Evaluation of renal functions in ER
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
acute kidney injury emergency department evaluation biomarkers
Loading Image
Reading File
I now have everything needed for a comprehensive, well-structured answer. Let me compile it.
Evaluation of Renal Function in the Emergency Room
The emergency assessment of renal function aims to detect acute kidney injury (AKI), differentiate its cause (prerenal, intrinsic, postrenal), gauge severity, and guide management — all rapidly and with the tools available at the bedside.
1. Clinical History & Physical Examination
Before ordering any tests, a focused history is essential:
- Precipitating events: volume loss (vomiting, diarrhea, hemorrhage), surgery, sepsis, trauma, rhabdomyolysis
- Nephrotoxin exposure: NSAIDs, ACE inhibitors/ARBs, aminoglycosides, IV contrast, vancomycin, cisplatin, statins (rhabdomyolysis)
- Obstructive symptoms: urinary hesitancy, nocturia, pelvic/flank pain, overflow incontinence, known malignancy
- Systemic illness: heart failure, cirrhosis, diabetes, hypertension, autoimmune disease
Physical examination may reveal:
- Reduced body weight, orthostatic hypotension, tachycardia, absent JVD → volume depletion (prerenal)
- Pulmonary/peripheral edema → volume overload (may still be prerenal in heart failure/cirrhosis)
- Myoclonus, asterixis, pericardial friction rub → advanced uremia
- Rash, arthritis, sinusitis → systemic vasculitis or glomerulonephritis
— Comprehensive Clinical Nephrology, 7th Ed.
2. Diagnostic Criteria for AKI (KDIGO)
AKI is defined by any of the following:
- Rise in serum creatinine ≥ 0.3 mg/dL within 48 hours
- Rise in serum creatinine to ≥ 1.5× baseline within 7 days
- Urine output < 0.5 mL/kg/hr for ≥ 6 hours
A single elevated creatinine cannot accurately measure functional loss without knowing baseline, as it lacks kinetic properties at non-steady state. It is also influenced by muscle mass, nutritional status, and drugs (cimetidine, trimethoprim, salicylates) that block tubular transport of creatinine. — Goldman-Cecil Medicine
3. Laboratory Tests
A. Serum Chemistry Panel
| Test | Normal | Clinical Relevance |
|---|---|---|
| Serum Creatinine (SCr) | 0.6–1.2 mg/dL (M); 0.5–1.1 (F) | Primary marker; rises lag behind actual injury by hours |
| Blood Urea Nitrogen (BUN) | 5–20 mg/dL | Affected by protein intake, GI bleeding, catabolic state; non-specific alone |
| BUN:Creatinine ratio | ~10–15:1 | > 20:1 suggests prerenal (enhanced urea reabsorption) or upper GI bleed; < 10:1 suggests intrinsic renal disease or low protein intake |
| Electrolytes (Na, K, Cl, HCO₃) | — | Hyperkalemia and metabolic acidosis suggest significant renal impairment or rhabdomyolysis |
| Calcium, Phosphorus | — | Hypocalcemia + hyperphosphatemia in acute tubular necrosis; tumor lysis syndrome |
| CBC with differential | — | Schistocytes → TMA/HUS; eosinophilia → AIN |
| Serum uric acid | — | Elevated in tumor lysis syndrome |
All patients with acutely elevated SCr should have serum electrolytes, calcium, phosphorus, BUN, and CBC. — Goldman-Cecil Medicine
B. Estimated GFR (eGFR)
Calculated from SCr using the CKD-EPI or MDRD equation incorporating age, sex, and race. In the ER, eGFR helps stage the degree of renal impairment but has limitations in rapidly changing SCr (non-steady state), extremes of muscle mass, and the elderly.
4. Urinalysis & Urine Microscopy
A cornerstone of ER renal evaluation. A fresh urine sample is centrifuged and sediment examined.
