131 pneumonia and 132 lung abscess , make mini chapter but in detailed and conceptual base, dont skip any topic and content , add drug dosages , images, columns , all the relevent content on basis of harrison internal medicine , add related image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
I now have all the material I need from Harrison's 22E to write a comprehensive mini-chapter. Let me compose the full detailed chapter now.
Chapter 131 & 132 — Pneumonia and Lung Abscess
Based on Harrison's Principles of Internal Medicine, 22nd Edition (2025)
CHAPTER 131: PNEUMONIA
Definition
Pneumonia is an infection of the pulmonary parenchyma. Despite its significant morbidity and mortality, it is frequently misdiagnosed, mistreated, and underestimated. Classically, pneumonia is divided into:
| Category | Definition |
|---|---|
| Community-Acquired Pneumonia (CAP) | Acquired outside hospital or within 48 h of admission |
| Hospital-Acquired Pneumonia (HAP) | Onset ≥48 h after hospital admission, not incubating at admission |
| Ventilator-Associated Pneumonia (VAP) | Onset ≥48 h after endotracheal intubation |
| Discontinued - did not reliably predict resistant pathogens; led to overuse of broad-spectrum antibiotics |
Aspiration pneumonia accounts for 5-15% of CAP cases. It is best considered a point on the CAP-HAP continuum, involving the airways/parenchyma in patients with macroaspiration risk factors and characteristic anatomic involvement (posterior segments of upper lobes, superior segments of lower lobes).
Pathophysiology
The classic view held that lungs are sterile and pneumonia results from pathogens invading this sterile space. This has been revised.
The Lung Microbiota Model
The lungs harbor a complex, dynamic bacterial community (the lung microbiota). Pneumonia is not simply a "sterile space invaded by a pathogen" - it is an emergent phenomenon driven by:
- Microbial entry - via inhalation, microaspiration, or direct mucosal dispersion
- Microbial elimination - mucociliary clearance, cough, immune cells
- Regional growth conditions - pH, O₂ tension, temperature, nutrient availability
Pathogenic Loop
An inflammatory event causes epithelial/endothelial injury → releases cytokines, chemokines, catecholamines → selectively promotes growth of certain bacteria (e.g., S. pneumoniae, P. aeruginosa) → positive feedback loop → accelerated inflammation + bacterial dominance → full pneumonia syndrome.
Inflammatory mediators:
- IL-6, TNF → fever
- IL-8, G-CSF → increased local neutrophil recruitment
- Macrophage/neutrophil mediators → alveolar damage, altered permeability → hypoxemia, consolidation
Etiology of CAP
| Pathogen | Notes |
|---|---|
| Streptococcus pneumoniae | Most common overall; causes lobar/segmental pneumonia |
| Mycoplasma pneumoniae | Atypical; young adults; macrolide resistance increasing |
| Haemophilus influenzae | COPD patients; smokers |
| Legionella pneumophila | Water sources; severe CAP; requires urinary antigen test |
| Staphylococcus aureus | Post-influenza; MRSA possible; cavitary lesions |
| Chlamydophila pneumoniae | Atypical; mild disease |
| Respiratory viruses | Influenza A/B, SARS-CoV-2, RSV, adenovirus |
| Pseudomonas aeruginosa | Structural lung disease (bronchiectasis, severe COPD) |
| Gram-negative bacilli (Enterobacteriaceae) | Nursing home patients, recent hospitalization |
Site of Care Decision
CURB-65 Score
| Variable | Points |
|---|---|
| C - Confusion (new) | 1 |
| U - Urea >7 mmol/L (BUN >19 mg/dL) | 1 |
| R - Respiratory rate ≥30/min | 1 |
| B - Blood pressure: systolic ≤90 or diastolic ≤60 mmHg | 1 |
| 65 - Age ≥65 years | 1 |
| Score | 30-day Mortality | Recommendation |
|---|---|---|
| 0 | 1.5% | Outpatient |
| 1-2 | ~9% | Inpatient (consider outpatient if only age ≥65) |
| ≥3 | ~22% | Inpatient; consider ICU |
Pneumonia Severity Index (PSI)
Points given for 20 variables (age, comorbidities, abnormal labs/vitals). Assigns to 5 classes:
| Class | Mortality | Disposition |
|---|---|---|
| I | 0.1% | Outpatient |
| II | 0.6% | Outpatient |
| III | 2.8% | Outpatient or short observation |
| IV | 8.2% | Inpatient |
| V | 29.2% | Inpatient (ICU likely) |
PSI is more robustly validated but harder to calculate than CURB-65.
