Provide detail answer of emphysema mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and images needed. Let me compile the comprehensive MBBS-level answer on emphysema.
Emphysema - Comprehensive MBBS Notes
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
1. Definition
Emphysema is defined as permanent, irreversible enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls, but without significant fibrosis.
The key word is permanent - this distinguishes it from physiological overinflation. The absence of fibrosis distinguishes it from other parenchymal lung diseases.
2. Types / Classification
Emphysema is classified by its anatomic distribution within the acinus (the functional respiratory unit distal to the terminal bronchiole).
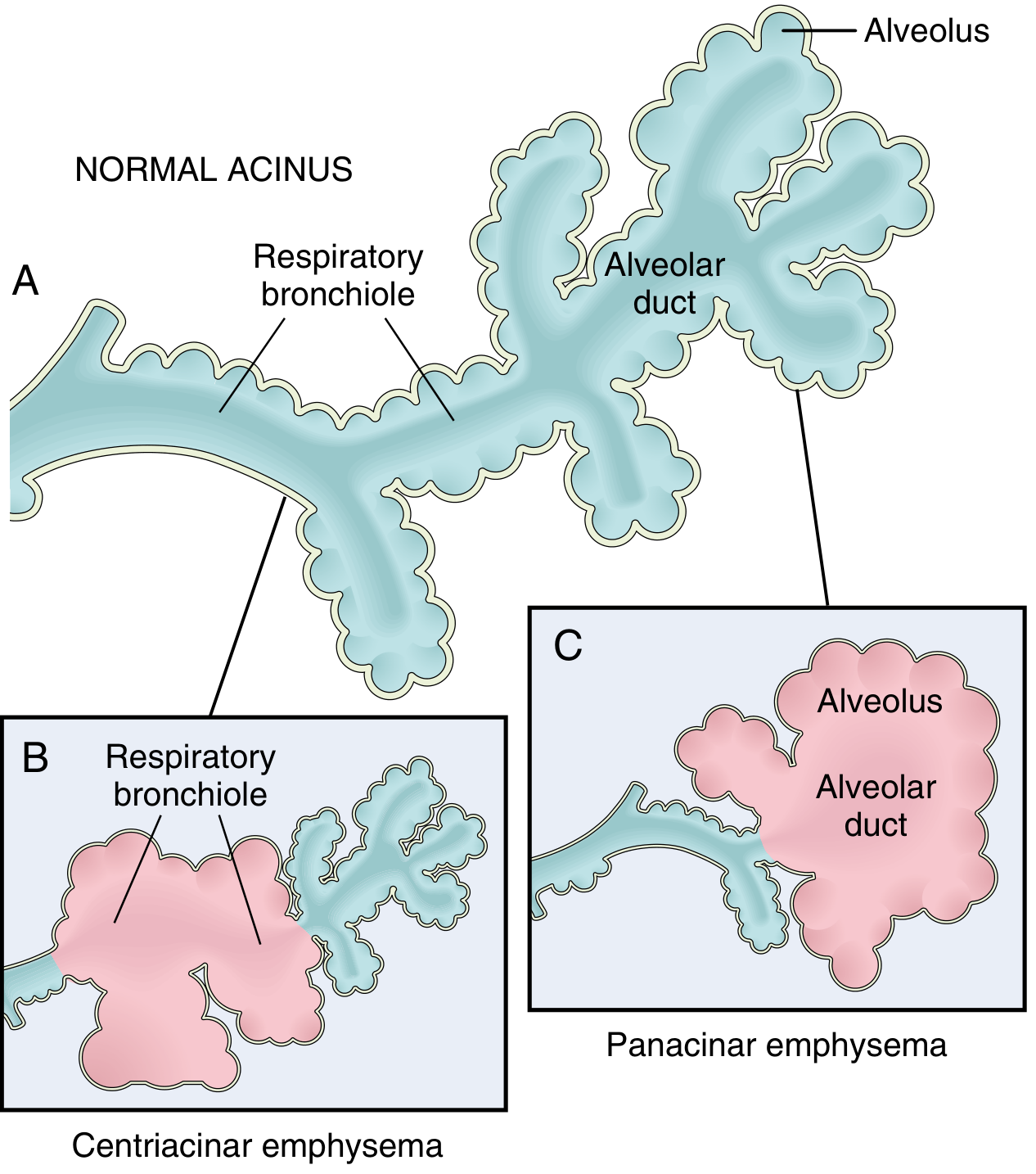
A. Centriacinar (Centrilobular) Emphysema - MOST COMMON
- Central / proximal parts of the acinus (respiratory bronchioles) are involved; distal alveoli are spared
- Both emphysematous and normal air spaces coexist in the same acinus and lobule
- More common and severe in the upper lobes, especially apical segments
- Constitutes >95% of clinically significant cases
- Strongly associated with cigarette smoking and often coexists with chronic bronchitis
- In advanced cases, distal acinus also involved (hard to distinguish from panacinar)
B. Panacinar (Panlobular) Emphysema
- The entire acinus is uniformly enlarged - from respiratory bronchioles all the way to terminal blind alveoli
- More common in lower lung zones and anterior margins; worst at the bases
- Associated with α1-antitrypsin deficiency (exacerbated by smoking)
- Produces pale, voluminous lungs that can obscure the heart at autopsy
C. Distal Acinar (Paraseptal) Emphysema
- Proximal acinus is normal, distal part is primarily involved
