
In detail x ray
Reading File
analyse_media
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a detailed radiological analysis of this X-ray:
Radiological Report - Left Hip X-Ray
Patient: Hari Dwivedi | Age/Sex: 40 years / Male | Date: 28 June 2026
Views: AP (Anteroposterior) Pelvis + Left Hip Lateral
Institution: SP Diagnostic Center, Wagholi, Pune
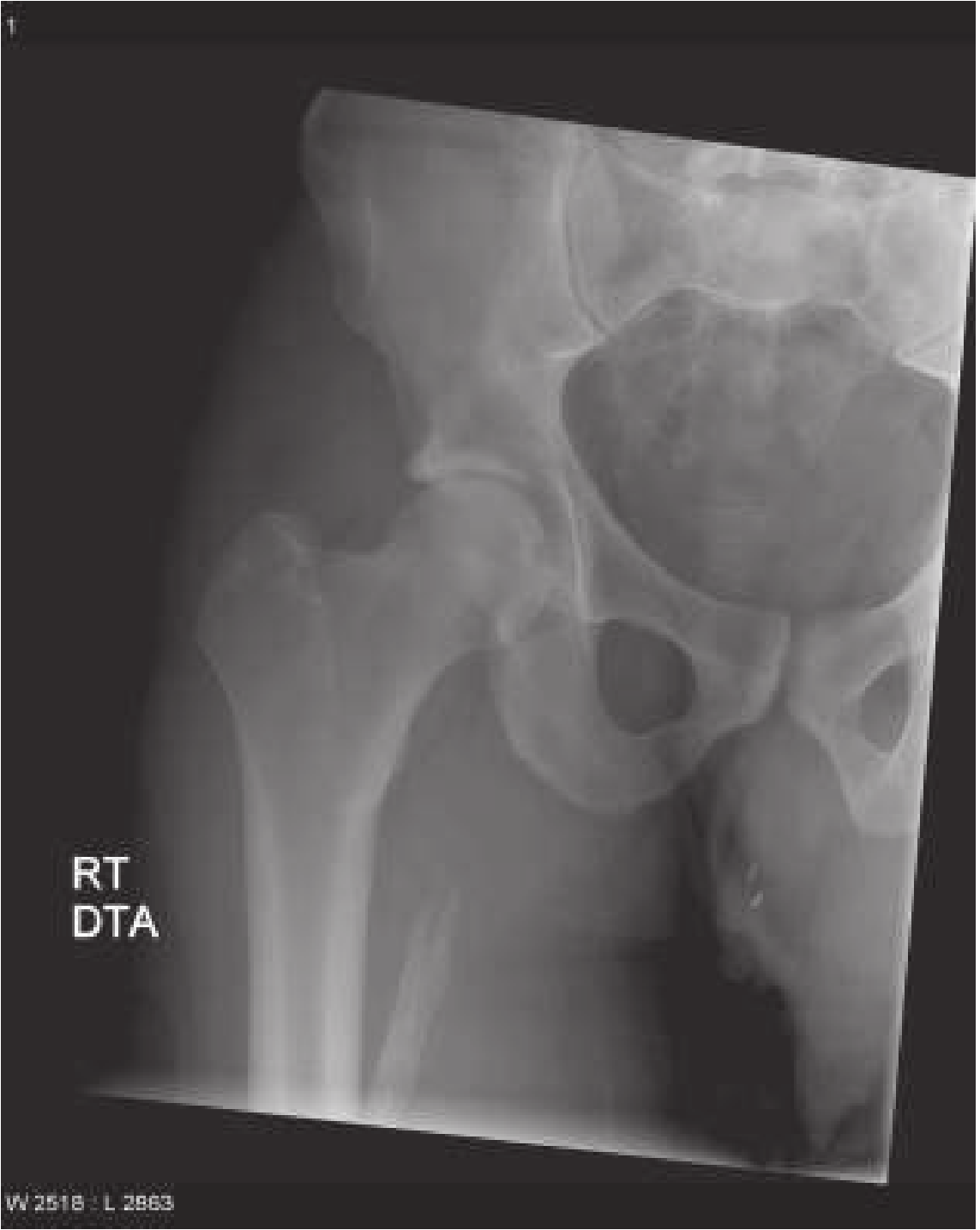
Primary Finding - Heterotopic Ossification / Myositis Ossificans
The most prominent and diagnostically significant finding is a large, well-circumscribed, oval-to-lobulated calcified soft tissue mass at the medial and posterior aspect of the proximal left femoral shaft, just distal to the lesser trochanter.
