Total PSA report level in blood
Reading File
Finding Sources
Searching PubMed
prostate specific antigen PSA screening guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information to give a thorough answer on total PSA levels in blood.
Total PSA (Prostate-Specific Antigen) in Blood
What is PSA?
PSA is a 33-kDa serine protease produced exclusively by prostatic epithelial cells. Its normal physiological role is to cleave and liquefy the seminal coagulum after ejaculation - it is secreted into prostatic alveoli and incorporated into seminal fluid. Because PSA is predominantly released into prostatic secretions, only a very small amount normally enters the bloodstream.
- Histology: A Text and Atlas (Mescher)
- Robbins & Cotran Pathologic Basis of Disease
Normal Reference Range
| Interpretation | Total PSA Level |
|---|---|
| Normal (healthy adult male) | < 4.0 ng/mL |
| Gray zone (suspicious) | 4.0 - 10.0 ng/mL |
| High suspicion for cancer | > 10.0 ng/mL |
At the standard cutoff of ≥ 4.0 ng/mL, PSA has a sensitivity of 68-80% and specificity of 60-70% for prostate cancer.
Age-Specific PSA Thresholds
Because the prostate naturally enlarges with age (raising PSA even without cancer), age-adjusted cutoffs improve diagnostic accuracy:
| Age Group | Upper Limit of Normal |
|---|---|
| 40 - 49 years | 2.5 ng/mL |
| 50 - 59 years | 3.5 ng/mL |
| 60 - 69 years | 4.5 ng/mL |
| 70 - 79 years | 6.5 ng/mL |
- Goldman-Cecil Medicine, 26th edition
PSA in Blood: Two Forms (Molecular Forms)
In serum, PSA circulates in two main forms:
| Form | % in Serum | Significance |
|---|---|---|
| Complexed PSA (bound to proteins, mainly α1-antichymotrypsin) | 60-95% | Higher in prostate cancer |
| Free PSA (unbound) | 5-40% | Lower % in prostate cancer |
A low free PSA fraction (or high bound fraction) correlates with prostate cancer. When total PSA is 4-10 ng/mL, a free PSA < 25% can detect 95% of cancers while avoiding ~20% of unnecessary biopsies.
- Quick Compendium of Clinical Pathology, 5th ed.
- Campbell-Walsh-Wein Urology
Causes of Elevated PSA (False Positives)
PSA is organ-specific, but NOT cancer-specific. Elevated PSA can occur with:
- Prostate cancer - most important cause
- Benign prostatic hyperplasia (BPH) - very common; causes overlap with cancer levels
- Prostatitis (acute and chronic) - can cause variable elevations
- Prostate infarction (in setting of BPH)
- Digital rectal examination (DRE) - small, transient elevation
- Prostate needle biopsy - spike lasting 4+ weeks before returning to baseline
- Ejaculation (within 24 hours, especially in men ≥ 50 years) - returns to baseline within 24 hours
- Long-distance cycling (>55 km rides) - ~10% elevation
- 5α-reductase inhibitors (finasteride, dutasteride) - reduce PSA by ~50% after 12 months; apply "doubling rule" to interpret results
- Campbell-Walsh-Wein Urology
Predictive Value by PSA Level
| PSA Level | Risk of Prostate Cancer |
|---|---|
| ≤ 0.5 ng/mL | 6.6% (12% high-grade) |
| 0.6 - 1.0 ng/mL | 10% |
| 1.1 - 2.0 ng/mL | 17% |
| 2.1 - 3.0 ng/mL | 24% (19% high-grade) |
| 4 - 10 ng/mL | ~25% (PPV) |
| > 10 ng/mL | 42-64% (PPV) |
Key point: There is NO PSA level that completely rules out prostate cancer.
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed.
Adjunctive PSA Indices
When total PSA alone is ambiguous, these derived indices add diagnostic value:
| Index | Definition | Use |
|---|---|---|
| Free PSA % | Free PSA / Total PSA × 100 | <25% favors cancer |
| PSA Density (PSAD) | Total PSA ÷ prostate volume (mL) | >0.09 ng/mL/cc raises cancer suspicion |
| PSA Velocity | Rate of PSA change over time | Rapid rise is suspicious |
| Age-adjusted PSA | Reference range adjusted by age | Better sensitivity in young, specificity in old |
Screening Recommendations (Current Guidelines)
- AUA/SUO 2023: Shared decision-making for men ages 55-69 years; routine screening not recommended for men ≥ 70 years
- USPSTF: Men ages 55-69 years should be informed of potential benefits and harms before screening
- EAU 2024 Guidelines (PMID: 38614820): Recommend risk-adapted screening; baseline PSA at age 45-50 is useful for risk stratification
Screening programs in men aged 55-69 years prevent approximately 1.3 deaths from prostate cancer and 3 cases of metastatic disease per 1,000 men screened over ~13 years.