- Found near the pleura, along lobular connective tissue septa, and adjacent to areas of fibrosis/scarring
- Usually more severe in the upper half of lungs
- Multiple enlarged air spaces (0.5 mm to >2 cm), sometimes forming bullae
- Cause is unknown; classically presents as spontaneous pneumothorax in young adults
D. Irregular (Paracicatricial) Emphysema
- Acinus is irregularly involved
- Almost invariably associated with scarring (post-inflammatory or fibrotic)
- Usually clinically insignificant
Only types A and B cause clinically significant airflow obstruction and are associated with COPD.
3. Etiology / Risk Factors
| Factor | Details |
|---|---|
| Cigarette smoking | #1 cause; >40 pack-years typical; damages epithelium, promotes inflammation, impairs ciliary clearance |
| α1-antitrypsin deficiency | Genetic (autosomal recessive); Pi locus on chromosome 14; homozygous Z allele (ZZ) gives <15% normal serum levels; ~1% of all emphysema cases; causes panacinar emphysema |
| Air pollution | Sulfur dioxide, nitrogen dioxide, particulate matter |
| Occupational dust | Coal, silica, grain, cotton |
| Airway infection | Not initiating, but causes acute exacerbations |
4. Pathogenesis
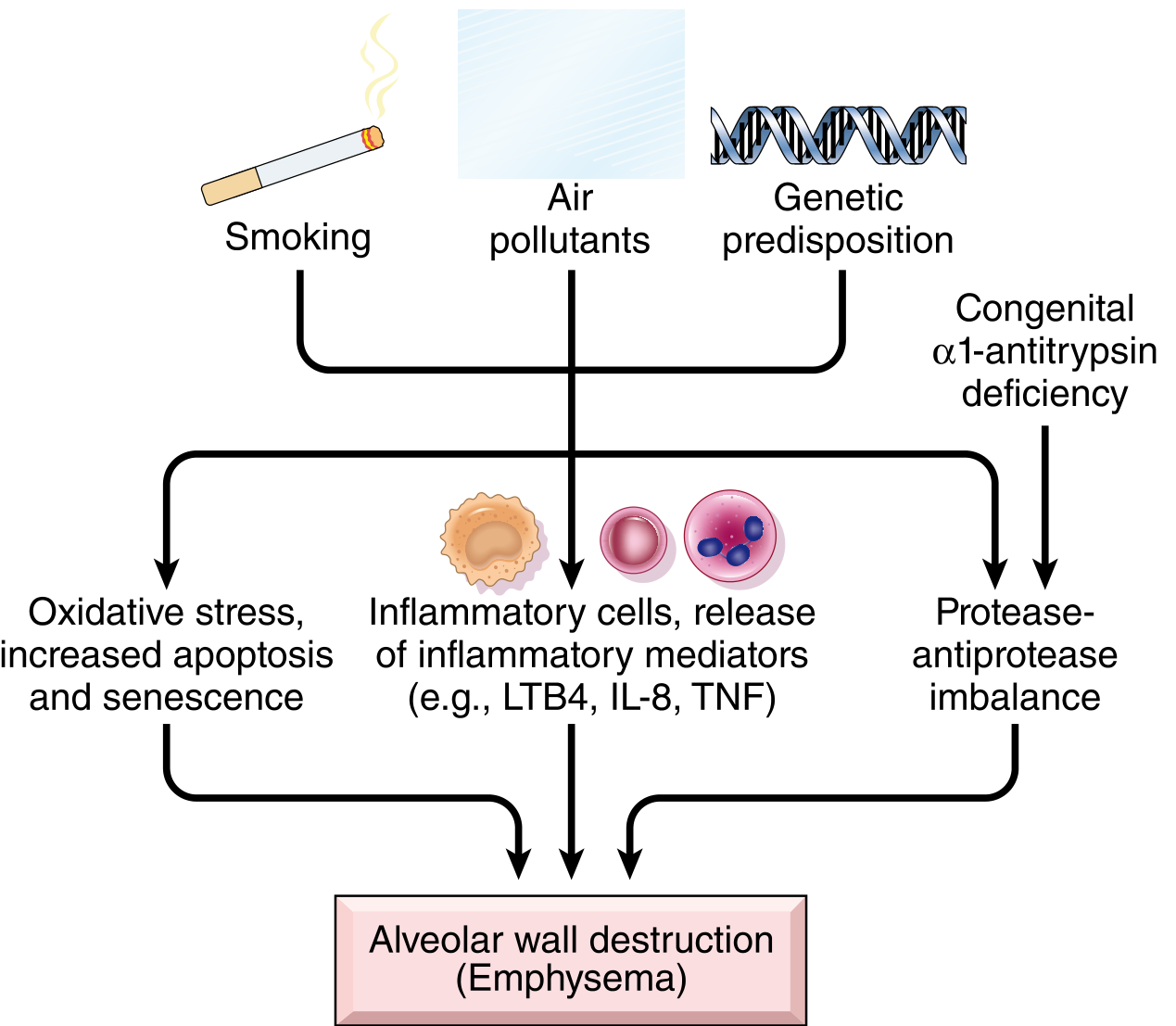
Key Mechanisms:
1. Protease-Antiprotease Imbalance (Central Mechanism)
- Inhaled toxins recruit neutrophils and macrophages into lung parenchyma
- These cells release proteases (especially elastase) that degrade connective tissue (elastin, collagen)
- Normally, α1-antitrypsin (α1-AT) inhibits elastase
- In smokers: cigarette smoke oxidizes and inactivates α1-AT; smoking also directly stimulates more protease release
- In α1-AT deficiency: constitutively reduced antiprotease activity - panacinar emphysema develops at an earlier age (30s-40s) and is more severe
