Definition of varicose veins
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a well-sourced definition of varicose veins drawn from multiple authoritative surgical and pathology textbooks:
Varicose Veins - Definition
Varicose veins are abnormally dilated, tortuous veins produced by prolonged, increased intraluminal pressure, resulting in vessel wall dilation and subsequent incompetence of the venous valves.
- Robbins, Cotran & Kumar: Pathologic Basis of Disease
The findings may include dilated and tortuous veins, telangiectasias, and fine reticular varicosities.
- Schwartz's Principles of Surgery, 11th Edition
Key Pathophysiology
- Increased venous pressure leads to progressive dilation of the vein wall
- Valve cusps become separated and incompetent, allowing retrograde (reflux) blood flow
- This creates a self-perpetuating cycle of further pressure elevation and dilation
- The superficial veins of the lower leg are most commonly affected because venous pressure at these sites can be elevated up to 10 times normal with prolonged dependent posture
Classification
| Type | Mechanism |
|---|---|
| Primary | Intrinsic abnormality of the venous wall itself |
| Secondary | Associated with deep and/or superficial venous insufficiency (e.g. DVT, post-thrombotic syndrome) |
Epidemiology
- Present in at least 10% of the general population (Schwartz's)
- Up to 20% of males and one-third of females develop lower extremity varicosities (Robbins)
- Risk factors: obesity, female sex, prolonged standing, pregnancy (compression of IVC by gravid uterus), family history, and inactivity
Sites Commonly Affected
- Lower limb superficial veins (great saphenous vein and small saphenous vein tributaries) - most common
- Esophageal varices - due to portal hypertension from liver cirrhosis
- Hemorrhoids - varicose dilation of the anorectal venous plexus
Clinical Consequences
Incompetent venous valves lead to stasis, congestion, edema, pain, and thrombosis. Chronic venous congestion causes secondary tissue ischemia, resulting in:
- Stasis dermatitis ("brawny induration")
- Skin hyperpigmentation and lipodermatosclerosis
- Venous ulceration
- (Note: embolism from superficial varicose veins is very rare, unlike DVT)
Sources:
- Robbins, Cotran & Kumar: Pathologic Basis of Disease - Varicose Veins, Vascular Pathology chapter
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Chapter 62
- Schwartz's Principles of Surgery, 11th Ed. - Vascular Surgery section
Thread and reticular veins
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, textbook-sourced breakdown of thread veins and reticular veins, placed in context alongside the full spectrum of superficial venous disease:
Thread Veins (Telangiectasias)
Thread veins - also called spider veins, hyphen webs, or telangiectasias - are tiny intradermal venules less than 1 mm in diameter. They appear as fine red, purple, or dark-blue lines or web-like patterns visible at the skin surface.
-
Histologically, they are dilated blood channels in normal dermal stroma with a single endothelial cell lining, limited muscularis, and adventitial layers. Most measure 26 to 235 µm in diameter and lie 175 to 382 µm below the stratum granulosum.
-
They are classified as CEAP class C1 disease (the lowest clinical class of visible venous abnormality).
-
Most telangiectasias arise from - and are fed by - underlying reticular veins. Treating the feeding reticular vein first is the key principle of management.
-
Bailey and Love's Short Practice of Surgery, 28th Ed.; Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.
Reticular Veins
Reticular veins are small, dilated, bluish subdermal veins measuring 1-2.9 mm in diameter, usually tortuous in course. They lie deeper than telangiectasias (subdermally rather than intradermally), which is why they appear blue-green rather than red.
-
They can be difficult to distinguish from a normal subdermal vein in someone with thin, pale, transparent skin.
-
They are best visualised with the patient lying prone or supine (unlike varicose veins, which are best seen standing). Transillumination helps detail their relationship to overlying telangiectasias.
-
They often act as the feeding source for overlying thread veins/telangiectasias.
-
Bailey and Love's Short Practice of Surgery, 28th Ed.; Fitzpatrick's Dermatology
Comparison Table
| Feature | Thread Veins (Telangiectasias) | Reticular Veins | Varicose Veins |
|---|---|---|---|
| Diameter | < 1 mm | 1-2.9 mm | ≥ 3 mm |
| Location | Intradermal | Subdermal | Subcutaneous |
| Colour | Red / dark purple | Blue / blue-green | Skin-coloured / blue |
| Appearance | Fine web or lines | Tortuous, flat | Bulging, tortuous |
| CEAP class | C1 | C1 | C2 |
| Best viewed | Standing | Prone / supine | Standing |
| Symptoms | Usually none | Usually none | Aching, heaviness |
Clinical Significance
Telangiectasias and reticular veins occur very commonly in the absence of significant reflux or obstruction and in the vast majority do not cause physical symptoms, though cosmetic treatment is commonly sought. Treatment is considered elective and is usually not covered by standard insurance. Up to 50% of patients do report some symptoms, however - ranging from dull aching to throbbing pain over affected areas.