Dipstick Urinalysis
- Protein: present in glomerulonephritis, nephrotic syndrome, myeloma (note: dipstick misses immunoglobulin free light chains; alkaline or contrast-containing urine → false positive)
- Blood: hematuria → glomerulonephritis, vascular disease, stones; myoglobinuria (rhabdomyolysis) → positive dipstick but no RBCs on microscopy
- Leukocyte esterase/nitrites: infection, AIN
- Glucose: renal tubular dysfunction (Fanconi syndrome), or just hyperglycemia
Urine Microscopy Findings in AKI
| Cause of AKI | Urinalysis / Sediment |
|---|---|
| Prerenal | Normal or hyaline casts only |
| Acute tubular necrosis (ATN) | "Muddy brown" granular casts, renal tubular epithelial (RTE) cells — >10 granular casts/LPF has 100% PPV for ATN |
| Acute interstitial nephritis (AIN) | WBCs in clumps and casts (no bacteria); rarely eosinophiluria |
| Glomerulonephritis | RBC casts, dysmorphic RBCs, proteinuria |
| Obstructive / Postrenal | Normal, or RBCs/WBCs; broad waxy casts if chronic |
| Tumor lysis syndrome | Uric acid crystals + hyperphosphatemia |
| Myeloma | Positive for protein on sulfosalicylic acid test, negative dipstick |
— Comprehensive Clinical Nephrology, 7th Ed.; Goldman-Cecil Medicine
5. Urine Chemistry Tests
Urine Sodium (UNa)
- < 20 mEq/L: tubules actively conserving sodium → prerenal
- > 40 mEq/L: tubular dysfunction → ATN
Fractional Excretion of Sodium (FENa)
$$\text{FENa} = \frac{U_{Na} \times P_{Cr}}{P_{Na} \times U_{Cr}} \times 100$$
| FENa | Interpretation |
|---|---|
| < 1% | Prerenal AKI (tubules intact, avidly reabsorbing Na) |
| > 3% | ATN (tubular damage, inability to reabsorb Na) |
| 1–3% | Indeterminate |
Limitations of FENa: Can be < 1% despite ATN in sepsis, myoglobinuria, hemoglobinuria, IV contrast nephropathy, heart failure, cirrhosis. Can be > 1% despite prerenal if the patient is on diuretics, has glycosuria, bicarbonaturia, or CKD.
Fractional Excretion of Urea (FEUrea)
Preferred when the patient is on diuretics (urea reabsorption is less affected by loop diuretics):
$$\text{FEUrea} = \frac{U_{Urea} \times P_{Cr}}{P_{Urea} \times U_{Cr}} \times 100$$
- < 35% → Prerenal AKI
- > 50% → ATN
Urine Osmolality
- > 500 mOsm/kg: concentrating ability preserved → prerenal
- < 350 mOsm/kg: isosthenuria → tubular dysfunction (ATN)
6. Urine Output Monitoring
| Pattern | Volume | Significance |
|---|---|---|
| Normal | > 0.5 mL/kg/hr | — |
| Oliguric AKI | < 500 mL/day | Worse prognosis; seen in ATN, prerenal, AIN |
| Non-oliguric AKI | > 500 mL/day | Better prognosis but SCr still rises |
| Anuria | < 100 mL/day | Complete obstruction, bilateral vascular catastrophe, cortical necrosis, anti-GBM disease |
| Wide daily variation | Variable | Suggests intermittent obstruction |
— Comprehensive Clinical Nephrology, 7th Ed.
