Explain me the Management of eclempsia and pre eclampsia, with details of mgso4
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full, detailed answer.
Management of Pre-eclampsia and Eclampsia
1. Diagnostic Criteria
Preeclampsia is defined as new-onset hypertension (SBP ≥140 mmHg or DBP ≥90 mmHg) after 20 weeks of gestation, plus at least one of the following (proteinuria is no longer required per ACOG 2013):
| Feature | Threshold |
|---|---|
| Proteinuria | ≥300 mg/24 h or protein:creatinine ≥0.3 |
| Thrombocytopenia | Platelets <100,000/µL |
| Renal insufficiency | Creatinine >1.1 mg/dL or doubling of baseline |
| Liver dysfunction | Transaminases ≥2× upper limit of normal |
| Pulmonary edema | New onset |
| Visual/neurological symptoms | New headache, visual disturbances |
Eclampsia = preeclampsia + new-onset grand mal seizures not attributed to another cause.
HELLP syndrome = Hemolysis + Elevated Liver enzymes + Low Platelets - a severe variant.
2. Initial Evaluation at Diagnosis
Once preeclampsia is diagnosed, immediately classify as with or without severe features:
- Assess symptoms (headache, visual changes, epigastric/RUQ pain, dyspnea)
- Labs: CBC, LFTs, serum creatinine, LDH, uric acid, coagulation studies
- Fetal assessment: estimated fetal weight, amniotic fluid index, antenatal testing (NST/BPP)
3. Management by Severity and Gestational Age
A. Preeclampsia WITHOUT Severe Features
| Gestational Age | Management |
|---|---|
| ≥37 weeks | Prompt delivery (induction of labor) |
| 34-36+6 weeks | Expectant management if fetal well-being reassuring, no severe features; target delivery by 37 weeks |
| <34 weeks | Expectant management with antenatal corticosteroids + close monitoring (inpatient vs outpatient based on reliability/distance) |
Monitoring during expectant management:
- BP assessment + symptom review at least weekly
- Labs (CBC, LFTs, creatinine) weekly
- NST or BPP at least twice weekly
- Amniotic fluid assessment weekly
- Fetal growth ultrasound every 3 weeks
- Daily fetal kick counts counseling
- Continued proteinuria reassessment is NOT recommended
MgSO4 use: ACOG does NOT recommend routine MgSO4 for preeclampsia without severe features due to insufficient evidence of benefit.
B. Preeclampsia WITH Severe Features
| Gestational Age | Management |
|---|---|
| ≥37 weeks | Prompt delivery |
| 34-36+6 weeks | Deliver; consider brief course of antenatal corticosteroids if >12 hours until delivery |
| <34 weeks | Antenatal corticosteroids first; expectant management may extend pregnancy 5-19 days IF none of the contraindications below are present |
Contraindications to expectant management at any gestational age:
- Eclampsia
- Pulmonary edema
- DIC
- Uncontrollable severe hypertension
- Abnormal fetal testing
- Placental abruption
- Stillbirth
- Nonviable fetus
After completing corticosteroid course (<34 weeks), delivery is indicated if any of the following develop:
- HELLP syndrome
- Persistent neurologic symptoms or epigastric/RUQ pain
- Platelets <100,000/µL, transaminases >2× ULN, creatinine >1.1 mg/dL
- Reversed end-diastolic flow on umbilical artery Doppler
- Labor or PPROM
MgSO4 is given as seizure prophylaxis for ALL patients with preeclampsia with severe features during labor and delivery.
C. Eclampsia (Active Seizure)
- Protect airway, position patient left lateral
- Administer MgSO4 (see dosing below) - this is the drug of choice
- After seizure control, plan delivery - eclampsia is not itself an indication for cesarean; vaginal delivery is preferred if feasible
- Delivery is the definitive treatment - perform within 24-48 hours of presentation
4. Hypertensive Emergency Management
Threshold: SBP ≥160 mmHg or DBP ≥110 mmHg persisting >15 minutes = obstetric emergency. Treatment must be given within 30-60 minutes of diagnosis. Target BP: 140-150 mmHg systolic / 90-100 mmHg diastolic.