The cutaneous manifestations of venous hypertension (of which these form part) include:
-
Telangiectasias
-
Reticular veins
-
Corona phlebectatica (malleolar flare) - a fan-shaped telangiectatic pattern at the ankle, signalling advanced venous disease
-
Current Surgical Therapy, 14th Ed.; Bailey and Love's, 28th Ed.
Clinical Photo
The image below (from Bailey and Love's) shows telangiectasias (fine red thread veins) alongside larger reticular veins (bluish, slightly larger tortuous vessels) on the leg:
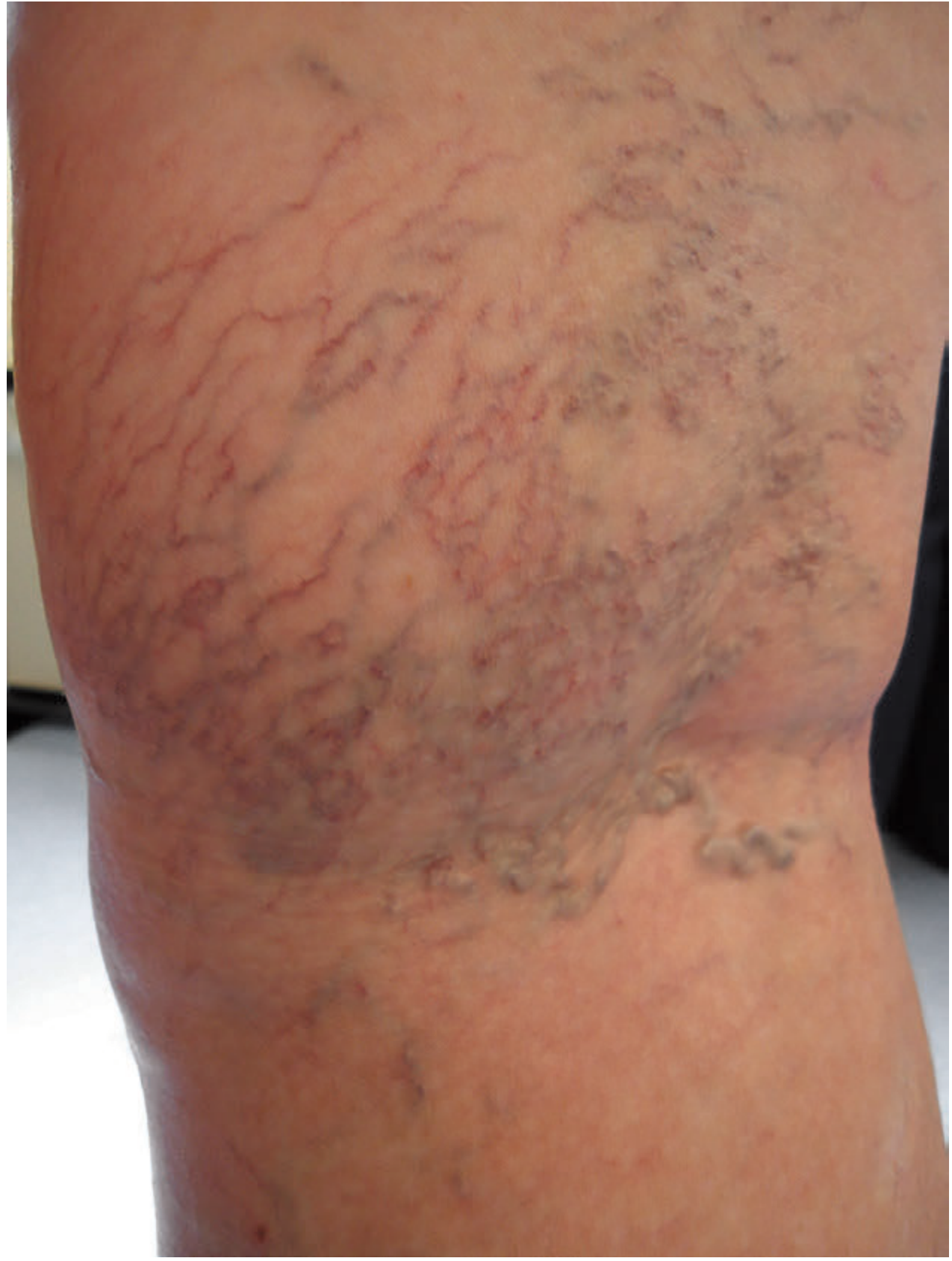
Figure 62.4 - Telangiectasia and reticular veins. Bailey and Love's Short Practice of Surgery, 28th Ed.