7. Novel Biomarkers of AKI
These detect tubular injury earlier than SCr (which rises only after ~50% nephron loss):
| Biomarker | Source | Significance |
|---|---|---|
| NGAL (Neutrophil Gelatinase-Associated Lipocalin) | Distal nephron, loop of Henle | Rises within 2 hours of ischemic or nephrotoxic injury; measurable in urine and serum |
| KIM-1 (Kidney Injury Molecule-1) | Proximal tubule | Highly specific for ischemic/nephrotoxic ATN |
| IL-18 | Proximal tubule | Elevated in ischemic ATN; not in prerenal or UTI |
| FABP (Fatty Acid-Binding Protein) | Proximal tubule | Marker of tubular ischemia |
| Cystatin C | All nucleated cells (filtered freely) | Earlier indicator of GFR decline than creatinine; not affected by muscle mass |
— Henry's Clinical Diagnosis and Management by Laboratory Methods
8. Imaging
Renal Ultrasound (First-Line Imaging)
- Mandated early to exclude postrenal obstruction (hydronephrosis, dilated collecting system)
- Assesses kidney size: small bilateral kidneys → CKD; normal or enlarged → favor acute
- Echogenicity: increased → chronic parenchymal disease
- Doppler: evaluates renal artery/vein patency (renal vein thrombosis, renal artery stenosis)
- Normal ultrasound does not exclude early/subacute obstruction
Other Imaging
- CT urogram/KUB: calculi, anatomic obstruction
- CT angiography/MRA: renal artery stenosis, bilateral renal vein thrombosis
- Renal scan (DTPA/MAG-3): assesses differential function and perfusion when anatomy is equivocal
9. Fluid Challenge Test
In suspected prerenal AKI with oliguria:
- Administer 100 mL IV bolus rapidly (1 min) or 3–4 mL/kg over 5 min
- Response (↑ urine output, ↓ SCr) confirms prerenal mechanism → continue resuscitation
- No response suggests intrinsic renal injury; further fluid loading risks harm
For distinguishing residual tubular function in established AKI:
- Furosemide 1–1.5 mg/kg IV: urine output > 100 mL/hr within 1 hour suggests preserved tubular function and predicts better outcome. — Goldman-Cecil Medicine
10. Classification of AKI and Laboratory Differentiation
| Feature | Prerenal | Intrinsic (ATN) | Postrenal |