Clinical Utility Summary
| Clinical Purpose | PSA Role |
|---|---|
| Early cancer detection | Screening test (imperfect sensitivity/specificity) |
| Monitoring after treatment | High value - rising PSA after surgery/radiation signals recurrence |
| Staging | Higher PSA correlates with more advanced disease |
| Treatment response | PSA nadir after therapy predicts outcome |
Note: PSA is best used as part of a multi-modal assessment including DRE, imaging (MRI preferred over ultrasound for biopsy guidance), and clinical risk factors - not as a standalone test.
High level alpha feto protein means
Finding Sources
Searching PubMed
alpha-fetoprotein AFP tumor marker clinical significance
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Excellent - I now have comprehensive data from multiple authoritative textbooks. Here is the complete answer:
High Alpha-Fetoprotein (AFP): What It Means
What is AFP?
AFP (alpha-fetoprotein) is a major fetal serum glycoprotein - structurally similar to albumin - synthesized during fetal life by:
- Yolk sac (primary early source)
- Fetal liver hepatocytes
- Fetal gastrointestinal tract and kidneys (minor contribution)
It is one of the most important oncofetal antigens in clinical medicine. After birth, AFP rapidly drops to nearly undetectable levels in healthy adults.
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Quick Compendium of Clinical Pathology, 5th ed.
Normal Reference Values
| Population | AFP Level |
|---|---|
| Healthy adults | < 5.4 - 8.4 ng/mL |
| Normal pregnancy | Usually < 100 ng/mL |
| Benign disease (max) | Never exceeds ~500 ng/mL |
| HCC / yolk sac tumor | Can reach thousands to >10,000 ng/mL |
A value > 500 ng/mL is virtually never benign - it strongly indicates malignancy.
Causes of Elevated AFP
1. Malignant Causes (Most Important)
| Cancer | AFP Significance |
|---|---|
| Hepatocellular carcinoma (HCC) | Elevated in ~70-90% of cases; most common use. Combined with ultrasound for surveillance in high-risk patients (chronic HBV/HCV, cirrhosis) |
| Yolk sac tumor (endodermal sinus tumor) | Highly elevated; magnitude correlates with prognosis - AFP > 10,000 ng/mL = poor prognosis |
| Embryonal carcinoma (testis/ovary) | Elevated; part of NSGCT (non-seminomatous germ cell tumor) |
| Mixed germ cell tumors (with yolk sac component) | Elevated in 50-70% of low-stage NSGCT; 60-80% in advanced NSGCT |
| Hepatoblastoma | Elevated in ~90% of cases; used for monitoring tumor response and recurrence |
| Gastric carcinoma (hepatoid variant) | Sporadic elevation |
| Cancers of stomach, pancreas, biliary tract, lung | Occasional elevation |
Key point: Pure seminoma and choriocarcinoma do NOT produce AFP. If AFP is elevated in a patient with apparent pure seminoma, the tumor must be reclassified as NSGCT.
- Schwartz's Principles of Surgery, 11th ed.
- Campbell-Walsh-Wein Urology
- Quick Compendium of Clinical Pathology, 5th ed.
2. Benign (Non-Malignant) Causes
| Condition | Notes |
|---|---|
| Cirrhosis | Common cause; values usually < 500 ng/mL |
| Acute hepatitis | Transient elevation |
| Chronic active hepatitis | Can be persistently mildly elevated |
| Hepatic necrosis | Cellular damage releases AFP |
| Ataxia-telangiectasia | Genetic disorder with persistently elevated AFP |
| Wiskott-Aldrich syndrome | Immunodeficiency with AFP elevation |
| Hereditary tyrosinemia | Metabolic disease with hepatic involvement |
| Pregnancy | Normal physiological elevation (< 100 ng/mL) |
3. AFP in Pregnancy (Obstetric Context)
Maternal serum AFP (MSAFP) is used as a prenatal screening test:
| Maternal AFP | Fetal Implication |
|---|---|
| HIGH AFP (≥ 2.0-2.5 MoM) | Open neural tube defect (spina bifida, anencephaly) - elevated in 85-95% of cases. Also: abdominal wall defects (gastroschisis, omphalocele), fetal death, twin pregnancy (~2x normal), placental abnormalities |
| LOW AFP | Down syndrome (Trisomy 21) - low in ~30% of cases (part of triple/quad screen with hCG, uE3, inhibin-A) |
- Tietz Textbook of Laboratory Medicine, 7th ed.