CEAP classification
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is the full CEAP classification, compiled from multiple surgical textbooks with the 2020 updates included:
CEAP Classification of Chronic Venous Disorders
The CEAP system was devised in 1994 by the American Venous Forum (AVF) and has since become the international standard for classifying chronic venous disease (CVD). It was last updated in 2020, which added corona phlebectatica as C4c, introduced the "r" modifier for recurrent disease, and replaced numeric venous segment descriptions with standard abbreviations.
- Sabiston Textbook of Surgery; Fischer's Mastery of Surgery, 8th Ed.
C - Clinical Classification
| Class | Description |
|---|---|
| C0 | No visible or palpable signs of venous disease |
| C1 | Telangiectasias or reticular veins |
| C2 | Varicose veins |
| C2r | Recurrent varicose veins (added 2020) |
| C3 | Edema |
| C4 | Changes in skin and subcutaneous tissue secondary to CVD |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C4c | Corona phlebectatica (added 2020) |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
| C6r | Recurrent active venous ulcer (added 2020) |
Each class is further qualified as:
- S = Symptomatic (aching, pain, tightness, skin irritation, heaviness, muscle cramps)
- A = Asymptomatic
e.g., a patient with an active venous ulcer with symptoms is classified as C6,S
E - Etiologic Classification
| Code | Meaning |
|---|---|
| Ec | Congenital - present since birth |
| Ep | Primary - no identifiable cause; intrinsic vein wall/valve defect |
| Es | Secondary - has an identifiable cause (post-thrombotic, post-traumatic) |
| Es(i) | Secondary - intravenous cause |
| Es(e) | Secondary - extravenous cause |
| En | No venous etiology identified |
A - Anatomic Classification
| Code | Meaning |
|---|---|
| As | Superficial veins |
| Ap | Perforator veins |
| Ad | Deep veins |
| An | No venous anatomic location identified |
These can be combined (e.g., As,p = superficial and perforator involvement).
P - Pathophysiologic Classification
| Code | Meaning |
|---|---|
| Pr | Reflux |
| Po | Obstruction |
| Pr,o | Reflux and obstruction |
| Pn | No pathophysiology identified |
How CEAP Is Written in Practice
A complete CEAP descriptor combines all four components, for example:
C3,S, Ep, As, Pr = Symptomatic edema, primary etiology, superficial vein involvement, due to reflux
C6,S, Es, Ad, Po = Active venous ulcer with symptoms, secondary etiology (e.g. post-DVT), deep vein involvement, due to obstruction
Supplementary Scoring Tools
Because CEAP alone cannot track treatment outcomes, two additional scoring systems are used alongside it:
| Tool | Purpose |
|---|---|
| Venous Clinical Severity Score (VCSS) | Current standard for clinical outcome assessment after intervention; validated patient-reported outcomes |
| Venous Segmental Disease Score (VSDS) | Quantifies extent of venous segment disease |
Together, CEAP + VCSS + VSDS provide researchers and clinicians with a complete framework for both classification and outcome monitoring.
- Sabiston Textbook of Surgery, 21st Ed.; Fischer's Mastery of Surgery, 8th Ed.; Harrison's Principles of Internal Medicine, 22nd Ed.
What is White cell trap theory in varicose veins
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Here is a thorough, textbook-sourced explanation of the White Cell Trapping Theory, placed in full context alongside the other theories of venous ulceration:
Pathophysiology of Venous Ulceration - The Competing Theories
The exact mechanism by which chronic venous hypertension leads to skin damage and ulceration has been debated for decades. Several theories have been proposed, each building on observations that challenged the previous one.
1. Stasis / Hypoxia Theory (Original - now disproved)
The earliest hypothesis held that static blood in the superficial veins led to local hypoxia and tissue death - hence the term "stasis ulcer." This was refuted when investigation of venous oxygen saturation showed it was actually higher in ulcerated limbs (arterialised venous blood), ruling out simple stasis as the mechanism.
2. Arteriovenous Fistula Theory (Disproved)
The elevated venous oxygen saturation prompted the hypothesis that arteriovenous fistulae were developing in response to high venous pressure, shunting oxygenated arterial blood into the venous system. This also could not be confirmed anatomically.
3. Fibrin Cuff Theory (Browse & Burnand, 1982)
This was a major step forward. The observation was that high venous pressure causes fibrinogen to leak out of damaged capillary endothelial cells, where it polymerises to form pericapillary fibrin deposits - so-called "fibrin cuffs."
Mechanism:
-
Venous hypertension → increased capillary pressure → endothelial damage → fibrinogen extravasation
-
Fibrinogen polymerises around capillaries forming thick fibrin cuffs
-
These cuffs act as a barrier to diffusion of oxygen and nutrients into the surrounding tissue
-
Result: local ischaemia, tissue necrosis, fibrosis, and ulceration
-
Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.