Flowchart for Acute Hypertension in Pregnancy
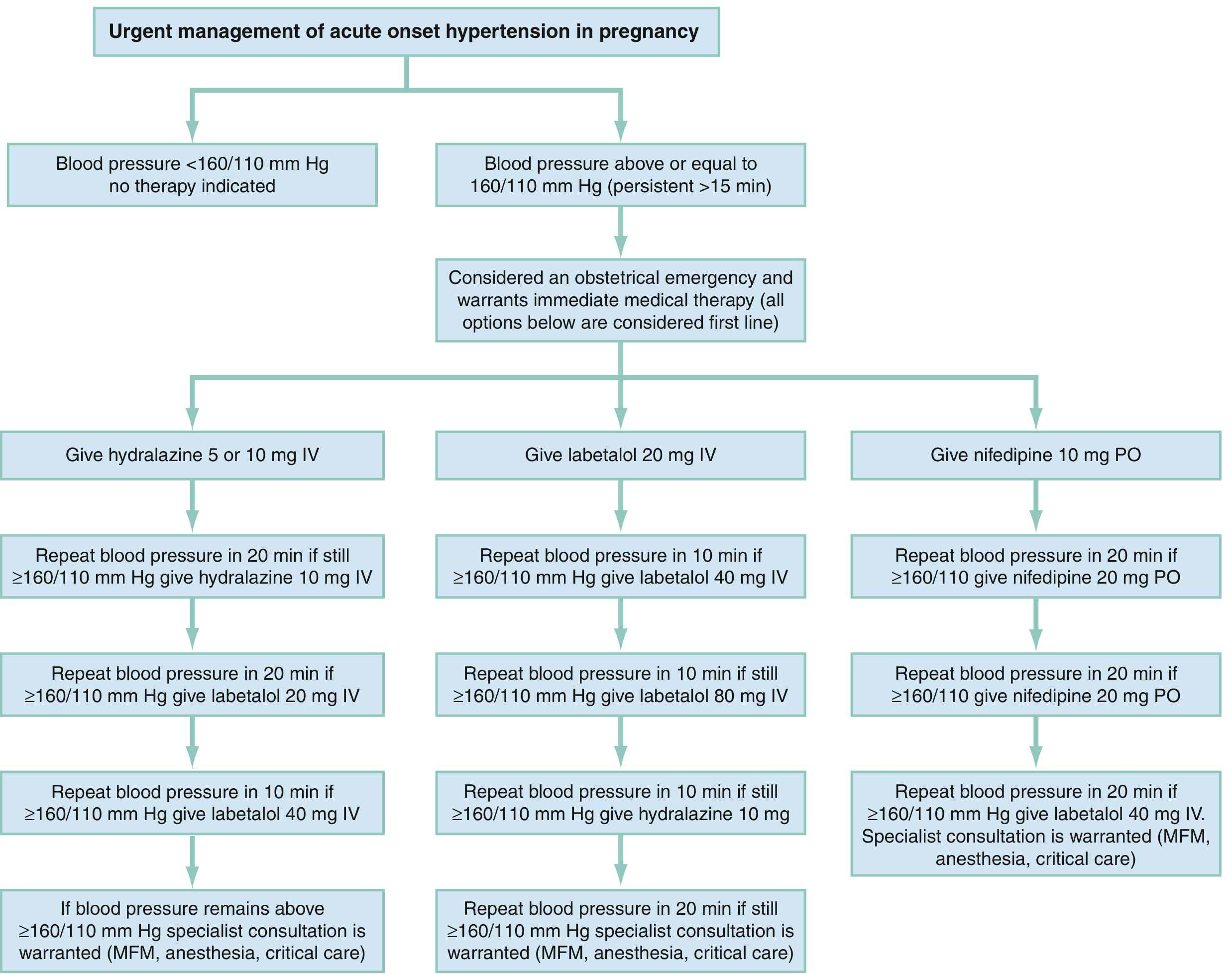
First-Line Antihypertensive Agents
| Drug | Starting Dose | Repeat | Onset | Duration | Notes |
|---|---|---|---|---|---|
| Hydralazine (IV/IM) | 5 mg IV/IM | 10 mg q20-40 min | 10-20 min | 3-8 h | Reflex tachycardia; headache may mimic worsening PE |
| Labetalol (IV) | 20 mg IV bolus | Double dose q10 min (max 80 mg/dose; 300 mg total) | 1-2 min | 6-16 h | Contraindicated in asthma, heart failure |
| Nifedipine (PO, immediate release) | 10 mg PO | 10-20 mg q20-30 min | 5-10 min | 4-8 h | Use when IV access unavailable; monitor for MgSO4 interaction |
Agents contraindicated in pregnancy: Atenolol, ACE inhibitors, angiotensin receptor blockers, direct renin inhibitors.
Avoid aggressive diuretics - preeclamptic women are already plasma volume depleted.