ICU Admission Criteria (ATS/IDSA Major + Minor)
Major criteria (direct ICU):
- Septic shock requiring vasopressors
- Acute respiratory failure requiring intubation/mechanical ventilation
Minor criteria (≥3 = ICU or high-level monitoring):
| Minor Criteria |
|---|
| Respiratory rate ≥30 breaths/min |
| PaO₂/FiO₂ ratio ≤250 |
| Multilobar infiltrates |
| Confusion/disorientation |
| Uremia (BUN ≥20 mg/dL) |
| Leukopenia (WBC <4000 cells/μL) |
| Thrombocytopenia (platelet count <100,000 cells/μL) |
| Hypothermia (core temp <36°C) |
| Hypotension requiring aggressive fluid resuscitation |
Antibiotic Resistance
S. pneumoniae Resistance Mechanisms
- Resistance to beta-lactams: direct DNA incorporation and remodeling of penicillin-binding proteins via contact with closely related streptococci
- Resistance to macrolides: ribosomal methylation (efflux - mef gene; ribosomal mutation - erm gene)
- When MIC ≥2 μg/mL for penicillin → use high-dose amoxicillin (3 g/day in divided doses) or respiratory fluoroquinolones
CA-MRSA
- Expresses Panton-Valentine leukocidin (PVL) - necrotizing pneumonia
- Often follows influenza, presents in young healthy patients
- Radiograph: rapidly progressing bilateral infiltrates/cavities
Macrolide Resistance in M. pneumoniae
- Binding-site mutation in domain V of 23S rRNA
- Rates: Japan (30%), China (95%), France/USA (5-13%)
Treatment of CAP
Algorithm for MRSA/Pseudomonas Risk Assessment
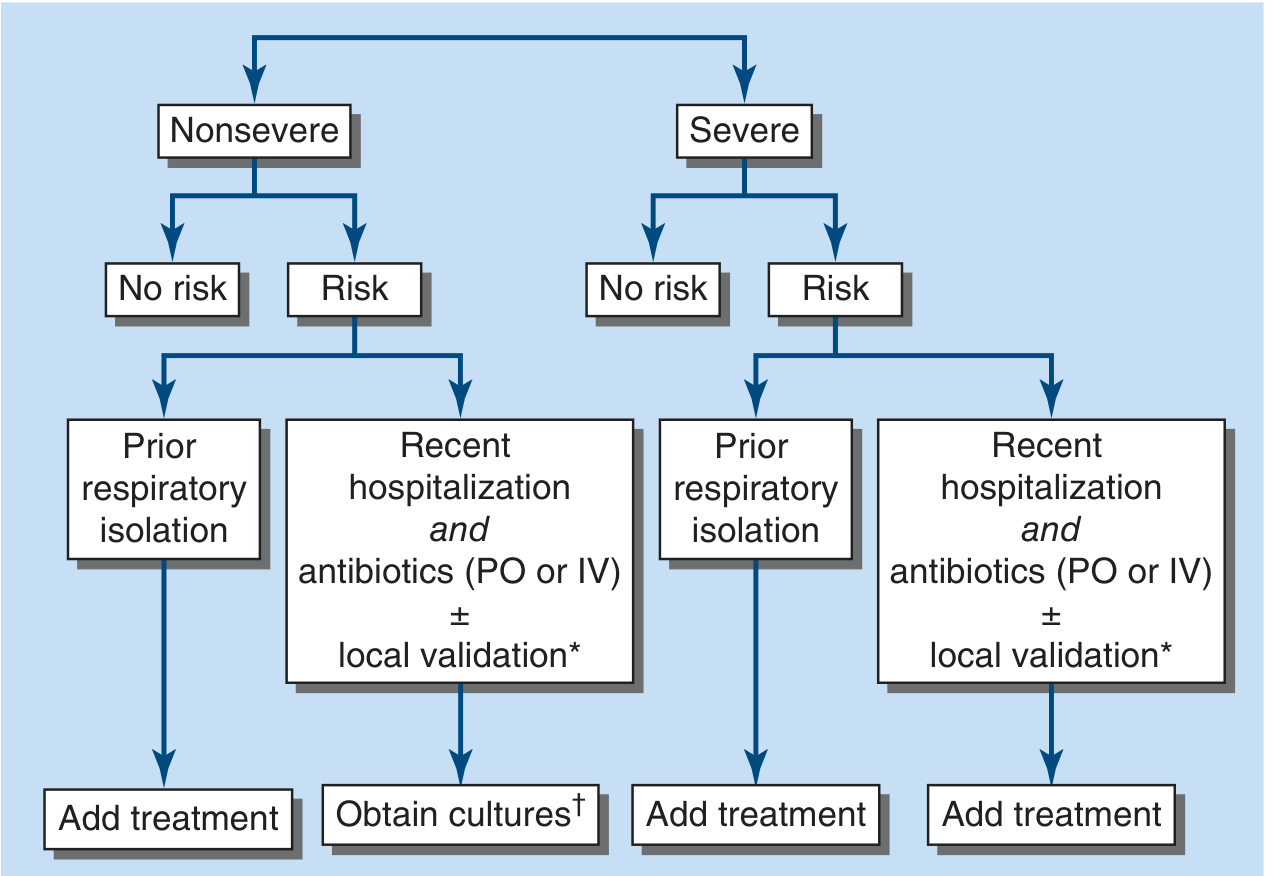
FIGURE 131-1 - Algorithm for assessment of inpatient risk of infection with MRSA or P. aeruginosa. Prior respiratory isolation = prior positive respiratory culture. Recent hospitalization AND antibiotics ± local validation = obtain cultures before adding MRSA/pseudomonal coverage.
TABLE 131-4: Outpatient CAP Treatment
| Patient Status | Regimen | Doses |
|---|---|---|