4. White Cell Trapping Theory (the "Leukocyte Trapping" Theory)
This theory emerged from the observation that leukocytes were reduced in venous blood returning from legs with venous hypertension - implying they were being retained (trapped) in the microcirculation.
Mechanism, step by step:
- Venous hypertension slows capillary blood flow in the lower limb
- Sluggish flow causes leukocytes (white blood cells) to marginate and adhere to capillary endothelium - a process normally reserved for acute inflammation
- The adherent leukocytes physically obstruct the local capillaries, further impairing microcirculation
- Trapped leukocytes become activated and migrate into the surrounding subcutaneous tissue
- Activated leukocytes release:
- Proteolytic enzymes (matrix metalloproteinases) - causing direct tissue destruction
- Toxic metabolites and reactive oxygen species (free radicals) - causing oxidative tissue damage
- This increases capillary permeability, worsening oedema and further perpetuating the cycle
- End result: local ischaemia, tissue necrosis, and ulceration
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.; Bailey and Love's Short Practice of Surgery, 28th Ed.
Current Status of the Theory
The white cell trapping theory has not been fully confirmed by subsequent investigation:
-
Polymorphonuclear leukocytes (neutrophils) were NOT consistently found within the peri-ulcer tissues
-
Instead, increased numbers of mast cells, monocytes, and lymphocytes were found in periulcer tissues
-
The concept remains relevant but has been modified rather than accepted wholesale
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
5. Trap Hypothesis (Unifying Theory)
This synthesises the above theories and adds an important further observation:
-
Venous hypertension causes extravasation of red blood cells from the capillary bed in addition to fibrin and leukocytes
-
These "trapped" red blood cells break down in the tissues and release haemoglobin, which is metabolised to haemosiderin
-
Haemosiderin is responsible for the characteristic brown hyperpigmentation ("brawny oedema") of advanced CVI
-
The fibrin cuffs and resultant fibrosis produce the thin, glistening, indurated skin of lipodermatosclerosis
-
These ischaemic, fibrotic areas develop stasis dermatitis with intense pruritus → scratching → skin breakdown → ulceration
-
Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.
Additional Factors Now Recognised
| Factor | Role |
|---|---|
| Reactive oxygen species | Increased in the ulcer environment; generate free radicals causing tissue damage |
| Proteolytic enzymes (MMPs) | Elevated in ulcers; degrade extracellular matrix |
| Senescent fibroblasts | Fibroblasts in peri-ulcer tissue are in a "senescent" state - unable to respond normally to repair signals |
| Growth factor inhibition | Sequestration of growth factors by fibrin cuffs impairs healing |
The Accepted Bottom Line
Ambulatory venous hypertension is the only universally accepted underlying cause of venous ulceration. This also explains why venous ulcers are never seen in the upper limb (where venous pressures are not comparably elevated by gravity and standing).
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Origin and coarse of long saphenous vein and Short saphenous vein
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a full anatomical account of both saphenous veins, drawn directly from Bailey and Love's Short Practice of Surgery, 28th Edition:
Anatomy of the Superficial Venous System
Both saphenous veins lie superficial to the fascia lata (deep fascia) but deep to the saphenous fascia, travelling in a fascial "envelope" - the saphenous compartment. This is clinically important because it keeps them distinct from the subcutaneous fat and makes them identifiable on duplex ultrasound.