- Result: unimpeded elastin degradation → loss of alveolar wall elastic recoil → air-space enlargement
2. Oxidative Stress
- Cigarette smoke contains reactive oxygen species (ROS)
- Inflammatory cells (macrophages, neutrophils) release additional ROS
- ROS cause direct tissue damage, endothelial dysfunction, and amplify inflammation
- ROS also inactivate antiproteases, compounding protease imbalance
- NRF2 (encoded by NFE2L2) is a key protective transcription factor against oxidant damage
3. Toxic Injury and Inflammation
- Noxious inhalants damage respiratory epithelium → chronic inflammation
- Inflammatory mediators: LTB4, IL-8, TNF-α attract more neutrophils/macrophages
- Accumulation of T and B lymphocytes in advanced disease
4. Loss of Elastic Recoil - Functional Consequence
- Small airways are normally held open by elastic recoil of surrounding parenchyma
- Destruction of elastic tissue in alveolar walls → loss of radial traction on respiratory bronchioles
- Respiratory bronchioles collapse during expiration (dynamic airway collapse) → functional air trapping even without mechanical obstruction
- This is the mechanism of obstructive ventilatory defect
5. Morphology
Gross Appearance:
- Panacinar: Pale, voluminous lungs; may obscure the heart when chest is opened at autopsy; uniformly enlarged air spaces
- Centriacinar: Lungs slightly deeper pink and less voluminous (until late stages); upper two-thirds more affected; focal emphysematous areas mixed with normal parenchyma
- Bullae: Large air-filled cysts >1 cm; seen especially in paraseptal emphysema; prone to rupture → pneumothorax
Histology:
- Destruction of alveolar walls without fibrosis
- Enlarged air spaces (fenestrations in walls)
