Ct head, principle, basics, use, evaluation, how to read , clinical co relation, with images as per standard books
CT head brain computed tomography normal anatomy
CT head hemorrhage stroke infarct pathology
CT head subdural epidural hematoma trauma skull fracture
CT brain subarachnoid hemorrhage hydrocephalus tumor
CT brain Hounsfield units attenuation table windows normal anatomy labeled
CT Head: Principles, Basics, Evaluation & Clinical Correlation
1. Historical Background & Introduction
- Low cost relative to MRI
- Rapidly acquired (5–10 seconds for a basic scan)
- Relatively low radiation dose
- Capable of rapid identification of haemorrhage, hydrocephalus, and herniation — all potentially treatable neurosurgical emergencies
- The key technique for differentiating ischaemic stroke from haemorrhage
- Feasible in medically unstable patients receiving active resuscitation
- Slip-ring technology (1980s): Continuous tube rotation; 1 second/image; enabled helical CTA
- Multidetector CT (MDCT, late 1990s): 64–320 detector rows; sub-0.3 second rotation; truly isometric voxels; high-quality multiplanar reconstructions
2. Basic Principles of CT
Detector System
- A scintillator absorbs x-rays → converts to visible light → photodiode → electrical signal → image
- Modern MDCTs use 64, 128, or 320 parallel detector rows simultaneously
Scanning Parameters
| Parameter | Typical Value |
|---|---|
| Slice thickness (brain) | ~3 mm standard; 0.4–0.6 mm for CTA/facial bones |
| Pitch | 1–2 (lower = higher dose; higher = gaps) |
| Gantry rotation time | 0.5–0.75 seconds |
| Tube voltage | 120 kV (adult) |
| Tube current | 200–400 mA (adult); reduced for children |
3. Hounsfield Units (HU) — The Language of CT
HU Reference Values for Neuroimaging
| Structure | Approximate HU |
|---|---|
| Air | −1000 |
| Fat | −100 to −50 |
| CSF / Water | 0–10 |
| White matter | 20–30 |
| Grey matter | 35–45 |
| Acute blood / Haemorrhage | 50–80 |
| Calcification | 100–400+ |
| Cortical bone | 400–1000+ |
Hyperdense = higher HU than brain (bright) — e.g. acute blood, calcification, contrast
Isodense = same HU as brain (may be hard to see)
Hypodense = lower HU than brain (dark) — e.g. oedema, infarct, CSF
4. Window Settings — How to Customise the Image
- Window Width (WW): The range of HUs displayed — wide = less contrast; narrow = more contrast
- Window Level (WL): The centre of the displayed range
Standard Window Presets
| Window | WL (HU) | WW (HU) | Use |
|---|---|---|---|
| Brain | 40 | 80 | Brain parenchyma, grey-white differentiation |
| Subdural / Blood | 70 | 150–200 | Acute haemorrhage, extra-axial collections |
| Bone | 400 | 2000–3000 | Skull fractures, calcification |
| Stroke | Narrowed WW | ↓WW | Enhances grey-white matter differentiation |
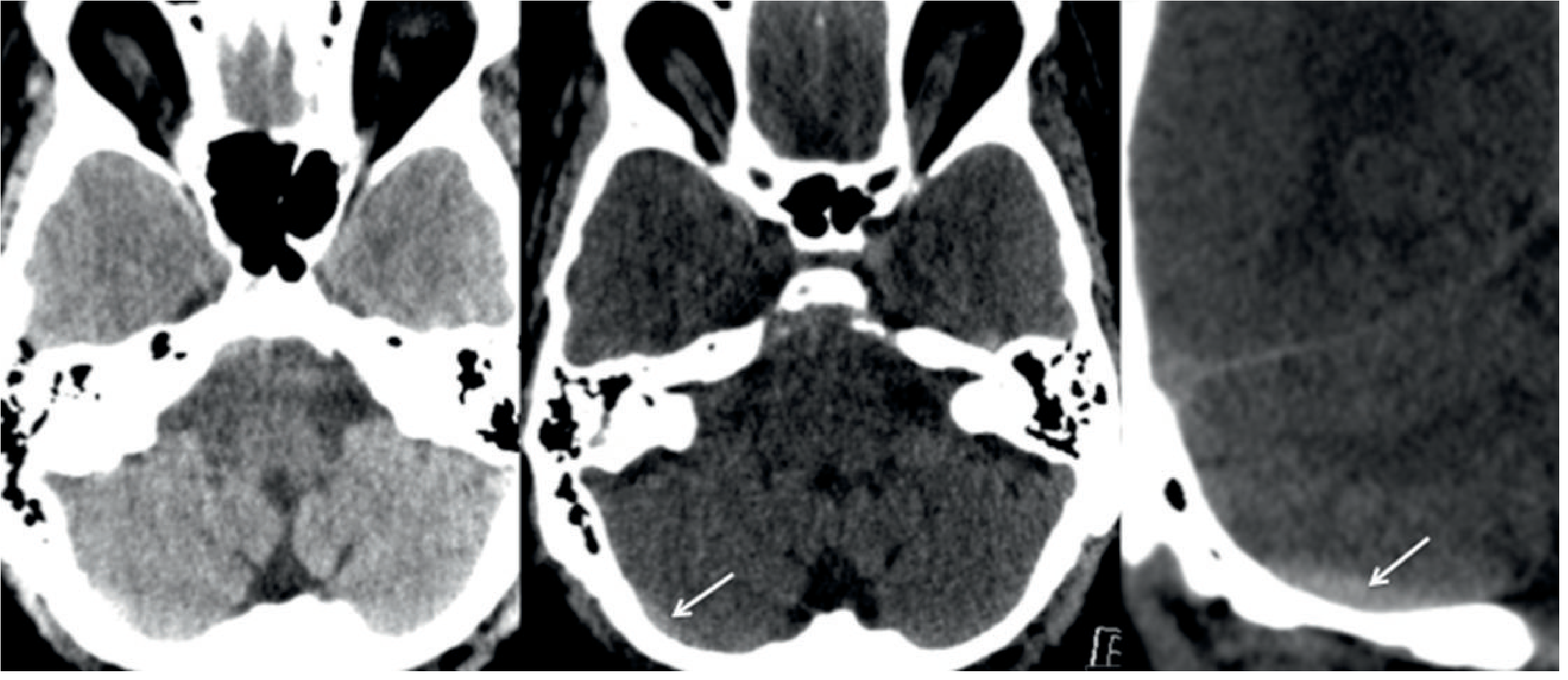
Tip: Small extra-axial haemorrhages — especially in the posterior fossa — can be occult on standard brain windows but visible on subdural/blood window settings (Fig. 54.2 in Grainger & Allison).
5. Indications for CT Head
Emergency / Acute Indications
- Head trauma — most frequent indication; replaced skull X-ray
- Acute stroke — differentiates ischaemia from haemorrhage; combined with CTA (aortic arch to skull vertex)
- Suspected subarachnoid haemorrhage (SAH) — thunderclap headache
- New-onset seizure / altered consciousness
- Acute headache — rule out haemorrhage, raised ICP
- Suspected meningitis/encephalitis — pre-lumbar puncture screening
- Hydrocephalus — shunt assessment
Elective Indications
- Known or suspected intracranial tumour / metastases
- Pre-surgical planning (complex fractures, vascular malformations)
- Follow-up of known pathology
- Dementia workup (structural causes)
6. Intravenous Contrast
- Characterise known pathology with blood-brain barrier breakdown (tumour, abscess, inflammation)
- CTA for vascular assessment (aneurysm, stenosis, AVM)
Contrast Precautions
- eGFR < 30 mL/min/1.73 m²: Avoid if possible (risk of contrast-induced nephropathy); prehydration if essential
- Known contrast allergy: Premedicate with antihistamines/corticosteroids (though no definite reduction in severe reactions)
- Mild reactions (1 in 10): Flushing, nausea, vomiting, urticaria
- Severe anaphylaxis: ~1 in 100,000
- Hyperthyroidism: Risk of delayed thyrotoxicosis (up to 8 weeks post-contrast)
- Breastfeeding: Can continue after iodinated contrast per most guidelines
7. Multiplanar Reconstructions
| Plane | Clinical Use |
|---|---|
| Axial | Standard; deep brain structures, cerebral parenchyma |
| Sagittal | Midline structures — corpus callosum, pituitary, clivus, craniocervical junction |
| Coronal | Orbits, sinuses, anterior/middle cranial fossae, occipital condyles; herniation syndromes; vertex haemorrhage |
| MIP | Maximum intensity projection — vascular (CTA) |
| VR/3D | Volume rendering — surgical planning, fracture assessment |
8. Systematic Approach to Reading a CT Head
Step 1 — Technical Adequacy
- Patient positioning, rotation, motion artefact?