Great Saphenous Vein (GSV) - Long Saphenous Vein
Origin
- Arises from the medial end of the dorsal venous arch of the foot
- The dorsal arch runs in the subcutaneous tissues over the metatarsal heads (the plantar surface drains preferentially dorsally to avoid pressure damage)
Course
- Passes anterior to the medial malleolus at the ankle
- Ascends the medial aspect of the leg, lying in the superficial tissues medial to the tibia, accompanied by the saphenous nerve
- Loops posteriorly at the level of the medial condyle of the femur
- Continues up the medial thigh
- In the groin, unites with several tributaries corresponding to branches of the common femoral artery
- Pierces the cribriform fascia covering the saphenous opening (fossa ovalis), located approximately 2.5 cm below and lateral to the pubic tubercle
- Terminates by draining into the common femoral vein (CFV) at the saphenofemoral junction (SFJ)
Key Facts
- The longest vein in the body
- Most frequently affected superficial vein in varicose disease (involved in ~60% of cases)
- Throughout its course it receives variable superficial tributaries
Important Tributary - Anterior Accessory GSV (AAGSV)
- One of the most common tributaries
- Commonly originates around the lateral border of the knee (sometimes as low as the lateral end of the dorsal arch)
- May course up the medial thigh anterolateral to the GSV, and drain into the GSV at or near the SFJ
- Frequently mistaken for the GSV itself (called a "duplex GSV" by some surgeons; a true duplex GSV is rare)
Small Saphenous Vein (SSV) - Short Saphenous Vein
Origin
- Arises from the lateral end of the dorsal venous arch of the foot
Course
- Passes posterior to the lateral malleolus
- Ascends the posterior midline of the leg, accompanied by the sural nerve
- In the proximal calf sits in the groove between the two heads of gastrocnemius
- Pierces the fascia of the popliteal fossa and typically terminates by draining into the popliteal vein at the saphenopopliteal junction (SPJ)
Termination - Highly Variable
The SPJ is notably variable in its position:
| Variant | Description |
|---|---|
| Typical | Terminates in the popliteal vein at the popliteal fossa |
| Low termination | Junction may occur as low as the mid-calf |
| Cranial extension | SSV continues beyond the SPJ into the posterior thigh, terminating by piercing the deep fascia to drain into the deep system |
| Giacomini vein | A cranial extension that communicates with the GSV system, occasionally joining the GSV at or near the SFJ |
| No popliteal termination | In some cases the SSV continues entirely as a cranial extension or Giacomini vein without any popliteal termination |
Comparison Summary
| Feature | Great Saphenous Vein (GSV) | Small Saphenous Vein (SSV) |
|---|---|---|
| Origin | Medial end of dorsal venous arch | Lateral end of dorsal venous arch |
| Ankle relation | Anterior to medial malleolus | Posterior to lateral malleolus |
| Course | Medial leg and thigh | Posterior midline of leg |
| Nerve companion | Saphenous nerve | Sural nerve |
| Termination | Common femoral vein (SFJ) - groin | Popliteal vein (SPJ) - popliteal fossa |
| Varicose disease | ~60% of cases | ~20% of cases |
| Length | Longest vein in the body | Shorter |
| Variability | Moderate (AAGSV common) | High (SPJ position very variable) |
Anatomy Diagram
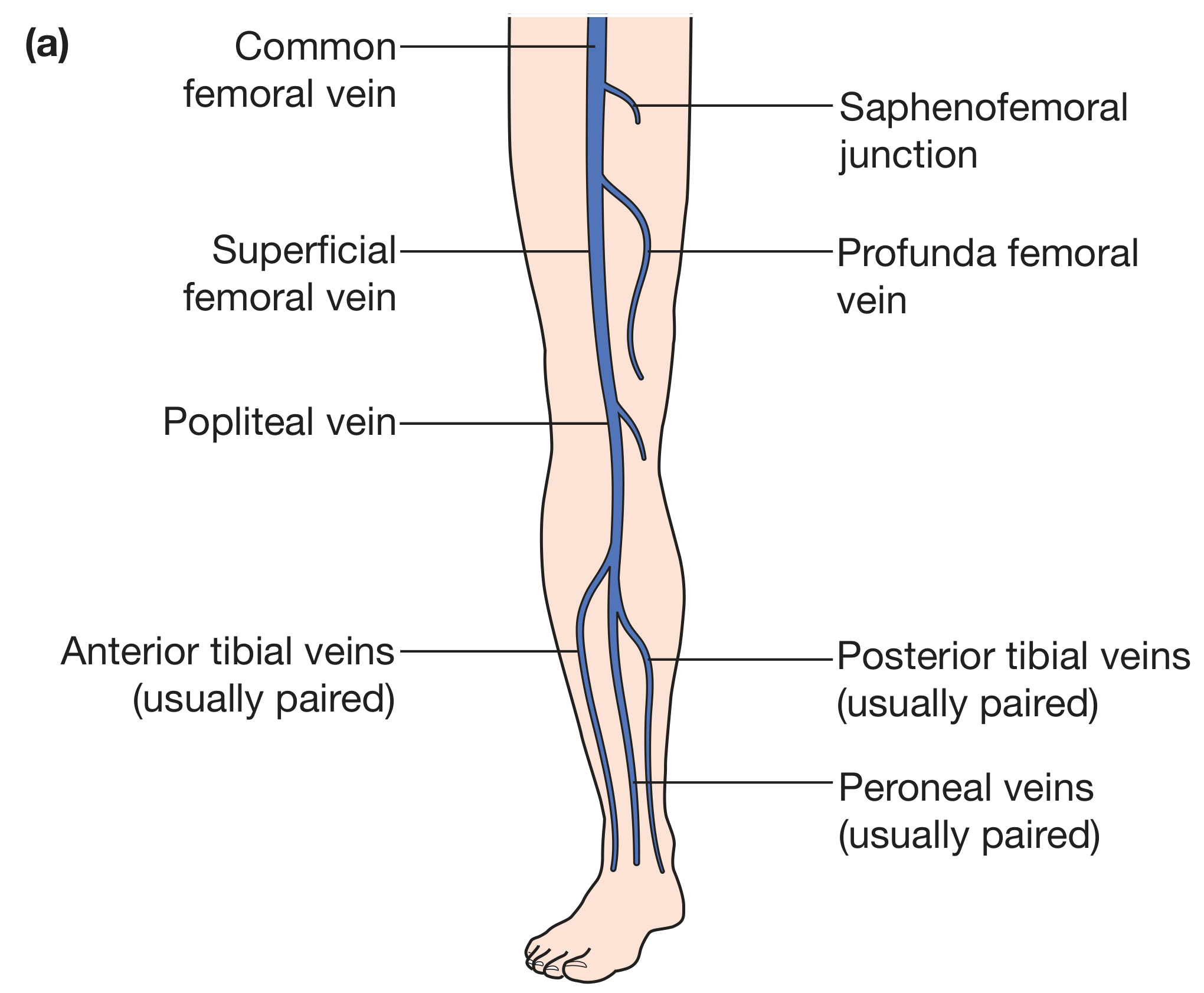
Figure 62.1(a) - Anatomy of the deep veins of the lower limb, showing the saphenofemoral junction. Bailey and Love's Short Practice of Surgery, 28th Ed.