Characteristics of the Mass:
| Feature | Description |
|---|---|
| Location | Medial/posterior proximal femur, distal to lesser trochanter |
| Size | Large - approximately 5-7 cm estimated |
| Margins | Well-defined, with a thick, mature peripheral sclerotic/ossified rim ("eggshell calcification") |
| Internal pattern | Reticular, trabecular, septated calcifications with central lucency |
| Cortical relationship | Adjacent to but no aggressive cortical destruction of the femur; cortex intact |
| Periosteal reaction | Absent (no aggressive periosteal response) |
| Zonal pattern | Peripheral ossification > central lucency - classic "zonal phenomenon" |
This pattern - peripheral calcification with central lucency - is the classic radiographic hallmark of mature myositis ossificans (heterotopic ossification). As described in Rosen's Emergency Medicine:
"Radiographically, myositis ossificans appears as irregularly shaped masses of heterogeneous bone in the soft tissues... It can be seen as early as 10-21 days after injury... CT can be helpful in distinguishing between neoplasm and myositis ossificans, because lesions of myositis ossificans begin to calcify at the periphery and progress toward the center."
- Rosen's Emergency Medicine, p. 689
And from Miller's Review of Orthopaedics:
"Radiographs show peripheral mineralization with a central lucent area as maturation progresses. The lesion is not attached to the underlying bone, but in some cases it may become fixed to the periosteal surface."
The mass in this patient shows mature/late-stage heterotopic ossification, given the well-organized, thick peripheral bone shell visible on both views.
Left Hip Joint Assessment
- Joint space: Well-preserved and symmetric - no joint space narrowing
- Femoral head: Normally shaped, no avascular necrosis, no subcortical collapse or sclerosis
- Acetabulum: Smooth margins, intact roof, no dysplasia or protrusio
- No osteophytes or subchondral cysts - no features of osteoarthritis
- Femoral neck: Normal neck-shaft angle (approximately 125-130°), no coxa vara or valga
- Greater and lesser trochanters: Intact, no avulsion fractures
Right Hip (Contralateral - Seen on AP View)
- Normal hip joint space
- No obvious pathology on this limited view
- Provided for comparison only
Pelvis Assessment
- Pelvis appears symmetric without obvious tilt or obliquity
- Sacroiliac joints appear normal
- No pelvic ring fractures
- Pubic symphysis appears intact
Differential Diagnosis for the Soft Tissue Calcification
| Diagnosis | Likelihood | Key Features |
|---|---|---|
| Myositis ossificans (heterotopic ossification) | Most likely | Peripheral calcification, zonal pattern, no cortical destruction, history of trauma |
| Parosteal osteosarcoma | Must exclude | Centrally calcified, cortical attachment, aggressive; absent here |
| Osteochondroma | Less likely | Typically arises from cortex with medullary continuity; no such continuity seen |
| Calcific bursitis | Less likely | Usually amorphous, poorly marginated, trochanteric location |
| Soft tissue sarcoma with calcification | Must exclude | Cortical destruction, aggressive margins; absent here |
The key differentiating point from malignancy (especially osteosarcoma) is the peripheral-to-central calcification pattern (zonal phenomenon). In osteosarcoma, calcification begins centrally. This mass shows the opposite, strongly favoring a benign process.
Impression
- Large mature myositis ossificans (heterotopic ossification) of the proximal left femoral soft tissues, most likely post-traumatic in etiology. The lesion appears mature based on the well-organized peripheral ossified shell.
- Left hip joint is preserved - no osteoarthritis, avascular necrosis, or fracture.
- No aggressive periosteal reaction or cortical destruction.