- Correct windows applied?
Step 2 — Skull & Scalp (Bone Window)
- Fractures (linear, depressed, comminuted)
- Scalp swelling/haematoma localises point of impact
- Sutural diastasis
- Intracranial calcifications (pineal, choroid plexus — normal landmarks for midline)
Step 3 — Extra-Axial Spaces
- Epidural space: Biconvex (lenticular) hyperdense collection — bounded by sutures
- Subdural space: Crescent-shaped collection — crosses sutures, conforms to brain surface
- Subarachnoid space: Basal cisterns (suprasellar, perimesencephalic, Sylvian), interhemispheric fissure
- Subgaleal / subperiosteal collections
Step 4 — Brain Parenchyma (Brain Window)
- Grey-white matter differentiation preserved?
- Any focal hypodensity (oedema, infarct) or hyperdensity (haemorrhage, calcification)?
- Basal ganglia, thalami, internal capsule, brainstem
Step 5 — Ventricles and Cisterns
- Size and symmetry of lateral ventricles (temporal horns should be <2 mm normally)
- Third and fourth ventricle
- Hydrocephalus? (obstructive vs. communicating)
- Cisternal effacement = raised ICP
Step 6 — Midline
- Falx cerebri — midline shift? (>5 mm is significant)
- Pineal gland displacement
Step 7 — Posterior Fossa
- Cerebellum, brainstem
- Beam-hardening artefact at petrous apices is a major limitation here — use thin slices
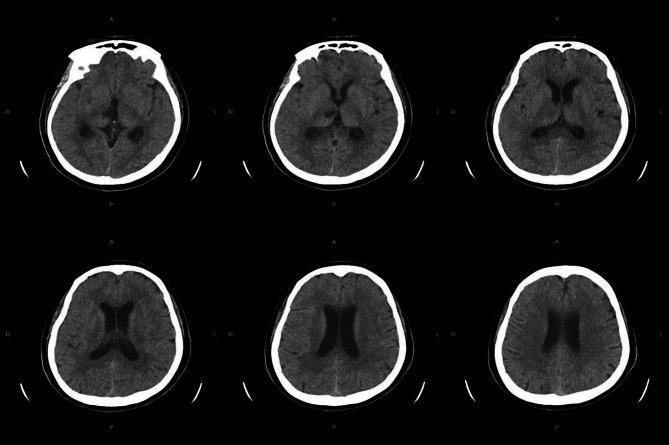
9. Normal CT Head Anatomy
10. Artefacts & Limitations
| Artefact | Cause | Appearance |
|---|---|---|
| Motion artefact | Patient movement (confusion, respiratory) | Blurred images |
| Beam hardening | Absorption of low-energy x-rays | Streaky hypoattenuation — worst between petrous apices |
| Partial volume | High + low density structure in same voxel | Averaged density — can mask pathology |