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 62
What are named perforators and tributaries
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete account of named perforators and tributaries of the lower limb superficial venous system:
Named Tributaries
Tributaries at the Saphenofemoral Junction (SFJ)
The SFJ is not simply the GSV joining the femoral vein - it is a confluence of superficial inguinal veins, receiving several named tributaries just before the GSV pierces the cribriform fascia. These are:
| Tributary | Drainage area |
|---|---|
| Superficial Epigastric Vein (SEV) | Anterior abdominal wall, running upward toward the umbilicus |
| Superficial Circumflex Iliac Vein (SCIV) | Lateral abdominal wall and iliac region |
| Superficial External Pudendal Vein (EPV) | External genitalia |
| Anterior Accessory GSV (AA-GSV) | Anterolateral thigh, often arising near the lateral knee |
| Posterior Accessory GSV (PA-GSV) | Posteromedial thigh (also called the posteromedial thigh tributary) |
Clinical note: Dilated superficial epigastric veins ("caput medusae" pattern on the abdominal wall) indicate incompetence of the SEV and should alert the clinician to underlying deep venous obstruction, usually at the iliofemoral segment.
- Dermatology 2-Volume Set 5e; Imaging Anatomy - Bones, Joints, Vessels and Nerves
Named Tributaries of the GSV in the Leg
| Tributary | Course / Notes |
|---|---|
| Posterior Accessory GSV / Posterior Arch of Leonardo | Runs lateral to the GSV in the lower leg; continuation of the superficial network of the dorsum of the foot; joins the GSV at the knee. Frequently overlies the Cockett perforators - clinically important in ulcer disease |
| Anterior tributary of the leg | Runs anteriorly in the leg, joining the GSV |