Recommended Next Steps
- Clinical correlation: Confirm history of prior trauma, repeated injury, or prior hip surgery (incidence of HO after hip surgery ~2%)
- MRI left hip: To better characterize the mass, assess medullary involvement, and exclude soft tissue malignancy if clinically warranted
- CT scan: Can confirm the classic peripheral-to-central calcification pattern ("zoning phenomenon") and definitively exclude attachment to cortex
- Orthopedic review: If the mass causes pain or limits range of motion, surgical excision may be considered - but only after the lesion has fully matured (typically 6-18 months after injury onset, confirmed by isotope bone scan showing quiescent activity)
- Bone scan (Tc-99m): Useful to confirm maturity of the lesion before any planned surgery
Note: This analysis is for informational/educational purposes. A formal radiological report from a qualified radiologist reviewing the original DICOM images is required for clinical decision-making.
Here is the textbook reference image of a similar case of mature myositis ossificans of the proximal femur for comparison:
Physiotherapy role in this
Finding Sources
Finding Sources
Searching PubMed
myositis ossificans physiotherapy rehabilitation
Finding Sources
Finding Sources
Searching PubMed
heterotopic ossification physical therapy exercise rehabilitation hip
Finding Sources
Reading Article
Finding Sources
Finding Sources
Searching the Web
physiotherapy myositis ossificans heterotopic ossification hip management guidelines 2023 2024
Reading Web Page
physiotherapy physical therapy exercise ROM myositis ossificans heterotopic ossification management
Here is a detailed breakdown of the physiotherapy role for this patient (40-year-old male with mature myositis ossificans / heterotopic ossification at the proximal left femur):
Physiotherapy in Myositis Ossificans - Proximal Left Femur
Phase 1: Acute / Active Inflammatory Stage
Goal: Protect, control pain and swelling, prevent joint stiffness
This phase applies if the lesion is still active (warm, swollen, tender). Based on the X-ray, the lesion appears mature, so this phase may already be past - but it is included for completeness.
Do's:
- Rest the hip in a functional position - hip in slight flexion/abduction with neutral rotation (use positioning aids)
- RICE: Rest, Ice (15-20 min, 3-4x/day), Compression, Elevation where possible
- Gentle passive range of motion (PROM) - initiated as early as possible, within pain-free range, to prevent ankylosis
- Isometric exercises for quadriceps and gluteals to maintain muscle tone without stressing the lesion
- Electrotherapy - TENS for pain control (safe at this stage)
Absolute Contraindications in active stage:
| Contraindicated Intervention | Reason |
|---|---|
| Deep tissue massage over lesion | Stimulates further heterotopic bone formation |
| Aggressive stretching | Creates microtrauma, worsens ossification |
| Heat therapy (ultrasound, hot packs) to lesion | Increases local circulation, promotes bone growth |
| Forceful joint manipulation | Risk of new hematoma formation and fracture |
"Resting the joint appears more likely to lead to decreased ROM or ankylosis." - Medscape / AAPMR KnowledgeNow (2024)
Phase 2: Subacute / Maturing Stage
Goal: Restore ROM, maintain muscle strength, prevent contracture
Timing: When acute inflammatory signs (warmth, redness, swelling) have subsided. Alkaline phosphatase levels normalize and X-ray shows organized peripheral calcification (as seen in this patient).
