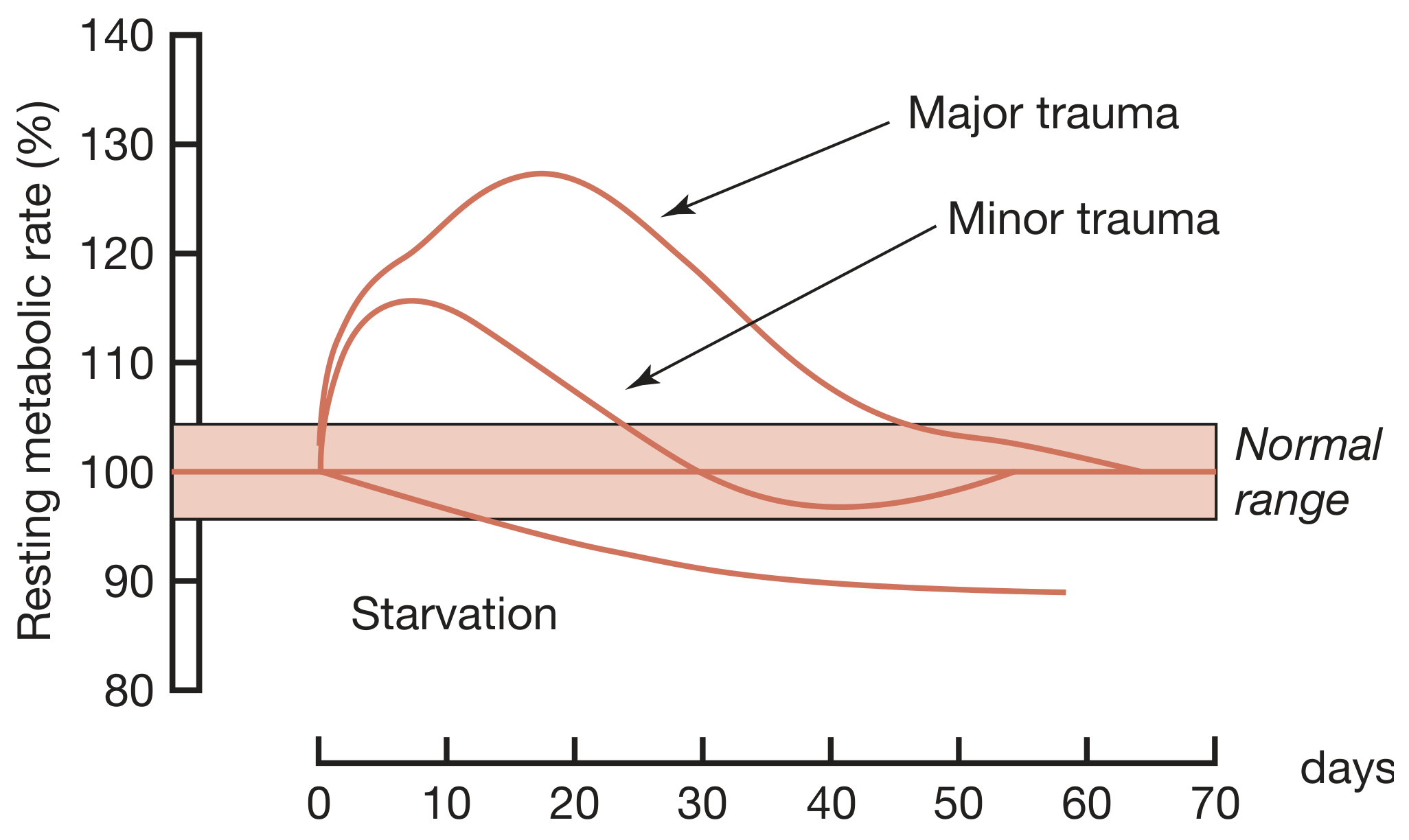
- Minor elective surgery: transient rise lasting ~5 days
- Fractured femur: ~2 weeks
- Major burns: months, with metabolic rate up to twice normal if sepsis is superimposed
- Genetic variability also determines individual response intensity
2. Mediators of the Metabolic Response
A. Tissue Damage Signals (DAMPs)
Tissue injury releases damage-associated molecular patterns (DAMPs) - also called alarmins - including:
- Heat shock proteins
- High mobility group protein B1 (HMGB1)
- S100 proteins
- Nucleic acid fragments
These are sensed by pattern recognition receptors (PRRs) - primarily Toll-like receptors (TLRs) and NOD-like receptors (NLRs) - on macrophages, neutrophils, and dendritic cells. PRR activation triggers:
- Inflammasome formation → caspase activation → IL-1β and IL-18 release
- Cytokine release: TNF-α, IL-1, IL-6, IL-8, interferons, chemokines
- Complement and kinin pathway activation
- DAMPs are self-perpetuating: sepsis, haemorrhage, massive transfusion, acidosis, crush syndrome, and ischaemia-reperfusion all trigger further DAMP release, amplifying the cascade.