- The Developing Human: Clinically Oriented Embryology
AFP Half-Life and Clinical Monitoring
- AFP has a half-life of 5-7 days
- After surgical resection of HCC or a germ cell tumor, AFP should fall steadily - a persistently elevated or rising AFP after treatment signals residual or recurrent disease
- In testicular NSGCT, AFP is measured at diagnosis, post-orchiectomy, during chemotherapy, and for long-term surveillance
AFP Levels Summarized by Level
| AFP Level | Clinical Interpretation |
|---|---|
| < 10 ng/mL | Normal adult |
| 10-100 ng/mL | Benign liver disease, pregnancy, mild hepatitis |
| 100-500 ng/mL | Cirrhosis, chronic liver disease (benign possible) |
| > 500 ng/mL | Strongly suggests malignancy |
| > 400 ng/mL + liver mass | Diagnostic of HCC (no biopsy needed per many guidelines) |
| > 10,000 ng/mL | Associated with poor prognosis in yolk sac tumors |
In Short
A high AFP means:
- In a non-pregnant adult - investigate for HCC (especially with liver disease/cirrhosis) or germ cell tumor (testis/ovary)
- In a pregnant woman - elevated MSAFP signals open neural tube defect in the fetus
- After cancer treatment - a rising AFP signals recurrence
- Benign causes are possible but AFP > 500 ng/mL essentially rules them out
cholangiocarcinoma
Finding Sources
Searching PubMed
cholangiocarcinoma diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Now I have comprehensive data from multiple authoritative textbooks including pathology images and classification diagrams. Here is the full answer:
Cholangiocarcinoma (CCA)
Definition
Cholangiocarcinoma is a malignant epithelial carcinoma arising from cholangiocytes (bile duct epithelium) anywhere along the intrahepatic or extrahepatic biliary tree. It is the most common bile duct tumor and the second most common primary liver malignancy after hepatocellular carcinoma (HCC).