| Metallic streak | Intracranial metalware, dental amalgam | Star/streak artefact — obscures adjacent structures |
11. Clinical Correlations with Images
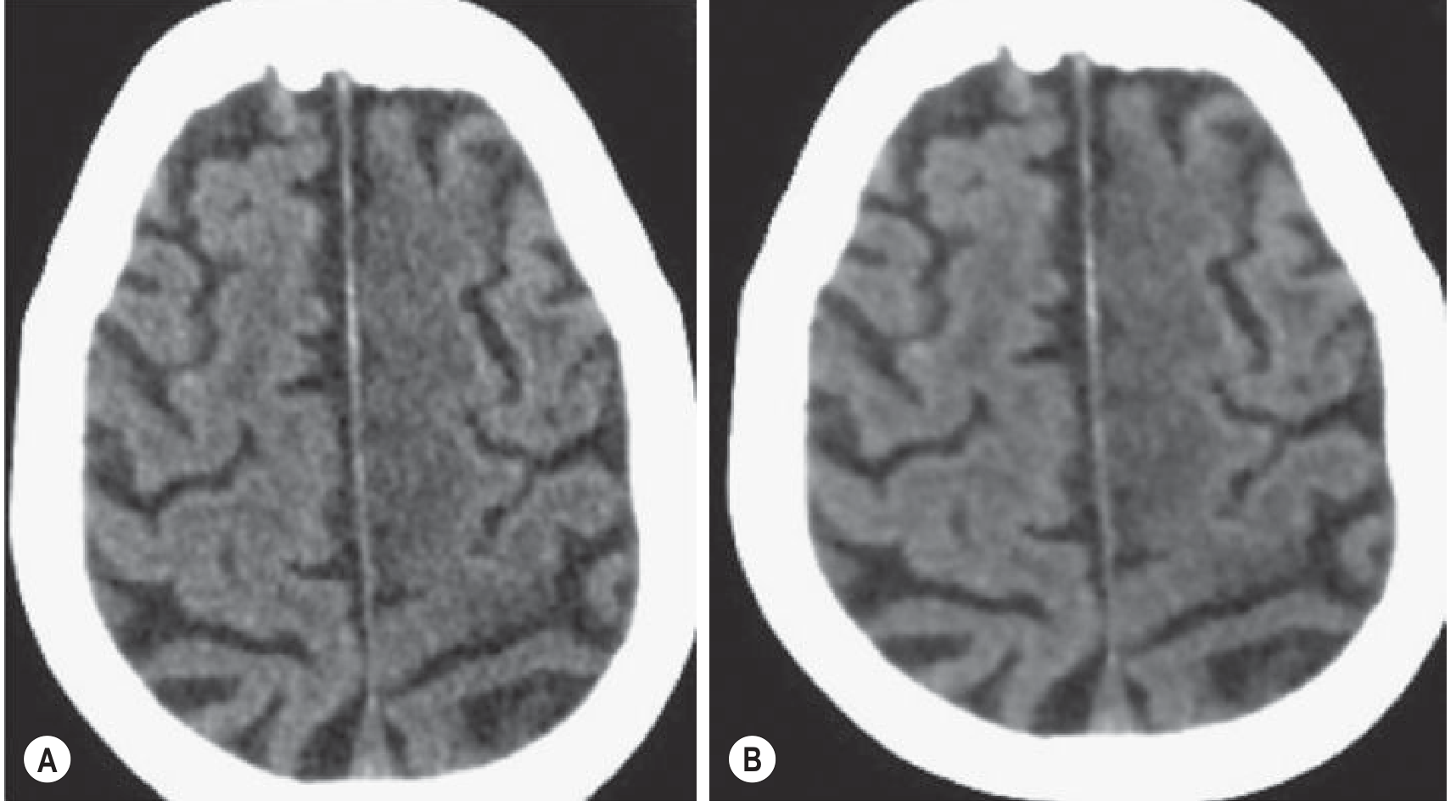
11.1 Acute Ischaemic Stroke
- Loss of grey-white differentiation in MCA territory
- Sulcal effacement
- Hyperdense MCA sign (clot in artery ~70–80 HU)
- "Insular ribbon" sign — loss of normal insular cortex definition
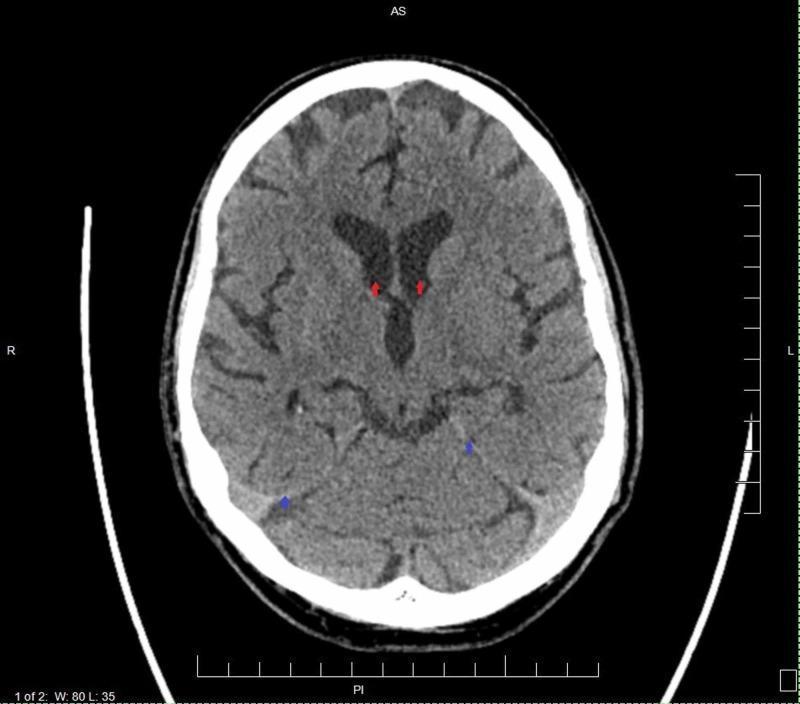
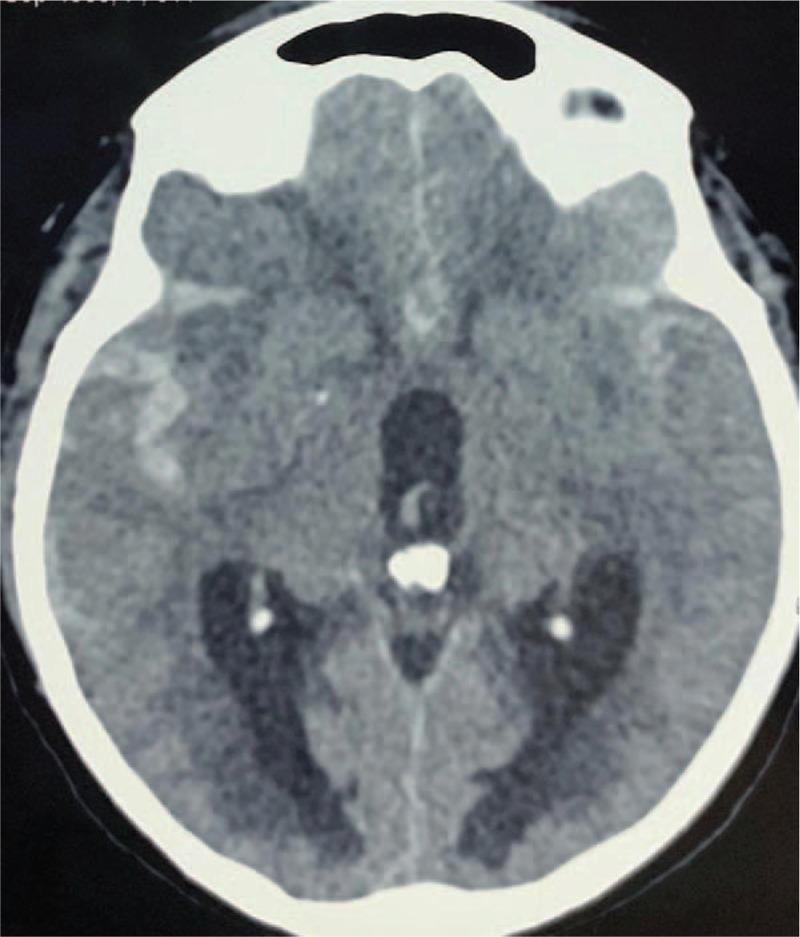
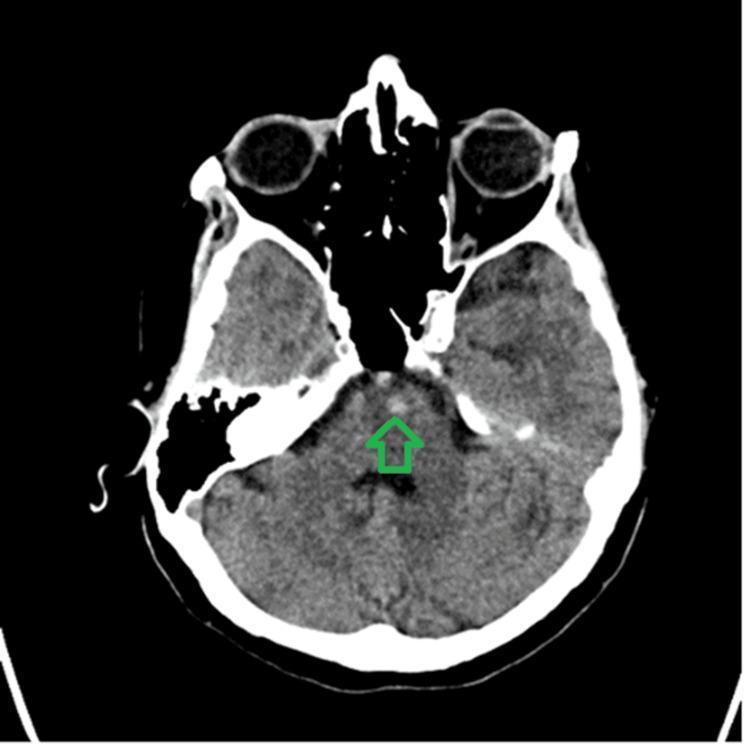
11.2 Subarachnoid Haemorrhage (SAH)
Sensitivity: ~98% within 6 hours (decreases over days as blood becomes isodense)
Complication: Acute hydrocephalus (temporal horn dilatation)

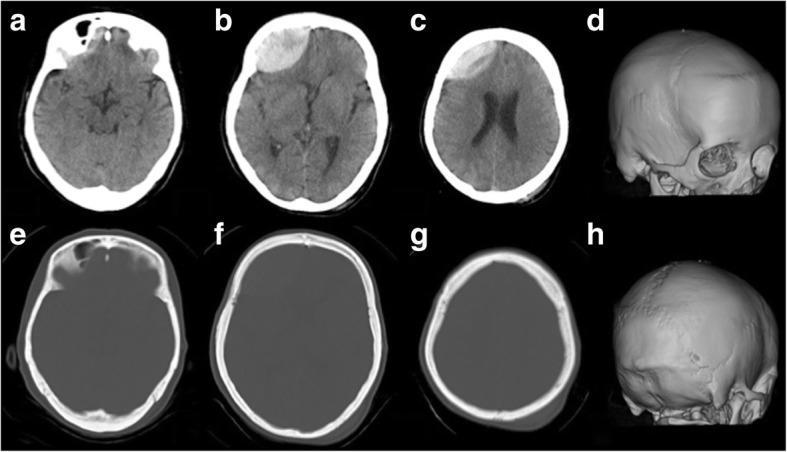
11.3 Epidural Haematoma (EDH)
CT appearance: Biconvex (lenticular), hyperdense extra-axial collection; bounded by cranial sutures; does NOT cross sutures
Clinical: "Lucid interval" followed by rapid deterioration — neurosurgical emergency

11.4 Subdural Haematoma (SDH)
CT appearance: Crescent-shaped collection that crosses sutures (follows brain surface)
| Timing | Density on CT |
|---|---|
| Acute (<3 days) | Hyperdense (50–70 HU) |
| Subacute (3 days–3 weeks) | Isodense (may be missed) |
| Chronic (>3 weeks) | Hypodense (similar to CSF) |
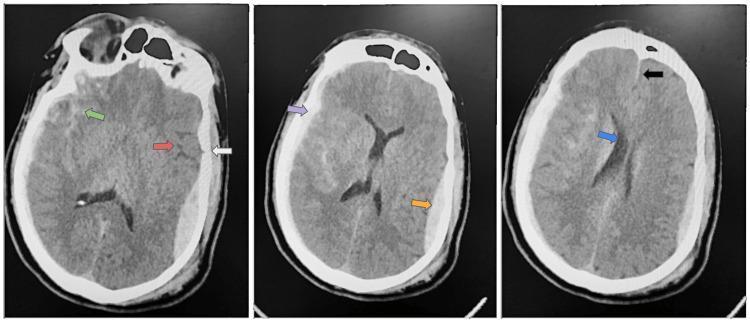
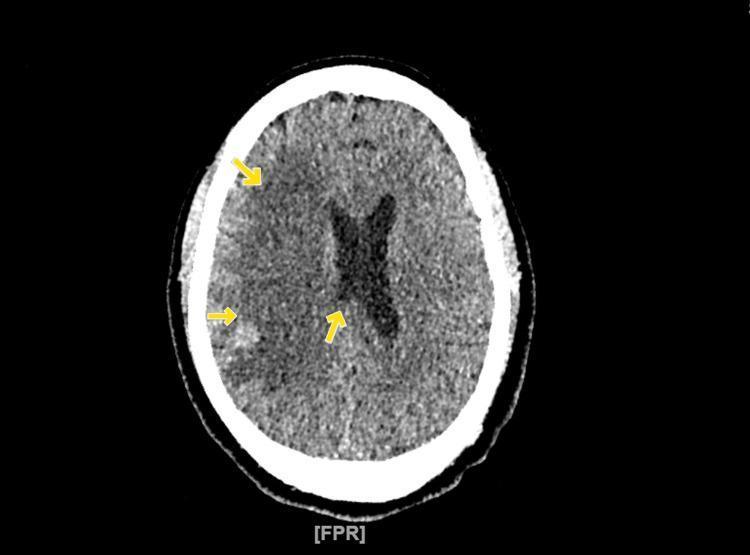
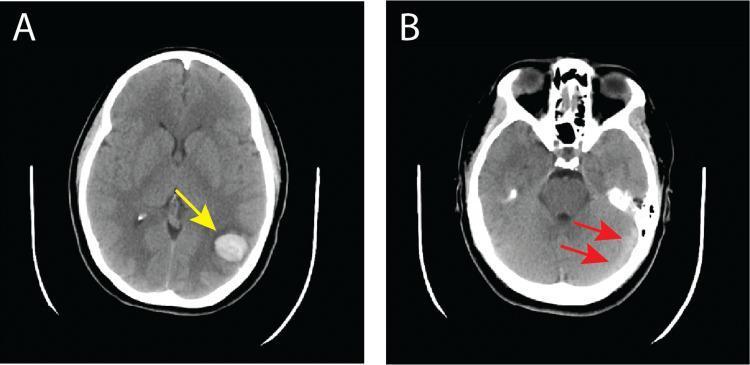
11.5 Intracerebral/Hypertensive Haemorrhage
CT appearance: Well-defined hyperdense lesion; surrounding hypodense oedema halo
Resolution: Liquefies over weeks → becomes hypodense
11.6 Cerebral Venous Sinus Thrombosis (CVST)
- Hyperdense sinus sign (dense transverse/superior sagittal sinus ~60–70 HU)
- Cord sign — hyperdense cortical vein