| Giacomini vein | Cranial extension of the SSV that communicates with the GSV system |
Visual: SFJ and Tributaries
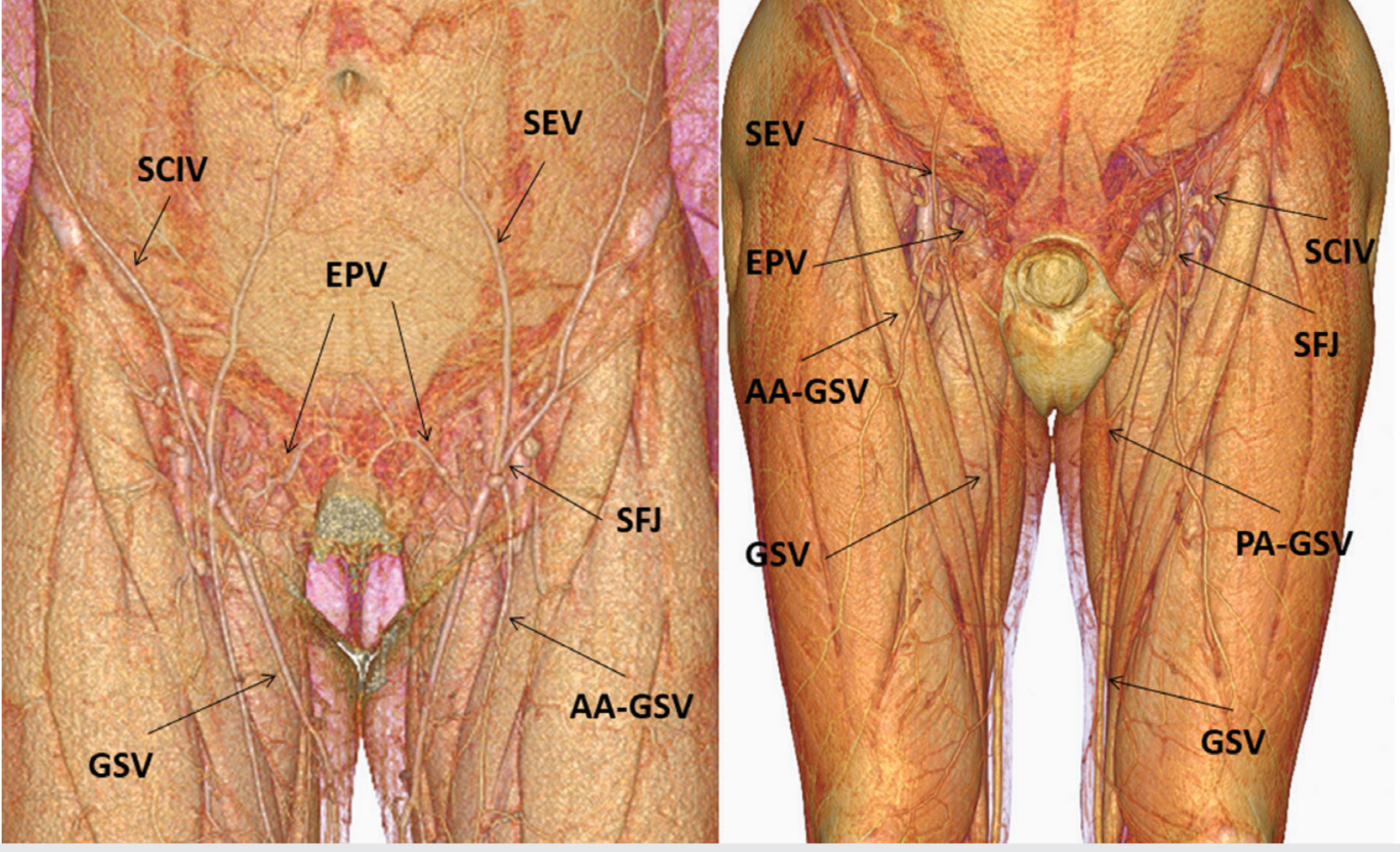
Fig. 12.3 - The confluence of superficial inguinal veins at the SFJ, showing SEV (superficial epigastric vein), SCIV (superficial circumflex iliac vein), EPV (external pudendal vein), AA-GSV, and PA-GSV. Imaging Anatomy, Volume 3.
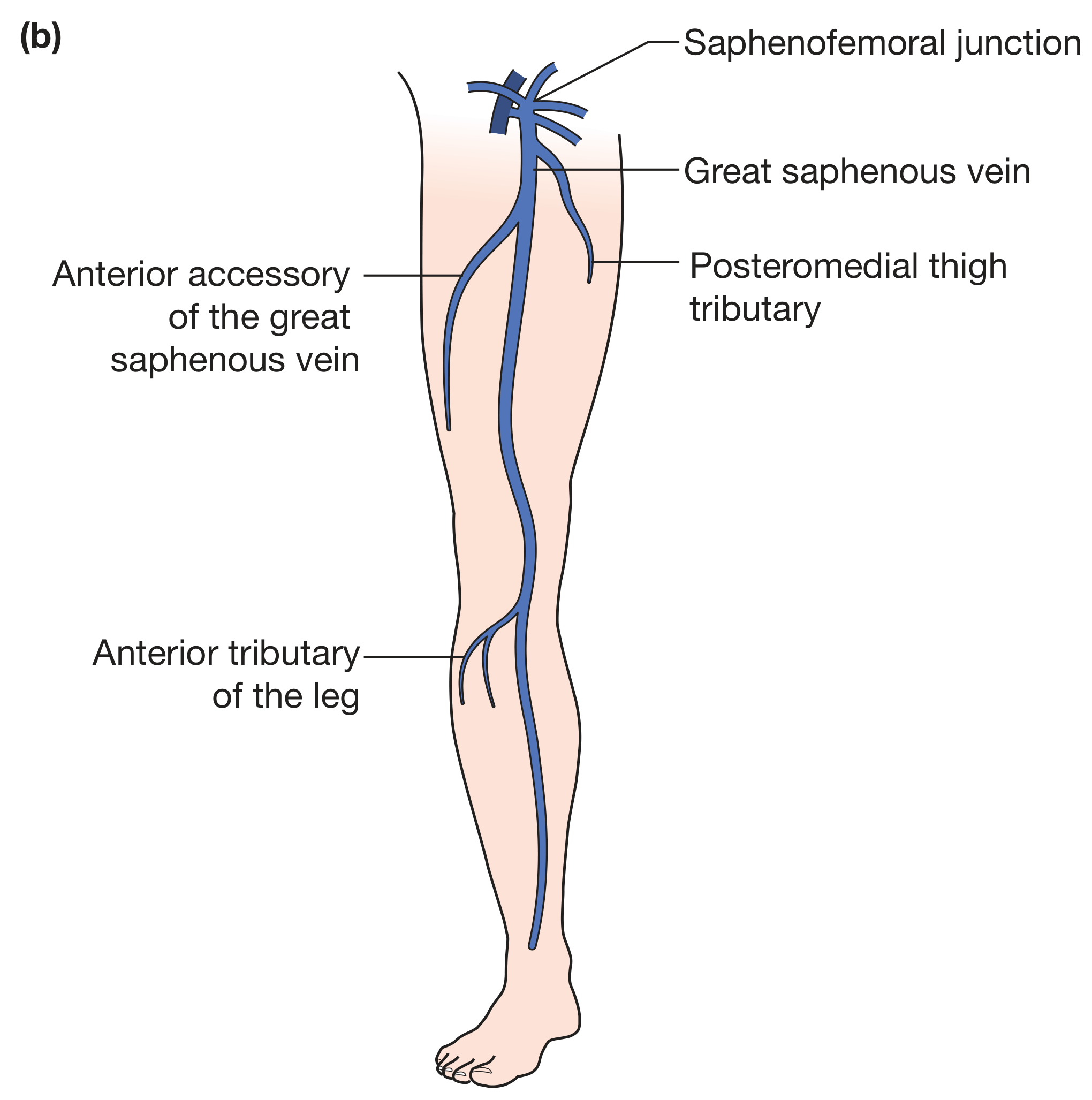
Fig. 62.1(b) - Superficial veins of the lower limb (great saphenous axis), showing the AAGSV and posteromedial thigh tributary. Bailey and Love's Short Practice of Surgery, 28th Ed.
Named Perforating Veins
Perforating (communicating) veins pierce the deep fascia to connect the superficial to deep venous system. They normally carry blood superficial → deep (valve direction). When incompetent, they allow outward reflux into superficial veins, causing or perpetuating varicosities and venous ulceration.
The four clinically important locations are: thigh, knee fold, upper medial leg, and lower medial leg.
Thigh Perforators
| Eponymous Name | Modern Name | Connection |
|---|---|---|
| Hunterian perforator | Femoral canal perforators (proximal) | GSV → femoral vein in the mid-thigh |
| Dodd's perforator | Femoral canal perforators (distal) | GSV → proximal popliteal / distal femoral vein in the distal thigh |
| Inguinal perforators | - | GSV → femoral vein in the proximal thigh |
| - | Posteromedial / posterolateral thigh perforators | Posterior thigh drainage |
Knee Perforators
| Eponymous Name | Modern Name | Connection |
|---|---|---|
| Boyd's perforator | Paratibial perforators (knee region) | GSV → posterior tibial veins in the upper third of the medial leg |
Upper Medial Leg Perforators (Paratibial)