- Robbins & Kumar Basic Pathology
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Classification by Location
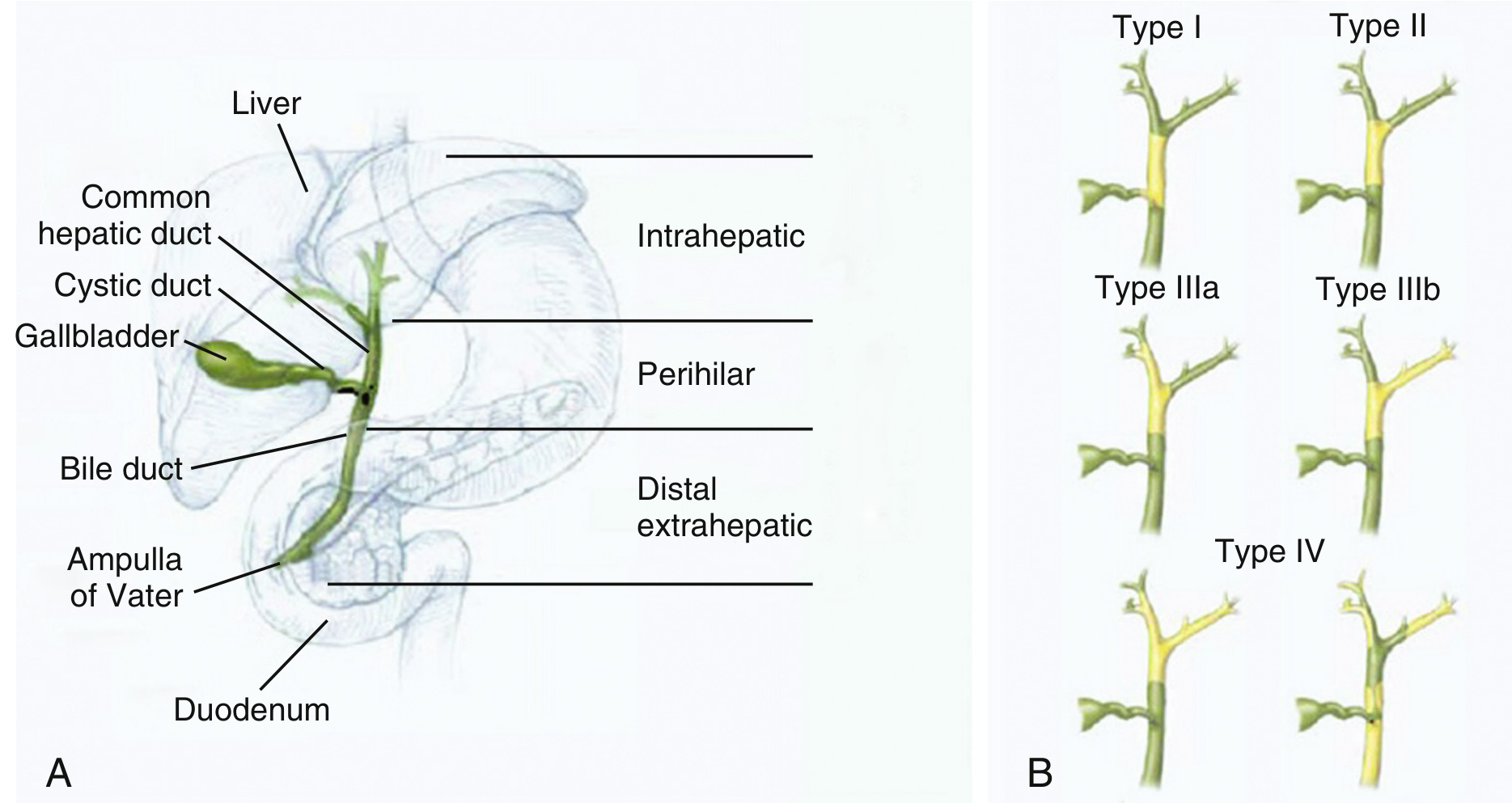
Fig: Anatomic classification (left) and Bismuth-Corlette classification of perihilar CCA (right) - Sleisenger & Fordtran
| Type | Location | Frequency |
|---|---|---|
| Perihilar (Klatskin tumor) | Between 2nd-order ducts and cystic duct insertion (biliary confluence) | 50-60% (most common) |
| Distal extrahepatic | Below cystic duct insertion, in the common bile duct posterior to duodenum | 20-30% |
| Intrahepatic | Within liver parenchyma, above 2nd-order bile ducts | ~10-20% |
Bismuth-Corlette Classification (Perihilar CCA)
| Type | Extent |
|---|---|
| Type I | Common hepatic duct, distal to confluence |
| Type II | Involves the right-left hepatic duct union |
| Type IIIa | Extends up the right hepatic duct |
| Type IIIb | Extends up the left hepatic duct |
| Type IV | Multifocal / involves confluence + both hepatic ducts |
Epidemiology
- Second most common primary liver cancer globally
- Accounts for < 2% of all cancers, but 10-20% of hepatobiliary cancer deaths
- Highest incidence: Southeast Asia (Thailand, Laos, Cambodia) - up to 113/100,000 due to liver fluke infestation
- Western nations: Typically diagnosed > 65 years; rare before age 40 (except in PSC patients)
- Male > female; higher rates in Asian and Hispanic populations in the US
- Incidence of intrahepatic CCA is rising worldwide since the 1980s
Risk Factors
All risk factors share a common mechanism: chronic biliary inflammation and cholestasis promoting somatic mutations in cholangiocytes.