11.7 Haemorrhagic Transformation of Ischaemic Stroke
ECASS Classification: HI1, HI2 (petechial), PH1, PH2 (parenchymal haematoma)

11.8 Normal CT vs. Pathology — Quick Reference
| Finding | Density | Location | Likely Diagnosis |
|---|---|---|---|
| Biconvex hyperdense | Hyperdense | Extra-axial | Epidural haematoma |
| Crescent hyperdense | Hyperdense | Extra-axial | Acute SDH |
| Crescent hypodense | Hypodense | Extra-axial | Chronic SDH |
| Basal cisterns hyperdense | Hyperdense | Subarachnoid | SAH |
| Focal hypodense + mass effect | Hypodense | Parenchyma | Ischaemic infarct + oedema |
| Focal hyperdense, deep | Hyperdense | Basal ganglia/thalamus | Hypertensive haemorrhage |
| Midline hyperdense sinus | Hyperdense | Dural sinuses | CVST |
| Rim-enhancing lesion | Ring on contrast | Parenchyma | Abscess / GBM |
12. Summary: Key Teaching Points
- HU scale underpins everything — acute blood is hyperdense (50–80 HU); oedema/infarct is hypodense; CSF is ~0 HU
- Window settings must be adjusted for each clinical question — always apply both brain and bone windows
- EDH = biconvex, bounded by sutures; SDH = crescent, crosses sutures
- SAH = blood in basal cisterns — check Sylvian fissures, interhemispheric fissure
- Early ischaemic stroke may be very subtle — look for loss of grey-white differentiation and sulcal effacement
- Posterior fossa is a blind spot on CT — use thin slices and multiplanar reformats
- Coronal reformats are essential for vertex/tentorial haemorrhage and herniation syndromes
- Always review bone windows for fractures, even if clinical question is vascular
Mri head, baics, interpretation, types, how to read, use, clinical co relation, examples, indicarion, contraindication , recent updates as per standard books in notes format for PG resident