| No comorbidities, no resistance risk | Amoxicillin + macrolide or doxycycline | Amoxicillin 1 g TID + Azithromycin 500 mg day 1 then 250 mg/d × 4 days OR Clarithromycin 500 mg BID |
| Doxycycline monotherapy | 100 mg BID | |
| Macrolide monotherapy (if local resistance <25%) | Azithromycin or clarithromycin as above | |
| With comorbidities ± resistance risk | Amoxicillin-clavulanate + macrolide or doxycycline | Amox-clav 500/125 mg TID or 875/125 mg BID + macrolide or doxycycline 100 mg BID |
| OR cephalosporin + macrolide or doxycycline | Cefpodoxime 200 mg BID or Cefuroxime 500 mg BID | |
| Respiratory fluoroquinolone monotherapy | Levofloxacin 750 mg/d, Moxifloxacin 400 mg/d, or Gemifloxacin 320 mg/d |
TABLE 131-5: Inpatient CAP Treatment
| Severity & Risk | Regimen | Doses |
|---|---|---|
| Nonsevere, no risk factors | Beta-lactam + macrolide | Ceftriaxone 1-2 g/d + Azithromycin 500 mg/d |
| OR respiratory fluoroquinolone | Levofloxacin 750 mg/d or Moxifloxacin 400 mg/d IV | |
| Nonsevere, prior respiratory isolation | Add MRSA or P. aeruginosa coverage | (See below) |
| Nonsevere, recent hospitalization + antibiotics ± local validation | Obtain cultures; add MRSA or P. aeruginosa only if cultures positive | |
| Severe, no risk factors | Beta-lactam + macrolide OR Beta-lactam + respiratory FQ | As above; escalate dosing |
| Severe, prior isolation or recent hospitalization | Add MRSA + P. aeruginosa coverage | (See below) |
Beta-lactam options: Ampicillin-sulbactam 1.5-3 g IV q6h, Ceftriaxone 1-2 g/d IV, Cefotaxime 1-2 g IV q8h, Ceftaroline 600 mg IV q12h, or Ertapenem 1 g/d IV
MRSA coverage: Vancomycin 15 mg/kg IV q12h (adjust to trough 15-20 mg/L) OR Linezolid 600 mg IV/PO q12h
P. aeruginosa coverage: Piperacillin-tazobactam 4.5 g IV q6h, Cefepime 2 g IV q8h, or Imipenem 500 mg IV q6h
HAP and VAP
Etiology
VAP Pathogens (TABLE 131-6):
| Non-MDR Pathogens ("Core Pathogens") | MDR Pathogens |
|---|---|
| S. pneumoniae, H. influenzae, MSSA | P. aeruginosa |
| E. coli, K. pneumoniae | MRSA |