- Loss of alveolar capillary bed → reduced diffusing capacity
- Fragmented elastic fibers (can be seen with elastic stains)
- Reduced number of alveolar walls per unit area
6. Clinical Features
"Pink Puffer" (Emphysema type)
| Feature | Description |
|---|---|
| Age | 50-75 years |
| Dyspnea | Early, severe, progressive |
| Cough | Late; scanty sputum |
| Appearance | Well-oxygenated (pink); thin/cachectic; barrel chest |
| Posture | Leaning forward, elbows on knees; pursed-lip breathing |
| Chest | Barrel chest (AP diameter increased), hyper-resonant, decreased breath sounds |
| Cyanosis | Absent or mild (maintains good oxygenation by hyperventilating) |
| Cor pulmonale | Uncommon until end-stage |
| Infections | Occasional |
| Blood gases | Relatively normal at rest; PaO2 maintained |
Barrel Chest Mechanism: Lung hyperinflation due to air trapping pushes the diaphragm down and increases AP diameter of thorax.
Pursed-lip Breathing Mechanism: Creates positive end-expiratory pressure (PEEP) in airways, preventing dynamic collapse of respiratory bronchioles during expiration.
Contrast with "Blue Bloater" (Chronic Bronchitis):
| Feature | Pink Puffer (Emphysema) | Blue Bloater (Chronic Bronchitis) |
|---|---|---|
| Age | 50-75 | 40-45 |
| Dyspnea | Early, severe | Mild, late |
| Cough | Late, scanty sputum | Early, copious sputum |
| Appearance | Pink, thin, barrel chest | Cyanotic, overweight |
| Infections | Occasional | Common |
| Cor pulmonale | End-stage only | Common |
| Airway resistance | Normal / slightly increased | Increased |
| Elastic recoil | Low | Normal |
| CXR | Hyperinflation, flat diaphragm, normal heart | Prominent vessels, large heart |
Most real patients fall somewhere in between with mixed bronchitic and emphysematous features.