MRI brain sequences T1 T2 FLAIR DWI normal anatomy comparison
MRI brain stroke DWI ADC diffusion restriction acute ischemic infarct
MRI brain multiple sclerosis demyelination white matter lesion tumor glioma
MRI brain meningioma abscess ring enhancement gadolinium contrast tumor
MRI brain hemorrhage T1 T2 signal methemoglobin hemosiderin evolution
MRI brain functional fMRI DTI tractography perfusion ASL advanced sequences
MRI Head — Complete PG Resident Notes
SECTION 1 — BASICS & PHYSICS
1.1 What is MRI?
- Noninvasive diagnostic technique using nonionising electromagnetic radiation — NO X-ray, NO radiation dose
- Uses a powerful superconducting magnet + radiofrequency (RF) pulses + magnetic field gradients
- Images the distribution of hydrogen nuclei (protons) in water and lipids
- Superior soft-tissue contrast compared to CT
- Scan time: 10 min (simple brain) to >60 min (complex protocol with contrast)
- Disadvantages: longer scan time, higher cost, limited availability, multiple contraindications
1.2 Historical Landmarks
| Year | Event |
|---|---|
| 1971 | Damadian differentiates normal vs. tumour tissue by NMR |
| 1977 | First human body MRI scan (Damadian) |
| 1978 | First human head MRI image (Clow & Young, EMI) |
| 2003 | Nobel Prize — Lauterbur & Mansfield (frequency encoding + slice selection) |
1.3 How MRI Works — Step by Step
- Patient placed in static magnetic field (B₀)
- Proton spins align parallel or antiparallel to B₀ (slight excess parallel → net magnetisation M in z-direction)
- RF pulse flips M into the transverse (x/y) plane
- Protons precess in phase → generate a Free Induction Decay (FID) signal
- After RF pulse OFF → protons relax back to equilibrium
- Two independent relaxation processes:
- T1 relaxation (longitudinal): Recovery of Mz — "spin-lattice relaxation"
- T2 relaxation (transverse): Decay of Mxy — "spin-spin relaxation"
- Three gradient coils encode frequency, phase, and slice location
- Data fills k-space → Fourier transform → recognisable image
- Spin Echo (SE): 90° + 180° RF pulses → reliable T1/T2 weighting
- Gradient Echo (GRE): Shorter TR, faster, T2* weighted — sensitive to susceptibility effects (blood, calcium)
- Inversion Recovery (IR): Preparatory 180° pulse → FLAIR, STIR
1.4 Key Timing Parameters
| Parameter | Definition | Effect |
|---|---|---|
| TR (Repetition Time) | Time between RF pulses | Short TR → T1W; Long TR → T2W/PD |
| TE (Echo Time) | Time from excitation to echo | Short TE → T1W/PD; Long TE → T2W |
| TI (Inversion Time) | Inversion recovery delay | FLAIR: long TI to null CSF; STIR: short TI to null fat |
SECTION 2 — MRI SEQUENCES & THEIR CLINICAL MEANING
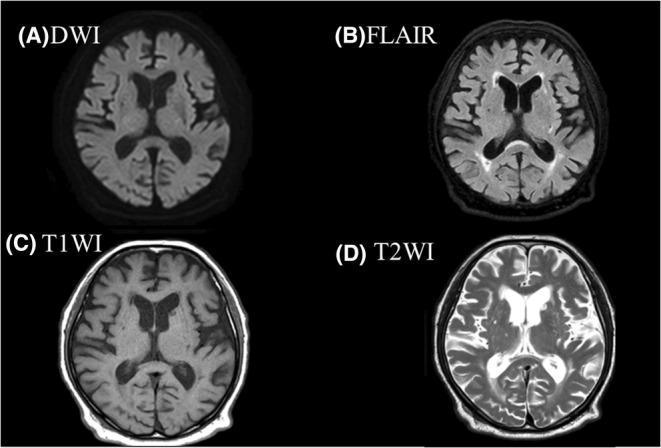
2.1 Core Sequences — The Fundamental Five
| Sequence | CSF | Grey Matter | White Matter | Fat | Pathological Oedema | Best For |
|---|---|---|---|---|---|---|
| T1W | Dark | Grey | Bright | Bright | Dark | Anatomy, post-contrast, subacute bleed, fat, calcification |
| T2W | Bright | Bright | Dark | Bright | Bright | Pathology detection, oedema, CSF spaces, posterior fossa |
| FLAIR | Dark (suppressed) | Grey | Dark | Variable | Bright | Periventricular lesions (MS), subtle cortical disease, SAH |
| DWI | Dark | Grey | Dark | Dark | Bright (acute infarct) | Acute ischaemia (minutes), abscess, epidermoid |
| GRE / T2* | Dark | Grey | Dark | Bright | Variable | Blood products, calcification, microhaemorrhages, SWI |
PG Memory Aid:
- T1 = "Tissue" — anatomy, bright fat, subacute blood (methemoglobin)
- T2 = "water (Two)" — water is bright, pathology lights up
- FLAIR = "Fluid Attenuated" — CSF goes dark, lesions near ventricles become obvious
- DWI = "Diffusion" — acute stroke lights up in minutes
2.2 Advanced/Specialised Sequences
| Sequence | Full Name | Clinical Use |
|---|---|---|
| SWI | Susceptibility-Weighted Imaging | Microhaemorrhages, amyloid angiopathy, cavernomas, veins, iron deposition |
| MRA | MR Angiography (TOF, PC) | Aneurysm, AVM, stenosis, CVST — without contrast |
| MRV | MR Venography | Cerebral venous sinus thrombosis |
| MR Perfusion | DSC, ASL, DCE | Stroke penumbra, tumour grading, vasospasm |
| MRS | MR Spectroscopy | Tumour (NAA↓, Cho↑, Cr), abscess (lactate, succinate peaks), epilepsy focus |
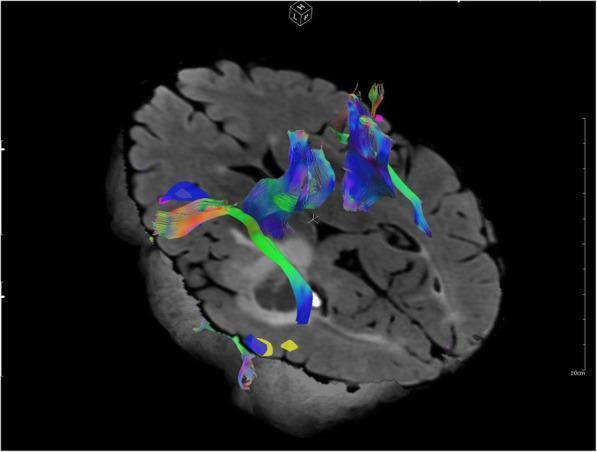
| DTI | Diffusion Tensor Imaging | White matter tract integrity; tractography for surgical planning |
| fMRI | Functional MRI (BOLD) | Eloquent cortex mapping pre-surgery (motor, language, visual areas) |
| ASL | Arterial Spin Labelling | Perfusion without gadolinium; increasingly used in stroke, dementia |
| DWI/ADC | Diffusion Weighted + Apparent Diffusion Coefficient | Confirms true restriction vs. T2 shine-through |
SECTION 3 — SIGNAL INTENSITY — WHAT IS BRIGHT/DARK?
3.1 T1 Signal — Bright (Hyperintense) Structures
Mnemonic: "FATMID"
| Bright on T1 | Why |
|---|---|
| Fat | Short T1 |
| Acute/subacute blood (methemoglobin) | Paramagnetic effect |
| Tumour (melanoma mets, colloid cyst) | Protein/melanin/blood |
| Manganese/gadolinium contrast | Paramagnetic |
| Infarct (subacute, cortical laminar necrosis) | Protein denaturation |
| Dermoid, lipoma | Fat content |
3.2 T2 Signal — Bright (Hyperintense) Structures
Mnemonic: "VESSEL"
| Bright on T2 | Why |
|---|---|
| Vasogenic oedema | ↑ extracellular water |
| Enlarging infarct (after 24 h) | Cytotoxic → vasogenic oedema |
| SAH (subacute, on FLAIR) | Blood products in CSF |
| Sclerosis/demyelination (MS plaques) | Demyelination + oedema |
| Encephalitis / abscess / tumour | ↑ water content |
| Lesions of any type (most) | Water ↑ |
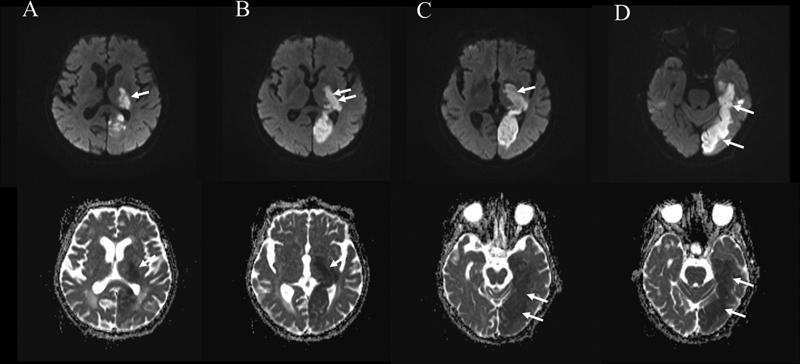
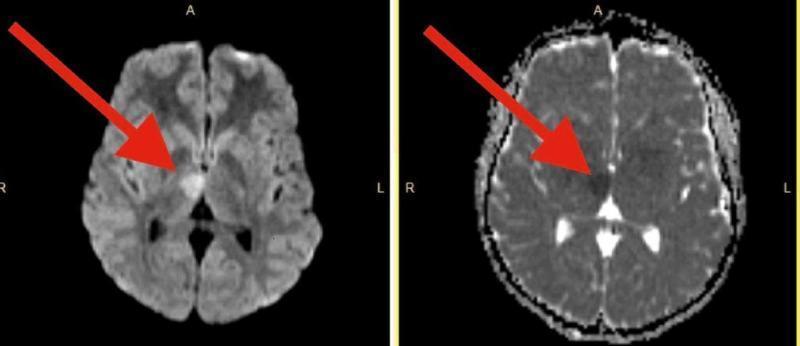
3.3 DWI Interpretation — Critical for PG Residents
| DWI | ADC Map | Interpretation |
|---|---|---|
| ↑ Bright | ↓ Dark | True restriction — acute infarct, abscess, dense tumour |
| ↑ Bright | ↑ Bright | T2 shine-through — not true restriction (MS chronic, tumour) |
| ↓ Dark | ↑ Bright | Facilitated diffusion — chronic MS, necrosis |
SECTION 4 — INDICATIONS FOR MRI BRAIN
Primary Indications
- Seizures / epilepsy
- Cranial nerve dysfunction