| Proteus spp., Enterobacter spp. | Acinetobacter spp. |
| Serratia marcescens | ESBL-positive / carbapenem-resistant Enterobacteriaceae |
| Legionella pneumophila, Aspergillus spp. |
Key Epidemiologic Points
- VAP develops in 6-52% of mechanically ventilated patients
- On any given day in ICU: ~10% of patients have pneumonia (vast majority VAP)
- Highest hazard in first 5 days of ventilation; plateau of ~1% per day after ~2 weeks
- COVID-19 has reversed the previously declining trend in VAP frequency
Diagnosis
- In non-intubated HAP: expectorated sputum (confounded by colonization)
- In VAP/ventilated HAP: bronchoscopic BAL, protected specimen brushing, or mini-BAL from endotracheal tube
TABLE 131-8: Empirical Treatment of HAP/VAP
| Risk Category | Beta-Lactam | Second Agent (if MDR risk) | Add if MRSA risk |
|---|---|---|---|
| No MDR risk | Piperacillin-tazobactam 4.5 g IV q6h | - | - |
| Cefepime 2 g IV q8h | - | - | |
| Levofloxacin 750 mg IV q24h | - | - | |
| MDR risk (choose 1 from each column) | Piperacillin-tazobactam 4.5 g IV q6h | Amikacin 15-20 mg/kg IV q24h | Linezolid 600 mg IV q12h |
| Cefepime 2 g IV q8h | Gentamicin 5-7 mg/kg IV q24h | OR Vancomycin (trough 15-20 mg/L) | |
| Ceftazidime 2 g IV q8h | Tobramycin 5-7 mg/kg IV q24h | ||
| Imipenem 500 mg IV q6h | Ciprofloxacin 400 mg IV q8h | ||
| Meropenem 1 g IV q8h | Levofloxacin 750 mg IV q24h | ||
| Consider newer agents* | Colistin (loading 5 mg/kg IV, then 2.5 mg × [1.5 × CrCl + 30] IV q12h) | ||
| Polymyxin B 2.5-3.0 mg/kg/day IV in 2 divided doses |
Newer agents for resistant organisms:
- Ceftazidime-avibactam, ceftolozane-tazobactam, imipenem-relebactam, plazomicin → resistant P. aeruginosa
- Meropenem-vaborbactam, ceftazidime-avibactam → carbapenem-resistant Enterobacteriaceae
- Cefiderocol → metallo-beta-lactamase Enterobacteriaceae, Stenotrophomonas, Acinetobacter
- Sulbactam-durlobactam → Acinetobacter spp.