5. Magnesium Sulfate (MgSO4) - Detailed
Indications
- Seizure prophylaxis: preeclampsia with severe features (antepartum, intrapartum, and postpartum)
- Treatment of active eclamptic seizures
- NOT routinely indicated for preeclampsia without severe features
Mechanism of Action
The exact mechanism is incompletely understood. Proposed theories include:
- Cerebrovascular effect - MgSO4 causes vasodilation of cerebral vessels, reversing the ischemia/vasospasm underlying eclamptic seizures
- NMDA receptor antagonism - blocks N-methyl-D-aspartate receptors, reducing neuronal excitability
Additionally, elevated serum magnesium concentrations act on cell membranes to:
- Slow/block neuromuscular and cardiac conduction
- Decrease smooth muscle contractility
- Depress CNS irritability
Importantly, blood pressure is not appreciably lowered by prophylactic magnesium doses.
Pharmacokinetics
- Distribution beyond extracellular fluid (enters bones and cells; volume > sucrose)
- Circulates largely unbound to proteins
- Almost exclusively excreted in urine (renal tubular reabsorption up to Tmax)
- Normal renal function: half-life ~4 hours
- Prolonged half-life with decreased GFR - dose reduction required
Standard Dosing Regimen (IV, USA)
| Phase | Dose |
|---|---|
| Loading dose | 4-6 g IV over 15-30 minutes |
| Maintenance infusion | 1-2 g/h continuous IV infusion |
- Use mechanically controlled infusion pump (mandatory - prevents inadvertent large dose)
- If maternal creatinine >1 mg/dL: reduce to 1 g/h or less
- Duration: Continue through labor/delivery and for 24 hours postpartum
Serum Magnesium Levels and Effects
| Effect | Serum Level (mEq/L) |
|---|---|
| Anticonvulsant prophylaxis (therapeutic target) | 4.8 - 8.4 |
| Loss of deep tendon reflexes | 7 - 10 |
| Respiratory paralysis | 10 - 13 |
| ECG changes | >15 |
| Cardiac arrest | >25 |
Monitoring (every 2 hours minimum)
- Deep tendon reflexes (DTRs) - most important clinical sign
- Presence of DTRs = serum level is not dangerously high
- Loss of DTRs = level likely >10 mEq/L - hold infusion and reassess
- Respiratory rate - must be ≥12/min before each dose
- Urine output - must be ≥25-30 mL/h (renal excretion is the only route of elimination)
- Level monitoring - not routinely needed if renal function is normal; use if creatinine is elevated
Antidote for Toxicity
Calcium gluconate - 10 mL of 10% solution (1 g) IV over 3 minutes
- Indicated if respiratory depression, apnea, or severe toxicity
Efficacy Evidence
- Meta-analysis of 6 RCTs (11,444 women): MgSO4 reduces the risk of eclampsia by more than 50% compared to no anticonvulsant
- Head-to-head trials: MgSO4 is superior to both phenytoin and diazepam for prevention and treatment of eclamptic seizures
- MgSO4 reduces recurrent seizures better than diazepam or phenytoin in women with eclampsia
When MgSO4 is contraindicated (use phenytoin or alternatives):
- Myasthenia gravis (MgSO4 potentiates neuromuscular blockade)
- Severe renal failure (acute or chronic)
Neonatal Considerations
- Average neonatal serum magnesium level in infants of treated mothers ~3.7 mEq/L
- Generally safe; monitor newborn for respiratory depression and hypotonia
6. Postpartum Management
- Continue MgSO4 for 24 hours postpartum in women who received it antepartum
- A noninferiority trial showed no difference in eclampsia rates between 24-hour continuation vs. stopping at delivery; however, 24 hours remains standard practice at most centers
- Monitor BP closely postpartum - hypertension can worsen in the first 3-5 days
- Resume/initiate oral antihypertensives if BP remains elevated
- Safe antihypertensives for breastfeeding: Labetalol, nifedipine, methyldopa
7. Prevention in High-Risk Women
For women with strong risk factors (prior preeclampsia, chronic hypertension, pregestational diabetes, BMI >30, antiphospholipid syndrome, ART):
- Low-dose aspirin 75-162 mg/day (ideally started before 16 weeks, no later than 20 weeks) to prevent preterm preeclampsia
- Calcium supplementation 1.2-2.5 g/day if dietary intake <600 mg/day
- Folic acid and vitamin D have not been shown to reduce preeclampsia risk
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, pp. 1069-1073 (Antepartum/Intrapartum Management, MgSO4 dosing, antihypertensive agents)
- Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 3373-3374 (Hypertensive emergencies in pregnancy, flowchart)
- Bradley and Daroff's Neurology in Clinical Practice, p. 2916 (MgSO4 mechanism)
- Swanson's Family Medicine Review, p. 500 (Eclampsia prophylaxis, MgSO4 vs phenytoin)
This is a shared conversation. Sign in to Orris to start your own chat.