- Diplopia / visual disturbance
- Ataxia
- Acute and chronic neurological deficits
- Suspicion of neurodegenerative disease (dementia, Parkinson's)
- Primary and secondary neoplasm
- Intracranial aneurysm
- Cortical dysplasia / morphological brain abnormalities
- Vasculitis
- Encephalitis / meningitis and complications
- Brain maturation assessment (paediatric)
- Headache (complex/red-flag)
- Mental status change
- Hydrocephalus
- Ischaemic disease / infarction
- Suspected pituitary dysfunction
- Demyelination / dysmyelination
- Vascular malformations
Extended/Specialised Indications
- Functional imaging / brain mapping (pre-surgical)
- Blood flow and brain perfusion
- MR Spectroscopy (tumour, infection, epilepsy)
- Volumetry and morphometry (dementia research)
- Tractography (DTI — surgical planning)
- Post-traumatic assessment
- Haemorrhage characterisation / follow-up
SECTION 5 — CONTRAINDICATIONS
Absolute Contraindications
- Ferromagnetic cerebral aneurysm clips (older generation)
- Cochlear implants (older non-MR-conditional)
- Certain cardiac devices: Older pacemakers, ICDs, neurostimulators without MR-conditional certification
- Metallic intraocular foreign bodies (e.g., metal workers — screening mandatory)
- Ferromagnetic intracranial hardware
Relative Contraindications (needs risk-benefit assessment)
- Modern MR-conditional pacemakers/ICDs — permissible at 1.5 T with strict protocols
- Claustrophobia — requires sedation/anaesthesia; open MRI as alternative
- First trimester of pregnancy — generally safe after 1st trimester; MRI preferred over ionising radiation when clinical necessity justifies; contrast (Gd) generally avoided throughout pregnancy
- Cochlear implants — some are MR-conditional (1.5 T or 3 T); verify manufacturer data
- Severe renal impairment (eGFR <30) — gadolinium contraindicated due to risk of Nephrogenic Systemic Fibrosis (NSF) — avoid older linear Gd agents; macrocyclic agents have lower risk
Key Safety Points for PG Residents
- MRI magnetic field is ALWAYS ON (even when not scanning)
- Field strength may exceed 60,000× Earth's magnetic field
- All patients, staff, and equipment must be safety-screened before entering the scan room
- Heating of metallic implants is a risk
- Website: www.mrisafety.com (check device compatibility before scanning)
- Breastfeeding: continue normally after gadolinium (very minimal excretion)
- Hearing protection mandatory for patient (gradient coil noise)
SECTION 6 — GADOLINIUM CONTRAST
When to Use
- Blood-brain barrier (BBB) breakdown: tumour, abscess, encephalitis, active MS, meningitis
- Characterise lesion after non-contrast abnormality found
- Pituitary, cranial nerve, meningeal disease
- Post-operative assessment (residual tumour vs. surgical change)
- Active inflammation vs. chronic scar
How It Works
- Gadolinium is paramagnetic → causes T1 shortening → bright signal on T1W post-contrast
- Normally excluded from brain by intact BBB
- Enhances where BBB is disrupted
Enhancement Patterns — Key Clinical Correlations
| Pattern | Description | Differential Diagnosis |
|---|---|---|
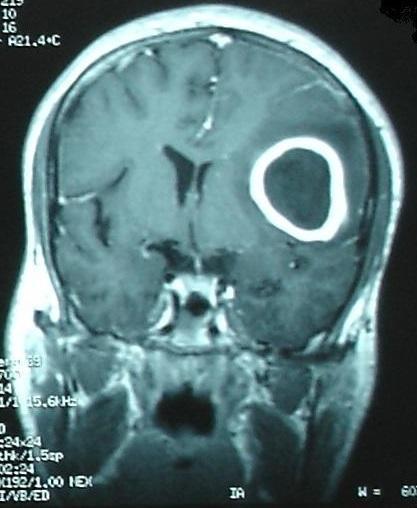
| Ring/rim enhancement | Peripheral bright rim, dark centre | High-grade glioma (GBM), abscess, metastasis, tumefactive MS |
| Homogeneous solid enhancement | Uniform brightening | Meningioma, lymphoma, WHO grade I tumour |
| Leptomeningeal enhancement | Sulcal/basal enhancement | Meningitis (bacterial, fungal, TB), carcinomatous meningitis |
| Dural tail sign | Enhancing dura adjacent to mass | Meningioma (classic but not pathognomonic) |
| Gyral enhancement | Cortical surface enhancement | Subacute infarct (luxury perfusion), herpes encephalitis |
| Nodular enhancement | Small discrete foci | Metastases, sarcoid, demyelinating plaques |
| Periventricular enhancement | Around ventricles | Lymphoma, CMV ventriculitis |
Gadolinium Safety
- Nephrogenic systemic fibrosis (NSF): Rare, severe; avoid in eGFR <30 (especially older linear agents like gadodiamide, gadopentetate)
- Brain deposition: Gadolinium accumulates in dentate nuclei and globus pallidus with repeated dosing — significance uncertain; macrocyclic agents (gadobutrol, gadoterate) have significantly lower deposition
- Recent guidance: use lowest effective dose; prefer macrocyclic agents for repeated scans
- Allergic reactions: Rare (<1%); urticaria most common; true anaphylaxis extremely rare
SECTION 7 — HOW TO READ AN MRI BRAIN — SYSTEMATIC APPROACH
Step 1 — Check Technical Quality
- Correct sequences acquired?
- Motion artefact? (ghosting, blurring)
- Field of view adequate?
- Pre- AND post-contrast if requested?
Step 2 — T1W First (Anatomy)
- Overall brain volume (atrophy?)
- Sulcal effacement or enlargement?
- Midline shift?
- T1 bright lesions: fat, blood, Gd contrast, calcification (rare on T1)
- Pituitary fossa, brainstem, cerebellum (no beam hardening artefact unlike CT)
Step 3 — T2W (Pathology Detection)
- Any focal hyperintensity?
- Distribution: cortical, subcortical, periventricular, deep white matter, basal ganglia, thalamus, brainstem, cerebellum
- CSF space enlargement — hydrocephalus?
- Posterior fossa: cerebellar/brainstem lesions (MRI superior to CT here)
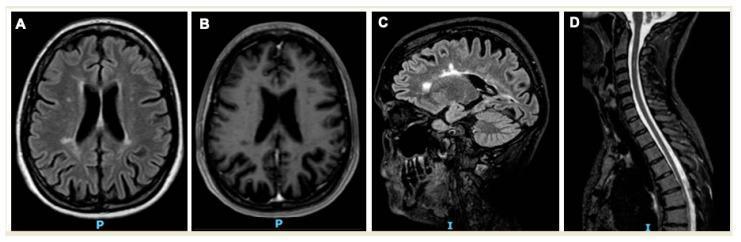
Step 4 — FLAIR (Periventricular & Cortical Lesions)
- CSF suppressed → periventricular lesions become obvious
- MS plaques: ovoid, periventricular, perpendicular to ventricles ("Dawson's fingers")
- Cortical lesions, leptomeningeal spread
- SAH: blood in CSF sulci → bright on FLAIR
Step 5 — DWI + ADC (Acute Pathology)
- Acute ischaemia: DWI ↑, ADC ↓ → detectable within minutes to hours (MRI advantage over CT)
- Abscess: DWI ↑ (restricted pus)
- Epidermoid cyst: DWI ↑ (restricted diffusion, cholesterol)
- Confirm with ADC map to exclude T2 shine-through
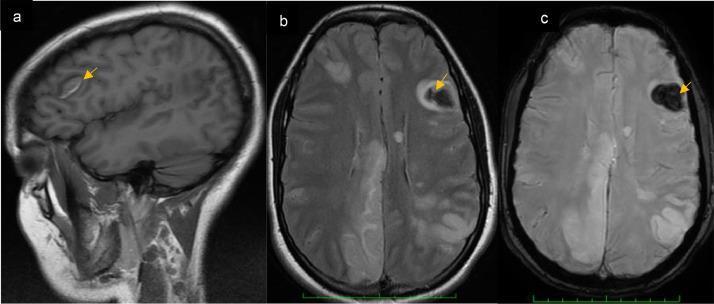
Step 6 — GRE/SWI (Blood & Susceptibility)
- Haemorrhage (any age), microbleeds, cavernoma, calcification
- "Blooming artefact" — lesion appears larger on GRE/SWI than on other sequences → characteristic of blood products
Step 7 — Post-Contrast T1W (Enhancement)
- BBB breakdown sites?