De-escalation, Duration, and Response
- De-escalation should occur once culture data return and clinical response is documented
- Duration for CAP: 5 days for most non-severe CAP if afebrile ×48-72 h; up to 7-10 days for more severe disease or specific pathogens (S. aureus, Pseudomonas, Legionella → 14-21 days)
- Duration for HAP/VAP: 7 days for most patients (shorter is non-inferior to longer in trials)
- Reassessment at 72 h is mandatory - if not improving, consider: wrong pathogen, wrong antibiotic, complication (effusion/empyema, lung abscess), or non-infectious diagnosis
Prevention
| Strategy | Details |
|---|---|
| Pneumococcal vaccine (PCV15, PCV20, PPSV23) | All adults ≥65; immunocompromised at younger ages |
| Annual influenza vaccine | All adults; especially elderly, healthcare workers |
| Smoking cessation | Major modifiable risk factor for CAP |
| VAP bundle | HOB elevation 30-45°, daily sedation interruption, oral chlorhexidine, subglottic secretion drainage, early enteral feeding |
Global Impact
Pneumonia has a profound global impact though precise data are hard to collect due to variation in:
- Etiologic pathogens and resistance rates between countries
- Access to diagnostic facilities and healthcare
- Vaccine availability and uptake
Simple extrapolation from U.S. data demonstrates substantial effects on quality of life, morbidity, healthcare costs, and mortality across all age groups.
CHAPTER 132: LUNG ABSCESS
Definition
Lung abscess represents necrosis and cavitation of the lung following microbial infection. Usually marked by a single dominant cavity >2 cm in diameter, though multiple abscesses can occur.
Classification
| Classification | Description |
|---|---|
| Primary (~80%) | Arises from aspiration; mainly anaerobic bacteria; no underlying pulmonary or systemic condition |
| Secondary (~20%) | Arises in setting of underlying condition (obstruction - foreign body, tumor; or systemic - HIV, immunosuppression) |
| Acute | Duration <4-6 weeks |
| Chronic (~40%) | Duration ≥4-6 weeks |
Epidemiology
- Middle-aged men more commonly affected than women
- Major risk factor: Aspiration
Risk Factors for Primary Lung Abscess
| Category | Examples |
|---|---|
| Altered mental status | Alcoholism, drug overdose, seizures, encephalopathy |
| Neurologic disease | Bulbar dysfunction, prior cerebrovascular events, neuromuscular disease |
| Esophageal disease | Dysmotility, strictures, tumors |
| GI risk | Gastric distension, gastroesophageal reflux, recumbent position |
| Oral/dental | Gingivitis, periodontal disease (anaerobic colonization of gingival crevices) |
The risk of aspiration combined with colonization of gingival crevices by anaerobic bacteria/microaerophilic streptococci drives primary lung abscess development. Many physicians consider lung abscess extremely rare in edentulous patients.
Historical note: Incidence fell dramatically in the late 1940s when oral surgical operations stopped being performed in the seated position without cuffed ETT (reducing perioperative aspiration). Penicillin availability further reduced incidence and mortality.
Etiology
TABLE 132-1: Microbial Pathogens Causing Lung Abscess
| Clinical Condition | Pathogens |
|---|---|
| Primary lung abscess (aspiration) | Anaerobes: Peptostreptococcus spp., Prevotella spp., Bacteroides spp., milleri group streptococci; microaerophilic streptococci |
| Secondary lung abscess (immunocompromise) | S. aureus, gram-negative rods (P. aeruginosa, Enterobacteriaceae), Nocardia spp., Aspergillus spp., Mucorales, Cryptococcus spp., Legionella spp., Rhodococcus equi, P. jirovecii |
| Embolic lesions | S. aureus (endocarditis), Fusobacterium necrophorum (Lemierre's syndrome) |
| Endemic infections | M. tuberculosis, M. avium, M. kansasii, Coccidioides spp., Histoplasma capsulatum, Blastomyces spp., parasites (E. histolytica, Paragonimus westermani, Strongyloides stercoralis) |