Key Physiotherapy Interventions:
1. Range of Motion Exercises
- Passive ROM (PROM): Gentle, slow, sustained stretches within comfortable range
- Active-Assisted ROM (AAROM): Patient participates with therapist assistance
- Active ROM (AROM): Independent movement through full range
- Focus on: Hip flexion, extension, abduction, adduction, internal and external rotation
- Progress gradually - avoid pain during exercise
- The consensus is that PROM and continued mobilization, once acute inflammation has subsided, are indicated to maintain ROM (Medscape HO Management, 2024)
2. Strengthening Programme
- Isometric → isotonic progression
- Hip flexors (iliopsoas), extensors (gluteus maximus), abductors (gluteus medius), quadriceps, hamstrings
- Aquatic exercises: excellent option - buoyancy reduces load, allows greater ROM with less pain
- Closed kinetic chain exercises when tolerating weight-bearing
3. Soft Tissue Work (Carefully)
- Massage to surrounding musculature (NOT directly over the calcified mass)
- Myofascial release to hip flexors, adductors, TFL if shortened
- Scar tissue / fascial mobilization around the lesion margins
4. Gait Rehabilitation
- Assess and correct any antalgic gait pattern
- Correct Trendelenburg if gluteus medius is weak
- Progress from walking aids to independent ambulation
- Stair training and functional task retraining
5. Electrotherapy Modalities
| Modality | Use | Notes |
|---|---|---|
| TENS | Pain relief | Safe over/around lesion |
| Ultrasound | NOT over calcified lesion | Contraindicated directly over bone |
| Laser therapy | May help pain and inflammation | Low-level laser to surrounding tissue |
| Extracorporeal Shock Wave Therapy (ESWT) | Emerging evidence for HO | May help with pain and lesion breakdown in mature stage |
| IFT / NMES | Muscle re-education | Around the lesion, not directly on it |
Phase 3: Mature Stage (Current Stage - Based on X-Ray)
Goal: Maximize function, maintain ROM, prevent recurrence, return to activity
The X-ray confirms a mature, well-organized lesion with thick peripheral ossification. At this stage the lesion is stable.
Physiotherapy Focus:
1. Progressive Strengthening
- Resistance training: Hip abductors, extensors, flexors
- Functional strengthening: Squats, lunges, step-ups (pain-guided)
- Core stability: Transversus abdominis, multifidus activation
- Proprioceptive training: Single-leg balance, unstable surface training
2. Flexibility & ROM Maintenance
- Daily sustained stretching of hip flexors, adductors, IT band
- Yoga / Pilates-based movements for hip mobility
- Hydrotherapy / aquatic therapy remains excellent at this stage
3. Functional Rehabilitation
- ADL training - sitting, rising from floor, climbing stairs
- Return to work / sport-specific training if applicable
- Ergonomic advice for occupation
4. Patient Education (Critical)
- Explain the nature of the lesion - it is benign and stable
- Teach self-ROM exercises for home program
- Warn about avoiding re-trauma to the area
- Signs of reactivation to watch for (new warmth, swelling, pain)
- Importance of regular follow-up
Pre-Surgical Physiotherapy (If Surgery is Planned)
If pain or ROM restriction is functionally limiting and surgical excision is being considered:
- Optimize pre-operative strength and ROM as much as possible
- Prehabilitation - respiratory exercises, cardiovascular fitness
- Confirm maturity of lesion before surgery (bone scan showing "cold" uptake)
- Typically surgery is deferred until 6-18 months after initial injury or until mature
Post-Surgical Physiotherapy (After Surgical Excision):
- Gentle PROM started 72 hours post-operation
- Progressive intensity over weeks
- Retraining in functional activities - transfers, walking, stairs
- NSAIDs (indomethacin) or low-dose radiation may be given post-surgically to prevent recurrence - physiotherapy complements this
- Full return to function over 3-6 months
Summary - Physiotherapy Goals by Phase
| Phase | Key Goal | Primary Intervention |
|---|---|---|
| Acute (active) | Protect, reduce pain | Rest + position, gentle PROM, TENS |
| Subacute (maturing) | Restore ROM, prevent contracture | Graded PROM → AROM, strengthening |
| Mature (current) | Maximize function | Progressive strengthening, flexibility, ADL rehab |
| Pre-surgical | Optimize pre-op fitness | Prehabilitation |
| Post-surgical | Restore full function | PROM at 72h, graded return |
Critical Points for This Patient (40-year-old male, mature lesion)
- Do not apply deep heat or ultrasound directly over the calcified mass - this remains contraindicated even in the mature stage
- Deep tissue massage directly on the ossified area is contraindicated
- The left hip joint space is preserved - this is favorable, meaning full functional recovery is achievable
- Regular reassessment of hip ROM is needed to detect any progressive restriction
- If the lesion causes no functional limitation, observation with a home exercise program is sufficient
- Coordinate with the orthopedic surgeon and physiatrist - physiotherapy is part of a multi-disciplinary team approach
This is a shared conversation. Sign in to Orris to start your own chat.