- Enhancement pattern (see Section 6)
- New enhancing lesions (MS activity, new metastases)
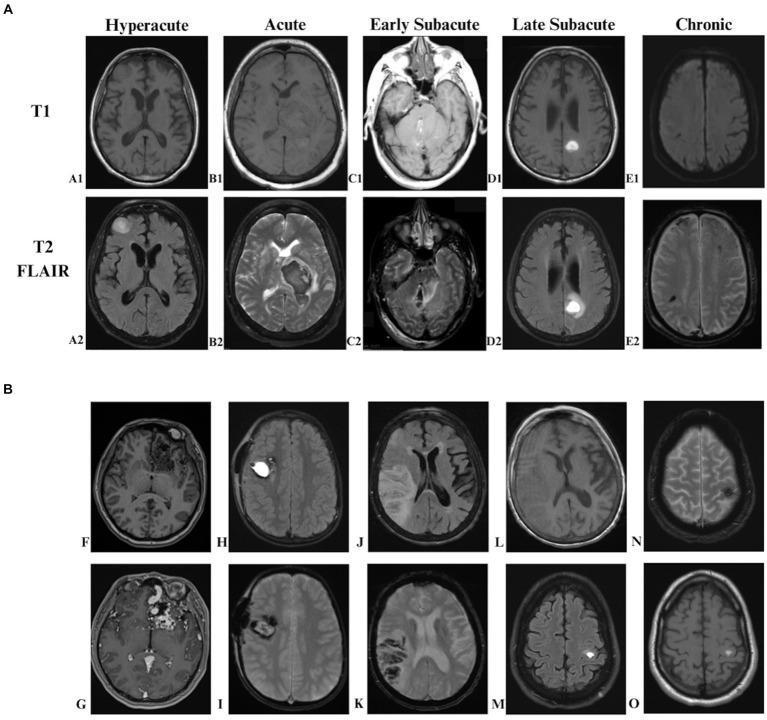
SECTION 8 — MRI SIGNAL OF HAEMORRHAGE OVER TIME
Evolution of Intracranial Haemorrhage on MRI
| Stage | Time | Blood Product | T1 | T2 | T2*/GRE |
|---|---|---|---|---|---|
| Hyperacute | 0–6 hours | Intracellular oxyhaemoglobin | Isointense (grey) | Isointense / slightly bright | Dark (susceptibility) |
| Acute | 1–3 days | Intracellular deoxyhaemoglobin | Isointense (grey) | Dark | Very dark (blooming) |
| Early subacute | 3–7 days | Intracellular methaemoglobin | Bright | Dark | Dark |
| Late subacute | 7–30 days | Extracellular methaemoglobin | Bright | Bright | Variable |
| Chronic | >14 days–months | Haemosiderin (ferritin) rim | Dark rim | Dark rim (black) | Black (blooming) |
PG Tip: "Bright on T1 = subacute bleed (methemoglobin)." Chronic blood leaves a permanent dark hemosiderin rim on T2/GRE.
SECTION 9 — CLINICAL CORRELATIONS WITH IMAGES
9.1 Acute Ischaemic Stroke
- DWI: ↑ (bright) — detectable within minutes (vs. CT negative for 6–24 h)
- ADC: ↓ (dark) — confirms true cytotoxic oedema
- FLAIR: may be normal <4.5 h — DWI+/FLAIR− mismatch = golden window for thrombolysis
- MRA: vessel occlusion
9.2 Multiple Sclerosis (MS)
- FLAIR/T2: Multiple ovoid periventricular hyperintense plaques
- Dawson's Fingers: Lesions perpendicular to lateral ventricles (along medullary veins) on sagittal FLAIR — pathognomonic
- T1 "Black holes": Chronic plaques appear hypointense on T1 = irreversible axonal loss
- Post-Gd: Active plaques enhance (ring or nodular) = BBB breakdown during relapse
- Spinal cord: T2 hyperintense intramedullary lesion (usually <2 vertebral segments)
- McDonald Criteria 2017: Dissemination in space (DIS) + dissemination in time (DIT) on MRI
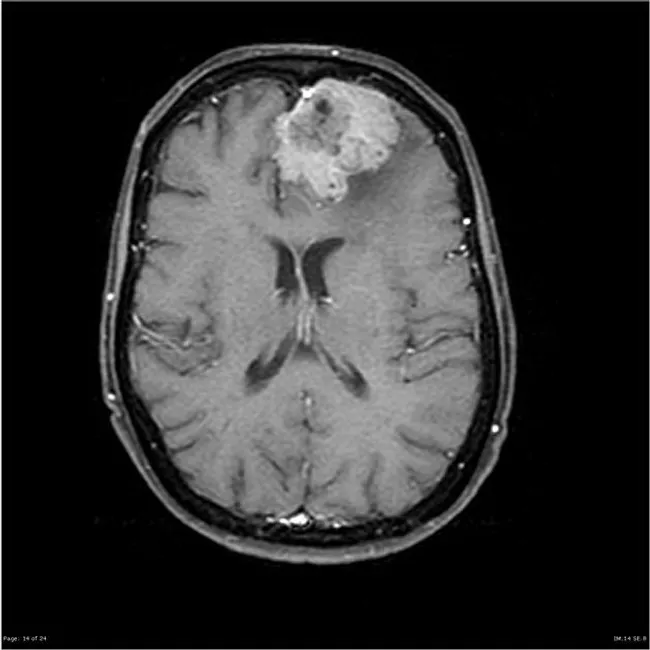
9.3 Glioblastoma (GBM) / High-Grade Glioma
- T2/FLAIR: Heterogeneous hyperintense mass + extensive surrounding vasogenic oedema
- T1 + Gd: Ring enhancement (irregular, thick rim) — active tumour margin; central necrotic dark core
- DWI: Restricted diffusion in solid components (high cellularity)
- MRS: ↑ Choline (cell membrane turnover), ↓ NAA (neuronal loss), lipid/lactate peaks (necrosis)
- Perfusion (DSC): Elevated rCBV in tumour (hyperperfusion)
- DTI: Corticospinal tract displacement — surgical planning
9.4 Brain Abscess
- T2/FLAIR: Hypointense rim (free radical-rich capsule) surrounded by hyperintense oedema
- T1 + Gd: Thin, smooth, regular ring enhancement — smooth inner wall (vs. GBM: thick, irregular)
- DWI: ↑ BRIGHT — restricted diffusion of pus (viscous fluid with restricted Brownian motion) — key differentiator from tumour
- ADC: ↓ dark — confirms true restriction
- MRS: Lactate, alanine, acetate, succinate, cytosolic amino acids — suggests pyogenic organisms
PG Exam Tip: Ring-enhancing lesion on MRI — if DWI bright = abscess; if DWI variable = tumour
9.5 Meningioma
- T1: Isointense to grey matter
- T2: Variable (iso- to hyperintense)
- Gd T1: Intense homogeneous enhancement + dural tail sign (enhancing dura extending from lesion)
- Extra-axial location (displaces brain, does not invade)
- Calcification: Hypointense on T2/SWI; may be visible as psammoma bodies
- Associated hyperostosis of adjacent bone
9.6 Pre-Surgical Brain Mapping (Advanced — Neurosurgery/Neurology PG)
- Maps eloquent cortex (motor, language — Broca's/Wernicke's, visual)
- Identifies critical white matter tracts (corticospinal tract, arcuate fasciculus)
- Allows safe surgical margins to minimise postoperative deficits
- Combined with MEG and intraoperative neuronavigation
SECTION 10 — MRI vs. CT — WHEN TO USE WHICH
| Situation | Preferred Modality | Reason |
|---|---|---|
| Acute trauma / head injury | CT | Speed, bone detail, haemorrhage detection |
| Acute stroke triage | CT first → MRI (DWI) | CT rules out bleed; DWI detects early ischaemia |
| Ischaemic stroke confirmation | MRI (DWI) | Visible within minutes |
| Posterior fossa lesion | MRI | No beam-hardening artefact |
| Seizures / epilepsy | MRI | Best hippocampal/cortical detail |
| Demyelination (MS) | MRI | FLAIR/T2 plaques, DIS/DIT for McDonald criteria |
| Tumour characterisation | MRI | Perfusion, spectroscopy, tractography, BBB status |
| Pituitary | MRI | No bone artefact; dynamic Gd protocol |
| Infection (abscess, encephalitis) | MRI | DWI, BBB integrity, enhancement pattern |
| Dementia workup | MRI | Atrophy patterns, vascular lesion load, hippocampal volumetry |
| Metallic implant / pacemaker | CT | MRI contraindicated in non-MR-conditional devices |
| Unstable patient | CT | MRI too slow, difficult monitoring |
| Pregnancy | MRI (avoid Gd) | No ionising radiation |
SECTION 11 — MRI ARTEFACTS
| Artefact | Cause | Appearance | Solution |
|---|---|---|---|
| Motion | Patient movement | Blurring, ghosting | Fast sequences, sedation, motion correction (PROPELLER/BLADE) |
| Pulsation | Arterial/CSF pulsatility | Ghosting in phase-encode direction | Cardiac gating, swap phase/frequency |
| Wrap-around (aliasing) | Body part outside FOV | Image wraps onto other side | ↑ FOV, ↑ phase-encode steps, oversampling |
| Chemical shift | Fat/water frequency difference | Dark/bright bands at fat-water interface | Fat suppression (STIR, Dixon) |
| Truncation (Gibbs ringing) | Undersampling at interfaces | Parallel bands at tissue edges | ↑ matrix size |