Connect the posterior accessory GSV (Leonardo's arch) or GSV → posterior tibial veins in the upper calf.
Lower Medial Leg Perforators
| Eponymous Name | Modern Name | Connection |
|---|---|---|
| Cockett's perforators I, II, III | Posterior tibial perforators | Posterior accessory GSV (Leonardo's arch) → posterior tibial veins |
| - Cockett I: 7 cm above medial malleolus | ||
| - Cockett II: 13.5 cm above medial malleolus | ||
| - Cockett III: 18.5 cm above medial malleolus |
Cockett's perforators are the most clinically significant - their incompetence directly causes the high venous pressures responsible for skin changes and ulceration in the "gaiter area" (medial ankle/lower calf). Note that they connect to the posterior accessory GSV (Leonardo's arch), NOT the main GSV trunk directly.
Summary Table of Named Perforators
| Name | Location | Connects |
|---|---|---|
| Hunterian | Mid-thigh | GSV → femoral vein |
| Dodd's | Distal thigh | GSV → femoral/popliteal vein |
| Boyd's | Upper medial leg / knee | GSV → posterior tibial veins |
| Cockett's I, II, III | Lower medial leg (gaiter area) | Posterior arch (Leonardo) → posterior tibial veins |
Clinical Significance of Incompetent Perforators
-
Incompetent perforators transmit the high pressure of the deep venous system directly into the superficial system during calf muscle contraction
-
Number and size of incompetent perforators correlate directly with severity of chronic venous disease
-
Cockett's perforators are the key drivers of ankle/gaiter area skin changes and venous ulceration
-
Subfascial Endoscopic Perforator Surgery (SEPS) was developed specifically to interrupt incompetent Cockett perforators
-
Fitzpatrick's Dermatology; Bailey and Love's Short Practice of Surgery, 28th Ed.; Imaging Anatomy Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.