| Risk Factor | Notes |
|---|---|
| Liver flukes (Opisthorchis viverrini, Clonorchis sinensis) | Major cause in Southeast Asia |
| Primary sclerosing cholangitis (PSC) | Lifetime risk 5-20%; leading cause of PSC-related death |
| Hepatolithiasis (intrahepatic gallstones) | Chronic bile stasis + inflammation |
| Hepatitis B and C | Elevated rates as with HCC |
| NAFLD/NASH | Emerging risk factor |
| Fibropolycystic liver disease | Caroli disease, choledochal cysts |
| Inflammatory bowel disease (especially UC with PSC) | Compound risk |
| Alcohol, smoking, diabetes, HIV | Additional risk modifiers in PSC-CCA |
Pathology
Gross Morphology
- Extrahepatic CCA: Usually small at diagnosis (cause early biliary obstruction); firm, gray nodules within duct wall or diffusely infiltrative
- Intrahepatic CCA: May be a single large mass or track along portal tracts; occurs in non-cirrhotic livers
Histology
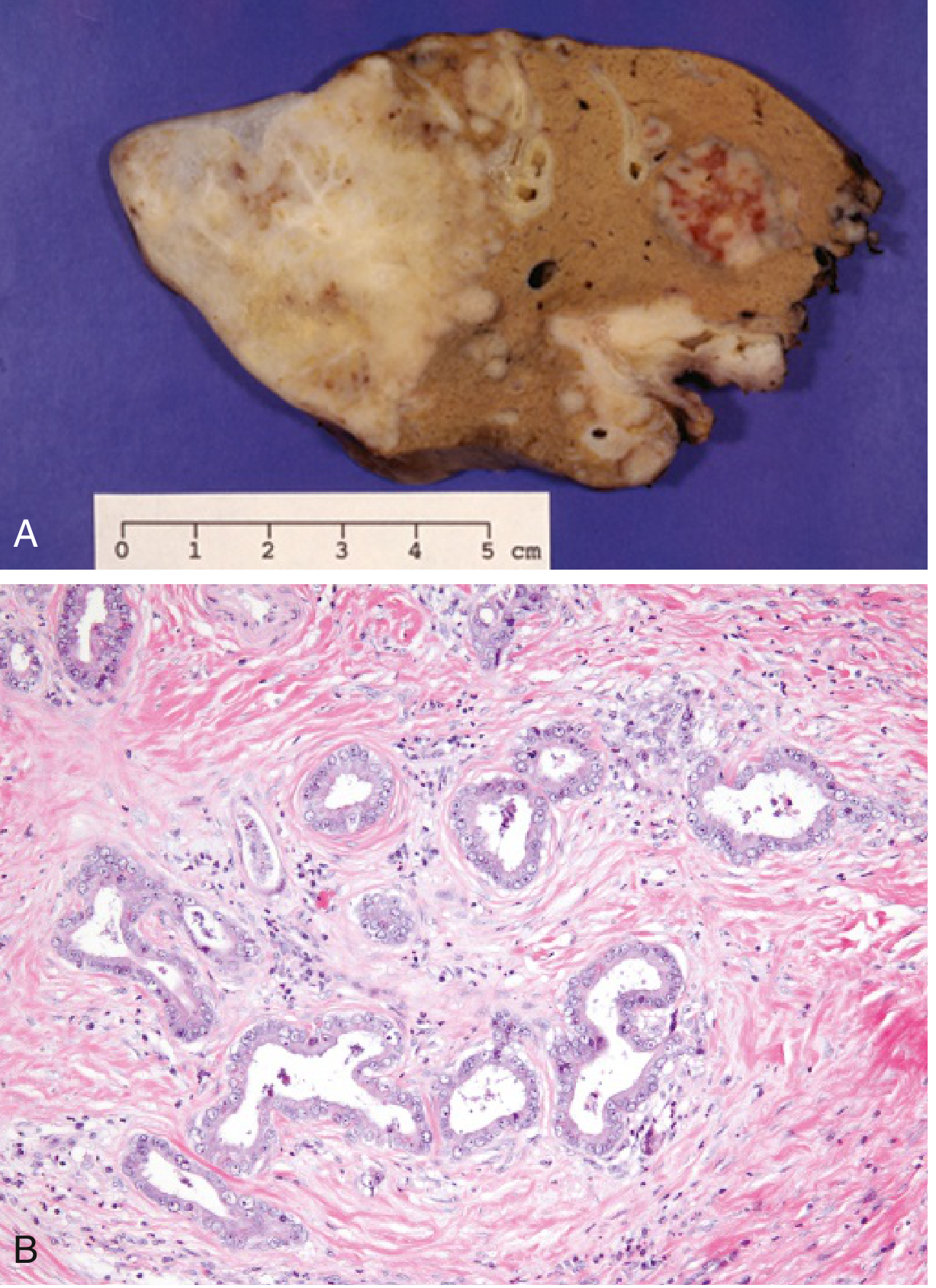
Fig: (A) Multifocal cholangiocarcinoma from patient with Clonorchis sinensis infestation. (B) Invasive malignant glands in reactive sclerotic desmoplastic stroma - Robbins & Kumar
- Mucin-producing adenocarcinoma - most are well to moderately differentiated
- Grow as glandular or tubular structures lined by malignant epithelial cells
- Marked desmoplasia (dense fibrous stroma) - characteristic feature
- Lymphovascular invasion and perineural invasion are common → extensive metastases
Clinical Presentation
| Type | Symptoms |
|---|---|
| Perihilar / Distal CCA | Obstructive jaundice (painless), pruritus, acholic stools, dark urine, weight loss, abdominal pain |
| Intrahepatic CCA | Nonspecific symptoms until late (abdominal discomfort, weight loss); often found incidentally on imaging |
Suspect CCA in a PSC patient who develops: worsening jaundice, unexplained weight loss, or new dominant stricture.