| Susceptibility (metal) | Metallic implants, surgical clips | Signal void + distortion | STIR, MARS sequences, titanium hardware |
| T2 shine-through | High T2 signal mimics DWI restriction | Bright DWI but bright ADC | Always confirm with ADC map |
SECTION 12 — RECENT UPDATES (2023–2025)
12.1 7 Tesla (7T) MRI — Clinical Approval
- FDA/CE approved for clinical neuroimaging (2017 FDA, expanding clinical use 2023–2025)
- Advantages: Ultra-high spatial resolution, improved cortical architecture, small lesion detection (hippocampal sclerosis, small MS lesions, cortical dysplasia)
- Limitations: Susceptibility artefacts, RF non-uniformity, limited body applications, higher cost, fewer contraindicated implants cleared
- Key use: Drug-resistant epilepsy, MS, dementia research, neurosurgical planning
12.2 AI-Accelerated MRI (Deep Learning Reconstruction)
- Compressed sensing + deep learning reduces scan time by 60–80% with maintained image quality
- FDA-cleared tools: Vendor-specific (e.g., GE AIR Recon DL, Siemens Deep Resolve, Philips SmartSpeed)
- Clinical impact: Paediatric brain MRI in <5 minutes; feasible in agitated patients
- Synthetic MRI: Single acquisition generates multiple contrast weightings simultaneously (T1, T2, PD, FLAIR, Myelin maps)
12.3 DWI-FLAIR Mismatch — Clinical Practice Update
- WAKE-UP Trial (NEJM 2018): Gd thrombolysis guided by DWI+/FLAIR− in unknown onset stroke → significantly better outcomes vs. placebo
- Now incorporated into 2023 ESO/AHA stroke guidelines for unknown-onset stroke
12.4 Gadolinium Deposition — Current Guidance
- Linear Gd agents (gadodiamide, gadopentetate) → higher brain deposition → several withdrawn/restricted in EU
- Macrocyclic agents (gadobutrol, gadoterate, gadoteridol) → significantly lower deposition → preferred for all repeated-dose applications
- 2023 ACR/ESR guidance: Use macrocyclic agents; record cumulative lifetime Gd dose; document clinical indication
12.5 Quantitative MRI (qMRI) — Emerging Standard
- T1/T2 mapping, myelin water imaging: Quantitative biomarkers replacing subjective visual assessment
- qMRI in MS: Myelin content tracking over time; treatment response monitoring
- Body/brain MRI vendors: Increasing integration of qMRI into clinical workflows
12.6 MR-guided Focused Ultrasound (MRgFUS)
- Combines MRI guidance with high-intensity focused ultrasound
- FDA-approved: Essential tremor, Parkinson's tremor (thalamotomy without surgery)
- Real-time thermal monitoring via MRI thermometry during treatment
12.7 Neuroradiological Updates — Brain Tumour (WHO 2021 Classification)
- Integrated molecular-MRI diagnosis: WHO 5th ed. (2021) requires IDH mutation status, MGMT methylation, 1p/19q codeletion for glioma grading
- MRI implications: Ring-enhancing T1 lesion alone is insufficient — biopsy/molecular profile mandatory for WHO grade
- Radiomics & AI: Machine-learning models can predict IDH status, MGMT methylation from standard MRI features with ~85% accuracy (research, not yet standard clinical practice)
SECTION 13 — QUICK REFERENCE — DIAGNOSIS AT A GLANCE
| Clinical Scenario | Key MRI Finding | Sequence to Look |
|---|---|---|
| Acute ischaemic stroke | DWI↑, ADC↓ | DWI + ADC |
| MS acute relapse | T2/FLAIR periventricular plaques, Gd-enhancing | FLAIR + Gd T1 |
| GBM | Irregular ring enhancement, central necrosis, oedema | Gd T1 + FLAIR |
| Brain abscess | DWI↑ (pus restriction), thin ring enhancement | DWI + Gd T1 |
| Subacute haemorrhage | T1 bright (methemoglobin) | T1W |
| Chronic haemorrhage / microbleed | T2*/SWI dark "blooming" | GRE/SWI |
| Meningioma | Extra-axial, homogeneous enhancement, dural tail | Gd T1 |
| SAH on MRI | FLAIR bright sulci (blood in CSF) | FLAIR |
| Herpes encephalitis | T2/FLAIR hyperintensity temporal lobes, DWI restriction | T2 + DWI |
| Epidermoid | DWI↑ (bright), T2 bright, non-enhancing | DWI |
| CNS lymphoma | Homogeneous enhancement, periventricular, DWI↑ | DWI + Gd T1 |
| Hippocampal sclerosis (epilepsy) | T2/FLAIR hyperintense small hippocampus | Coronal FLAIR + T2 |
SECTION 14 — PG EXAM HIGH-YIELD POINTS
- MRI uses NO ionising radiation — can be used in pregnancy (avoid Gd in 1st trimester)
- T1W: anatomy, anatomy, anatomy — bright fat/blood/Gd; T2W: pathology lights up
- FLAIR suppresses CSF → periventricular lesions (MS Dawson's fingers) become obvious
- DWI + ADC: Acute stroke detectable in minutes — DWI↑ + ADC↓ = true restriction
- DWI-FLAIR mismatch (DWI+ / FLAIR−) = stroke onset <4.5 h → thrombolysis window
- Abscess = DWI↑ (restricted pus); Tumour = variable DWI — key ED differentiator
- MS: Dawson's fingers (sagittal FLAIR) + black holes (T1) + Gd-enhancing = active disease
- Haemorrhage: Subacute = T1 bright (methemoglobin); Chronic = T2 black rim (haemosiderin)
- Gadolinium deposition → prefer macrocyclic agents; avoid in eGFR <30 (NSF risk)
- Posterior fossa: MRI is always preferred over CT (no beam-hardening artefact)
- 7T MRI now clinically approved — best for epilepsy, cortical dysplasia, small MS lesions
- WHO 2021 glioma classification requires molecular profile — MRI alone is insufficient for final grade
- MR-conditional devices — check www.mrisafety.com; never assume safety from appearance alone
- Macrocyclic Gd agents (gadobutrol, gadoterate) = safer for repeated exposure; preferred currently