7. Investigations
Pulmonary Function Tests (PFTs) - Most Important
- FEV1/FVC ratio < 0.7 - hallmark of obstructive ventilatory defect (GOLD criteria)
- FEV1 reduced (correlates with severity)
- TLC, RV, FRC all increased (air trapping, hyperinflation)
- DLCO (diffusing capacity) reduced - specific for emphysema (loss of alveolar surface area); helps distinguish emphysema from asthma
- Flow-volume loop: shows expiratory flow limitation, "scooped-out" appearance
Chest X-Ray
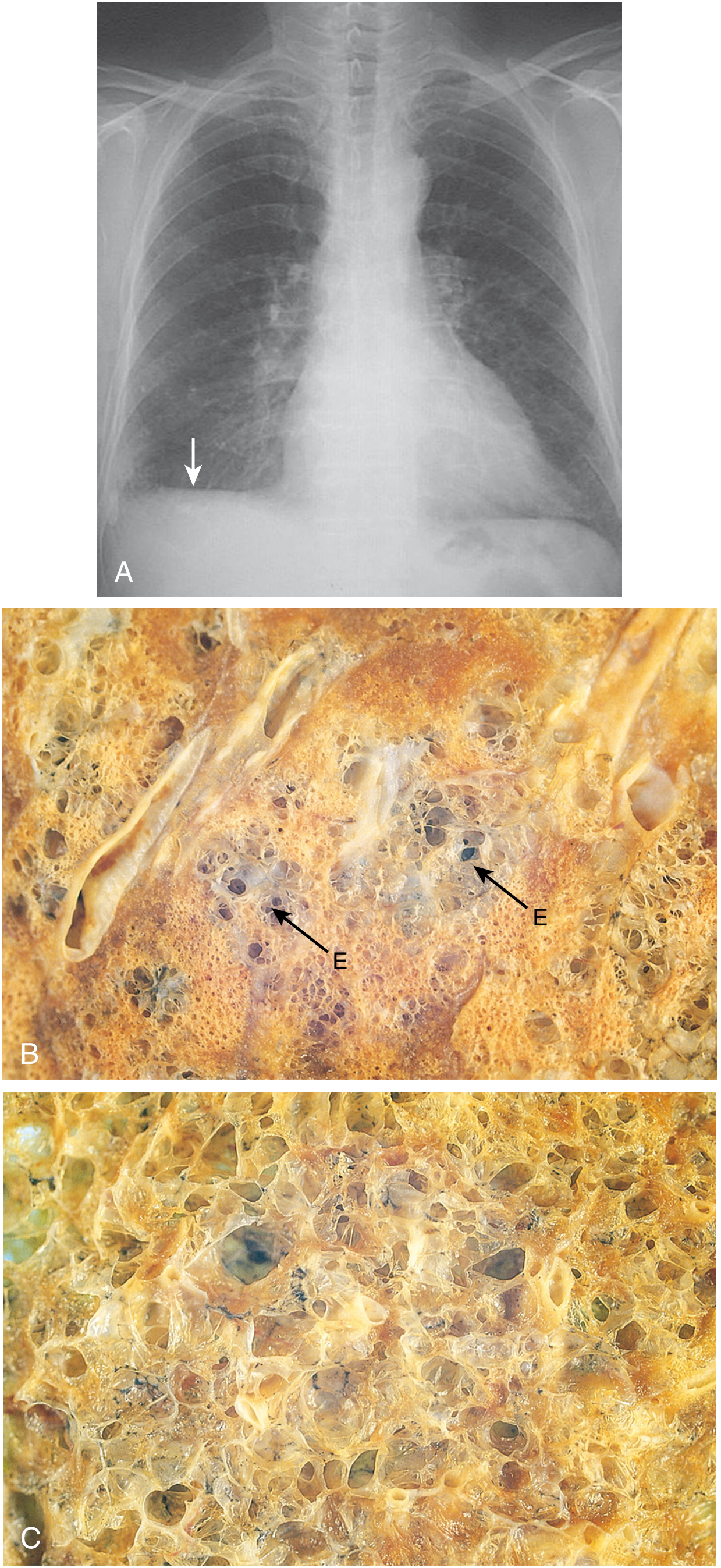
- Hyperinflated lungs - increased translucency
- Flattened diaphragm - most reliable sign (diaphragm level at or below 10th posterior rib)
- Increased AP diameter (barrel chest)
- Bullae - avascular hyperlucent areas
- Narrow mediastinum, elongated heart shadow
- Attenuated peripheral vascular markings ("pruning")
HRCT Chest
- Most sensitive method for diagnosing and quantifying emphysema
- Low-attenuation areas without visible walls
- Can differentiate centriacinar from panacinar patterns
- Centrilobular nodules in centriacinar type
Blood Gas Analysis (ABG)
- Maintained relatively normal until late stages in pure emphysema
- Eventually: hypoxemia (PaO2↓), hypercapnia (PaCO2↑)
Other Tests
- α1-antitrypsin serum levels (especially if age <45, non-smoker, panacinar pattern, family history)
- CBC: polycythemia secondary to chronic hypoxia (late)
- ECG: right axis deviation, P pulmonale (if cor pulmonale develops)
8. Treatment / Management
Non-Pharmacological
- Smoking cessation - single most effective intervention; slows FEV1 decline
- Pulmonary rehabilitation - improves exercise tolerance and quality of life
- Nutritional support - weight loss is common in emphysema
- Vaccination - influenza and pneumococcal vaccines to prevent exacerbations
Pharmacological
| Drug | Purpose |
|---|---|
| Long-acting bronchodilators (LABAs, LAMAs) | First-line; relieve bronchospasm, reduce hyperinflation |
| Inhaled corticosteroids (ICS) | Combined with LABAs in moderate-severe disease |
| Short-acting bronchodilators (SABA, SAMA) | Rescue therapy |
| Roflumilast (PDE-4 inhibitor) | For frequent exacerbators with chronic bronchitis component |