Tumor Markers
| Marker | Role | Performance |
|---|---|---|
| CA 19-9 | Most useful; >100 U/L in PSC patients | Sensitivity 52-89%, specificity 76-86% |
| CEA | Adjunct marker | Lower sensitivity |
| AFP | Used to differentiate from HCC (AFP elevated in HCC, not CCA) | - |
| IgG4 | Rule out IgG4-associated cholangitis (mimics CCA) | Important exclusion |
CA 19-9 alone is insufficient - up to one third of patients with elevated CA 19-9 do not have CCA.
Diagnosis and Imaging
Intrahepatic CCA
- CT / MRI with contrast: Rim or peripheral arterial enhancement with progressive centripetal enhancement in delayed phases (opposite of HCC, which shows washout)
- PET/CT: Sensitivity 95%, specificity 83% for intrahepatic CCA
- Tissue biopsy only needed for unresectable disease; if resectable, proceed to surgery without biopsy
Perihilar / Distal CCA
- MRCP: Best for defining proximal extent of biliary invasion and tumor-vessel relationships
- CT: Superior for vascular involvement and resectability assessment (accuracy 60-88%)
- ERCP / Percutaneous THC: Provides cholangiography + cytological brushing + biliary drainage
- Cytology brushing: specificity 90-100% but sensitivity only 4-20%
- FISH (fluorescence in situ hybridization) combined with cytology improves sensitivity to 35-60%
Molecular Pathways and Targeted Therapy
More than 40% of CCAs carry actionable genetic alterations.
| Alteration | Targeted Drug |
|---|---|
| FGFR2 fusions (~15% intrahepatic CCA) | Pemigatinib (FDA-approved) |
| IDH1 mutations (~20% intrahepatic CCA) | Ivosidenib (FDA-approved) |
| MSI-High / dMMR / TMB-High | Pembrolizumab (1st or subsequent line) |
| NTRK fusions | Entrectinib, larotrectinib |
| BRAF V600E mutations | Dabrafenib + trametinib |
| Poor prognosis markers | HER2 amplification, ARID1A, TP53, KRAS mutations |
Key pathways implicated: IL-6/STAT3, TGF-β/SMAD, EGFR, Notch, Wnt/β-catenin.
Treatment
| Setting | Treatment |
|---|---|
| Resectable localized disease | Surgical resection with negative margins (R0) - only potentially curative option |
| Intrahepatic CCA, unresectable | Biopsy → systemic therapy ± locoregional therapy |
| Perihilar CCA with cirrhosis | Liver transplantation (selected cases, protocol-based) |
| Unresectable / metastatic | Gemcitabine + cisplatin (standard 1st line) ± immunotherapy; targeted agents per molecular profile |
| Biliary obstruction | Biliary stenting (ERCP or percutaneous) for palliation |
Prognosis
- Extremely poor regardless of subtype
- Extrahepatic CCA: ~15% survival at 2 years after diagnosis
- Intrahepatic CCA: median survival 6 months from diagnosis even after surgical treatment
- Most patients present at an advanced, unresectable stage
- Natural course: median survival < 24 months after diagnosis
- PSC-associated CCA: Leading cause of death in PSC patients since liver transplantation became available
Recent Guidelines (2023-2025)
This is a shared conversation. Sign in to Orris to start your own chat.