| Miscellaneous | Bacterial (often S. aureus) after influenza or viral infection, Actinomyces spp. |
Pathogenesis
Primary Lung Abscess
- Aspiration of anaerobes/microaerophilic streptococci from gingival crevices into lung parenchyma
- Initial pneumonitis develops (worsened by gastric acid tissue damage)
- Over 7-14 days: parenchymal necrosis and cavitation
- Anaerobes produce more extensive tissue necrosis in polymicrobial infections (synergistic virulence factor action)
- Dependent lung segments most affected: posterior segment of RUL and apical segments of lower lobes (aspiration in recumbent position); posterior segment of LUL and RML (aspiration in upright position)
Secondary Lung Abscess
- Post-obstructive: Bronchial obstruction (malignancy, foreign body) prevents secretion clearance → abscess formation
- Immunosuppressed host: Impaired host defenses (post-BMT, solid organ transplant, HIV) → susceptibility to atypical pathogens
Imaging
Chest Radiograph
- Thick-walled cavity with air-fluid level (classic finding)
- Location: dependent segments (posterior upper lobe, superior lower lobe)
- May take time to distinguish from empyema with bronchopleural fistula
CT Chest (Preferred)
- Better anatomic definition than plain film
- May detect abscess earlier than radiograph
- Distinguishes abscess from empyema, identifies underlying lesion (tumor, obstruction)
- Guides percutaneous drainage planning

FIGURE 132-1: Representative chest CT scans showing development of lung abscess. Panel A (left): Left lung infiltrate with central necrosis in a patient with lymphoma-associated severe P. aeruginosa pneumonia (black arrow). Panel B (right): Two weeks later, cavitation with air-fluid levels consistent with lung abscesses (white arrow). [Harrison's 22E, p. 1078]
Clinical Features
Symptoms
| Symptom | Notes |
|---|---|
| Cough | Productive; often purulent, foul-smelling sputum (anaerobic) |
| Fever | Subacute onset; may be low-grade initially |
| Pleuritic chest pain | Especially if pleural extension |
| Night sweats, fatigue | Constitutional symptoms, often weeks before diagnosis |
| Hemoptysis | Occurs; life-threatening if massive |
| Weight loss | Prominent in chronic abscesses |
Physical Examination
| Finding | Notes |
|---|---|
| Decreased breath sounds | Over affected area |
| Dullness to percussion | Especially with associated effusion/empyema |
| Amphoric breath sounds | Sometimes heard over large cavities |
| Oral/dental disease | Periodontal disease, poor dentition strongly suggestive |
Diagnosis
Lung abscesses are documented by chest imaging:
- Chest radiograph detects thick-walled cavity with air-fluid level
- CT provides better definition and may provide earlier detection
Microbiologic Workup
- Blood cultures - obtain before antibiotics
- Sputum culture - limited by oropharyngeal contamination
- Bronchoscopy with BAL or protected specimen brushing - more reliable for culture, especially in secondary/immunocompromised cases
- Thoracentesis - if associated pleural effusion (rule out empyema)
- Consider Gram stain, aerobic and anaerobic cultures, fungal cultures, AFB smear/culture depending on clinical context
- Serologies/PCR for endemic fungi, Legionella, as indicated
Key Distinguishing Considerations
| Feature | Lung Abscess | Empyema with BPF | Cavitary Malignancy |
|---|---|---|---|
| Wall thickness | Thick, irregular | Thin, smooth | Irregular, nodular |
| Air-fluid level | Present (round) | Present (lenticular) | May be present |
| Location | Parenchymal | Pleural space | Variable |
| Associated symptoms | Fever, putrid sputum | Fever, pleurisy | Weight loss, hemoptysis |
Treatment
Antibiotic Therapy (Primary Lung Abscess)
Key point: Clindamycin is superior to penicillin in clinical trials for primary lung abscess because oral anaerobes can produce beta-lactamases.Metronidazole is NOT effective as monotherapy - covers anaerobes but NOT the microaerophilic streptococci that are frequently part of the mixed flora.