| Antibiotics | During infective exacerbations |
| Mucolytics (N-acetylcysteine) | May reduce exacerbations |
| α1-AT replacement therapy | Augmentation therapy for α1-AT deficiency |
Oxygen Therapy
- Long-term oxygen therapy (LTOT): indicated when PaO2 ≤55 mmHg (or ≤59 mmHg with cor pulmonale/polycythemia) at rest
- Recommended for ≥15-16 hours/day
- Reduces pulmonary hypertension and improves survival
Surgical Options
- Bullectomy - removal of large bullae compressing adjacent normal lung
- Lung Volume Reduction Surgery (LVRS) - resects severely emphysematous areas (upper lobe predominant); improves elastic recoil and diaphragm function
- Bronchoscopic lung volume reduction - endobronchial valves (less invasive)
- Lung transplantation - for end-stage disease in selected candidates
9. Complications
| Complication | Mechanism |
|---|---|
| Pulmonary hypertension | Hypoxic vasoconstriction + loss of capillary bed |
| Cor pulmonale | Right heart failure from pulmonary hypertension |
| Spontaneous pneumothorax | Rupture of subpleural bullae (especially paraseptal type) |
| Acute respiratory failure | Superimposed infection |
| Polycythemia | Secondary to chronic hypoxemia |
| Weight loss / cachexia | Increased work of breathing + systemic inflammation |
10. Key Concepts Summary
| Concept | Remember |
|---|---|
| Definition | Permanent air space enlargement + wall destruction, no fibrosis |
| Most common type | Centriacinar (>95% of clinical cases) |
| Most common cause | Cigarette smoking |
| Genetic cause | α1-antitrypsin deficiency (ZZ genotype) → Panacinar |
| Central mechanism | Protease-antiprotease imbalance (elastase > α1-AT) |
| Diagnostic test | Spirometry: FEV1/FVC <0.7 |
| DLCO | Reduced (distinguishes from asthma) |
| CXR sign | Flat diaphragm + hyperinflation |
| Clinical type | "Pink puffer" - dyspneic, barrel-chested, well-oxygenated |
| Spontaneous pneumothorax | Paraseptal/distal acinar emphysema |
| Best intervention | Smoking cessation |
References: Robbins & Kumar Basic Pathology (Robbins Pathology), Ch. 11 | Robbins, Cotran & Kumar Pathologic Basis of Disease, Ch. 15
This is a shared conversation. Sign in to Orris to start your own chat.