B. Neuroendocrine Response
The stress response runs through: nociceptive afferents → spinal cord → thalamus → hypothalamus → pituitary
Acute phase (hours):
- Hypothalamic release of corticotropin-releasing factor (CRF)
- Anterior pituitary releases ACTH → adrenal cortex secretes cortisol (within hours of injury)
- Hypothalamic sympathetic activation → adrenal medulla releases adrenaline (epinephrine) and noradrenaline
- Glucagon and growth hormone (GH) are also elevated
- These "counter-regulatory" hormones together liberate glucose from carbohydrate stores and break down fat and protein
- GH has direct lipolytic, insulin-antagonising, and pro-inflammatory properties
Chronic phase (days):
- Hypothalamic suppression occurs
- Low serum levels of target organ hormones (e.g., IGF-1, thyroid hormones, gonadal hormones)
- May contribute to chronic wasting
Other hormonal changes include:
- Hypersecretion of prolactin and GH with low IGF-1
- Peripheral inactivation of thyroid hormones
- Gonadal suppression
- Aldosterone and ADH release → Na+ and water retention
3. Metabolic Changes
Carbohydrate Metabolism
- Accelerated gluconeogenesis (from amino acids, lactate, glycerol)
- Peripheral insulin resistance (correlates with the magnitude of the operation)
- Hyperglycaemia - the so-called "pseudodiabetes of injury"
- Hyperglycaemia itself aggravates inflammation by generating excess oxygen free radicals in mitochondria and enhancing cytokine production
Protein Metabolism
- Skeletal muscle proteolysis driven by cortisol, TNF-α, IL-1, IL-6
- Amino acids used as gluconeogenic substrates
- Net negative nitrogen balance
- Increased hepatic acute-phase protein synthesis (CRP, fibrinogen, complement, coagulation factors)
- In critical illness, protein losses may exceed 1 kg/day of lean body mass
Fat Metabolism
- Lipolysis activated by catecholamines and glucagon
- Free fatty acids and triglycerides become the principal fuel source
- Fat stores are mobilised to fuel the hypermetabolic state
- Ketogenesis is relatively suppressed (unlike in starvation)
Starvation vs. Injury - Key Distinction
| Feature | Starvation | Injury |
|---|---|---|
| Metabolic rate | Decreased (~90% of normal) | Increased (110-130%+ of normal) |
| Primary fuel | Fat/ketones | Mixed: glucose + fat + protein |
| Protein catabolism | Conserved after adaptation | Sustained and marked |
| Insulin sensitivity | Preserved | Resistant |
| Nitrogen loss | Moderate, decreasing | High, sustained |
4. Fluid and Electrolyte Changes
- Sodium and water retention (aldosterone + ADH)
- Potassium loss (intracellular K+ released with protein catabolism)
- These can be monitored by daily fluid balance and 24-hour urine Na+, K+, and urea
- Hypoalbuminaemia (reduced synthesis + redistribution + capillary leak)
5. Systemic Consequences
SIRS (Systemic Inflammatory Response Syndrome)
When the local inflammatory cascade becomes systemic, it manifests as:
- Fever > 38°C or < 36°C
- Heart rate > 90 bpm
- Respiratory rate > 20/min or PaCO2 < 32 mmHg
- WBC > 12,000 or < 4,000 or > 10% bands
Immunological Changes
- Pro-inflammatory state initially (IL-1, IL-6, TNF-α)
- Counter-regulatory anti-inflammatory response syndrome (CARS) follows - mediated by IL-10, IL-4, IL-13, TGF-β
- Prolonged CARS leads to immune suppression, increased susceptibility to infection, and failure to resolve inflammation
Multi-Organ Dysfunction (MODS)
If SIRS is uncontrolled or prolonged:
- Acute kidney injury (AKI)
- Acute lung injury / ARDS
- Coagulopathy (endothelial DAMP activation)
- Hepatic dysfunction
- Within the brain: secondary brain injury
6. Nutritional Implications
The hypermetabolic, catabolic state drives significant nutritional requirements:
Energy:
- Gold standard measurement: indirect calorimetry (VO2 and VCO2, calculating respiratory quotient RQ = VCO2/VO2)
- Practical target: 25-30 kcal/kg/day
- Overfeeding is dangerous - excessive carbohydrate is converted to fat in the liver (hepatic steatosis); for every 3 O2 molecules inspired, 29 CO2 must be expired → hyperventilation and respiratory acidosis
Protein:
- Healthy adults: 0.8 g/kg/day RDA
- Critically ill/post-trauma: 1.2-2.0 g/kg/day
- Severely stressed patients: up to 2.5 g/kg/day
Enteral over parenteral nutrition is preferred to preserve gut mucosal integrity and reduce bacterial translocation.
7. Modifying the Metabolic Response
Modern surgical and critical care practices aimed at attenuating the metabolic response include:
- Enhanced recovery after surgery (ERAS) protocols - reducing perioperative starvation, multimodal analgesia, early mobilisation
- Regional anaesthesia - blocks the neuroendocrine afferent arc
- Tight glycaemic control (though the optimal target remains debated)
- Avoiding secondary triggers: prompt treatment of sepsis, bleeding, and ischaemia
- Nutritional support - both enteral and parenteral when required
- Pre-habilitation before elective surgery
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 24-26
- Fischer's Mastery of Surgery, 8th Edition, pp. 239-241
- Pye's Surgical Handicraft, 22nd Edition, p. 95
- Schwartz's Principles of Surgery, 11th Edition (Chapter: Systemic Response to Injury and Metabolic Support)
This is a shared conversation. Sign in to Orris to start your own chat.