|---|---|---|---|
| BUN:Cr ratio | > 20:1 | ~10–15:1 | Variable |
| FENa | < 1% | > 3% | Variable |
| FEUrea | < 35% | > 50% | Variable |
| Urine osmolality | > 500 mOsm/kg | < 350 mOsm/kg | Variable |
| Urine Na | < 20 mEq/L | > 40 mEq/L | Variable |
| Urinary sediment | Hyaline casts | Muddy brown casts, RTEs | Normal/RBCs |
| Response to fluids | Yes | No | No (unless relieved) |
| Ultrasound | Normal | Normal (or enlarged) | Hydronephrosis |
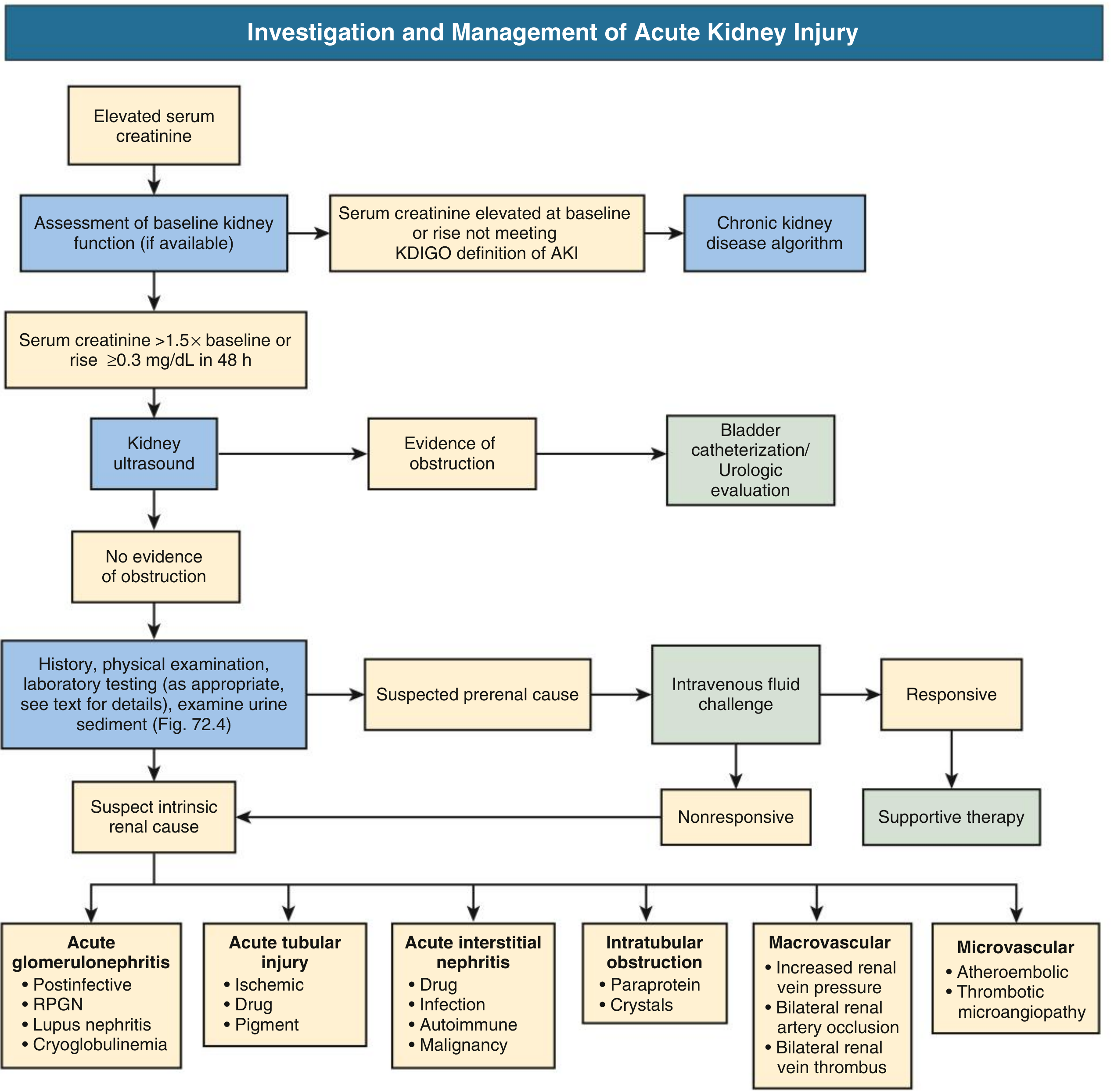
AKI Investigation Algorithm
11. Additional Tests for Systemic Causes
When systemic etiology is suspected:
| Condition | Tests |
|---|---|
| Glomerulonephritis | ANA, anti-dsDNA, ANCA (c/p), anti-GBM, complement C3/C4, ASO titre, cryoglobulins |
| Multiple myeloma | SPEP, UPEP, serum free light chains, bone marrow biopsy |
| Thrombotic microangiopathy (HUS/TTP) | Blood film (schistocytes), ADAMTS13, LDH, haptoglobin |
| Rhabdomyolysis | CK, myoglobin (serum/urine), urine dipstick positive without RBCs on microscopy |
| Tumor lysis syndrome | Uric acid, phosphorus, LDH, urine uric acid crystals |
| Infective endocarditis | Blood cultures, echocardiogram |
| Hepatorenal syndrome | LFTs, albumin, ascites evaluation |
Key Takeaways for the ER Clinician
- Establish baseline creatinine — the most critical first step to define AKI vs. CKD
- Urine output monitoring begins immediately; foley catheter if oliguric
- The diagnostic triad: serum chemistries + urinalysis/microscopy + renal ultrasound covers > 95% of ER AKI diagnoses
- FENa is useful but imperfect — always interpret in clinical context (diuretic use, sepsis)
- Novel biomarkers (NGAL, KIM-1) detect injury earlier but are not yet standard-of-care in most ERs
- Early ultrasound is mandatory to exclude obstruction before attributing AKI to intrinsic causes
- Prerenal AKI is the most common cause (30–60%) and may resolve with IV fluid resuscitation
Sources: Comprehensive Clinical Nephrology 7th Ed. · Goldman-Cecil Medicine · Brenner and Rector's The Kidney · Henry's Clinical Diagnosis and Management by Laboratory Methods · Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.