| Regimen | Dose | Notes |
|---|---|---|
| Clindamycin (preferred, Option 1) | 600 mg IV TID → when afebrile: 300 mg PO QID | Switch to oral once clinical improvement |
| Beta-lactam/beta-lactamase inhibitor (Option 2) | Ampicillin-sulbactam or piperacillin-tazobactam IV → then Amoxicillin-clavulanate 875/125 mg PO BID | IV until stable, then oral step-down |
| Moxifloxacin (evidence: small study) | 400 mg/d PO | Comparable to ampicillin-sulbactam |
Treatment Duration
- Continue until imaging shows abscess cleared or regressed to small scar
- Range: 3-4 weeks to up to 14 weeks
- Some literature suggests ≥6 weeks associated with better outcomes
- Secondary abscesses: prolonged course until resolution documented
Secondary Lung Abscess
- Direct antibiotic coverage at identified pathogen
- Prolonged courses required (duration until resolution on imaging)
- Address underlying cause: relieve obstruction, treat systemic condition
- If presumed primary abscess fails to improve → workup for secondary cause
Interventional/Surgical Management
When to Consider Additional Interventions
- No response to antibiotics within 7 days (10-20% of patients fail medical therapy)
- Continued fevers + progressive cavity on imaging
- Abscess >6-8 cm - less likely to respond to antibiotics alone
| Approach | Considerations |
|---|---|
| Percutaneous drainage | Option when poor surgical candidate; risks: pleural contamination, pneumothorax, hemothorax; traversing normal lung = major complication risk |
| Surgical resection | Definitive but reserved for failed medical + failed percutaneous approaches; timing is challenging (balance morbidity risk vs. need to clear persistent infection) |
| Bronchoscopy | Can facilitate drainage and obtain better cultures; therapeutic role in postobstructive abscesses |
Complications
| Complication | Notes |
|---|---|
| Pneumatoceles | Persistent cystic changes post-abscess; correlates with larger cavity size |
| Bronchiectasis | Permanent airway damage |
| Empyema | Extension to pleural space; requires drainage |
| Life-threatening hemoptysis | Major vascular erosion |
| Massive aspiration of abscess contents | Can cause respiratory failure |
| Recurrence | Despite appropriate therapy |
Prognosis
| Factor | Mortality Impact |
|---|---|
| Primary abscess (overall) | ~2% mortality |
| Secondary abscess | Up to 75% mortality in some series |
| Poor prognostic factors | Age >60, malignancy-related, aerobic bacteria, sepsis at presentation, symptoms >8 weeks, abscess size >6 cm |
Prevention
| Strategy | Details |
|---|---|
| Airway protection | Cuffed endotracheal tube for at-risk surgical/sedated patients |
| Oral hygiene | Reduce gingival anaerobic colonization |
| Minimize sedation | Decreases aspiration risk |
| Head-of-bed elevation | 30-45° for patients at aspiration risk |
| Treat underlying conditions | GERD, esophageal disease, neurologic disease |
Lemierre's Syndrome (Special Mention)
A distinct form of secondary lung abscess caused by Fusobacterium necrophorum:
- Begins as peritonsillar/oropharyngeal infection
- Leads to internal jugular vein thrombophlebitis
- Septic emboli travel to lungs → multiple bilateral cavitary lesions
- Treatment: prolonged beta-lactam/metronidazole + anticoagulation (controversial)
Summary Comparison: Pneumonia vs. Lung Abscess
| Feature | Pneumonia | Lung Abscess |
|---|---|---|
| Pathology | Alveolar exudate/consolidation | Parenchymal necrosis + cavitation >2 cm |
| Key pathogens | S. pneumoniae, atypicals, viruses | Anaerobes, S. aureus, gram-negatives |
| Risk factors | Age extremes, immunosuppression, comorbidities | Aspiration, poor dentition, alcoholism |
| Classic imaging | Consolidation/infiltrate | Thick-walled cavity + air-fluid level |
| Key antibiotic | Beta-lactam ± macrolide/FQ | Clindamycin or amox-clavulanate |
| Duration | 5-14 days | 3-14 weeks |
| Surgery | Rarely needed | 10-20% fail medical therapy → drainage/surgery |
Sources: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapters 131 (Mandell & Niederman) and 132 (Baron, Baron & Barshak), McGraw Hill Medical.
This is a shared conversation. Sign in to Orris to start your own chat.