Diabetic ketoacidosis management in pediatrics
Reading File
Finding Sources
Searching PubMed
"diabetic ketoacidosis" AND "pediatric" AND management
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading Article
PMID: 41296041
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive content to provide a detailed, well-structured answer. Let me compile everything.
Diabetic Ketoacidosis (DKA) Management in Pediatrics
Epidemiology & Background
Diabetes is the most common pediatric endocrine disorder, with a prevalence of approximately 1 in 400 children. Up to 34% of children with new-onset type 1 diabetes present in DKA. In children with known diabetes, DKA tends to cluster in a small subset - roughly 5% of children account for nearly 60% of DKA episodes. DKA is the leading cause of mortality in patients with diabetes under 24 years of age, and cerebral edema is the leading cause of DKA-related death.
- Tintinalli's Emergency Medicine, p. 1013
Pathophysiology
The core problem is absolute or relative insulin deficiency, resulting in cells being unable to take up glucose. Counterregulatory hormones (catecholamines, cortisol, growth hormone, glucagon) rise, driving:
- Glycogenolysis and gluconeogenesis (hyperglycemia)
- Lipolysis and ketogenesis (ketonemia)
- Osmotic diuresis as glucose exceeds the renal threshold (dehydration, electrolyte loss)
- Conversion of free fatty acids to acetoacetate and beta-hydroxybutyrate (wide anion gap metabolic acidosis)
Note: Beta-hydroxybutyrate is the major ketoacid but does not react with nitroprusside-based urine/serum ketone assays - so measured ketone levels may appear deceptively low, and ketones paradoxically rise on therapy as beta-hydroxybutyrate converts to acetoacetate.
Corrected serum sodium formula (important for monitoring):
Corrected Na = [1.6 × ((serum glucose - 100) / 100)] + measured Na
Monitoring During Treatment
- Bedside glucose every 1 hour
- Electrolytes and venous blood gases every 2 hours
- Continuous cardiac monitoring - QTc prolongation occurs frequently in DKA and correlates with ketosis, potentially causing torsades de pointes
- Avoid medications that prolong the QT interval (e.g., ondansetron)
- Monitor perfusion, electrolytes, mental status, hyperglycemia, and ketonemia
1. Fluid Resuscitation
Average fluid deficit is 5-10% of body weight (may be greater).
| Situation | Approach |
|---|---|
| Shock / hemodynamic instability | 20 mL/kg bolus of normal saline (0.9% NaCl); repeat if still hypotensive |
| After stabilization | Replace deficit evenly over 24-48 hours |
| Alternative | 50% deficit replacement in first 8 hours; remainder over next 16-24 hours |
| High osmolarity (>340 mOsm/L) | Extra caution - avoid rapid fluid correction |
After the initial bolus, run NS at 1.5x maintenance rate in the ED. Some protocols use 0.66% NaCl to 0.9% NaCl to ensure a steady rise in serum sodium (falling or static sodium during therapy predicts cerebral edema).
Important update: A large multicenter RCT found no difference in neurologic outcomes based on fluid type or rate of administration, suggesting more rapid fluid administration does not increase cerebral edema risk - though caution is still warranted in severely hyperosmolar children.
2. Insulin Therapy
- Do NOT give an insulin loading bolus - associated with increased risk of cerebral edema
- Start IV regular insulin only after the initial fluid bolus is complete
- Dose: 0.1 unit/kg/hour
- Target glucose decline: 50-100 mg/dL/hour (controlled rate to prevent osmolar shifts)
When glucose drops to <250 mg/dL (14 mmol/L):
- Add dextrose to IV fluids - do NOT stop insulin
- Maintain glucose at 150-300 mg/dL until ketoacidosis resolves
- If pH improvement is too slow (<0.03 pH units/hour), the insulin infusion rate can be doubled
Minimum insulin rate:
- Do not reduce below 0.05 units/kg/hour - insulin is required to clear ketosis even after glucose normalizes
Transitioning to subcutaneous insulin:
- Wait until pH >7.30, bicarbonate >15 mEq/L, and serum ketones cleared
- Taper IV insulin to 0.02-0.05 units/kg/hour
- Start multidose SC regular insulin at 0.1 unit/kg every 2 hours
- Overlap IV and SC insulin by 1-2 hours before stopping IV
Recent evidence (2025 meta-analysis, PMID 41296041): Early initiation of long-acting basal insulin (glargine/detemir) during IV insulin with ≥4 hour overlap shortens DKA resolution by ~3-5 hours without increasing hypoglycemia or hypokalemia. This is an emerging practice to discuss with a pediatric endocrinologist.
3. Potassium Replacement
Total-body potassium deficits are large. Initial rehydration and insulin both cause precipitous drops in serum K+ due to redistribution.
| Serum K+ (mEq/L) | Action |
|---|---|
| >6.0 | Hold potassium; exclude hyperkalemia before adding |
| 3.5-5.5 | Add 30 mEq/L (half as KCl, half as KPO₄) if urinating |
| 2.5-3.5 | Add 40 mEq/L |
| <2.5 | Consider higher doses; central line + ICU required at most institutions |
| <3.0 (initial) | Profound deficit; aggressive replacement; hold insulin until K+ corrects |
- Never start potassium until hyperkalemia is excluded and the child is urinating
- Monitor serum potassium at least every 2 hours
4. Phosphate & Magnesium
- Phosphate depletion in DKA is common but IV replacement has not been proven beneficial
- Monitor for symptomatic hypophosphatemia (serum PO₄ <1 mmol/L): muscle weakness, rhabdomyolysis, respiratory depression
- If symptomatic, add potassium phosphate to IV fluids (provide half of potassium needs as KPO₄, half as KCl)
- Overaggressive phosphate replacement can cause hypocalcemia
- Same general approach applies to magnesium
5. Bicarbonate Therapy
Routine bicarbonate use is NOT recommended. It:
- Does not improve outcomes
- Is associated with a fourfold increase in cerebral edema risk
- Can cause volume overload, hypokalemia, hypernatremia, and paradoxical CNS acidosis
Only consider bicarbonate if:
- pH <7.0 AND
- Hemodynamic compromise unresponsive to fluid resuscitation
If used: 0.5-2.0 mEq/kg IV over 1-2 hours. Never correct beyond pH 7.1 or bicarbonate >10 mEq/L.
6. Cerebral Edema - The Most Feared Complication
Incidence: ~0.5-1% of all pediatric DKA cases, but accounts for 60-90% of all pediatric DKA deaths. Mortality 21-24%; only 14-57% of survivors recover neurologically normal.
Who is most at risk: Children <5 years old (rare >20 years)
Risk Factors
- Age <5 years
- Severe acidosis
- Severe hyperosmolality
- Failure of serum sodium to rise with treatment (key early warning)
- Initial insulin bolus administration
- Bicarbonate administration
Timing
Cerebral edema typically manifests 6-12 hours after onset of therapy, though it can occur as early as the first hour:
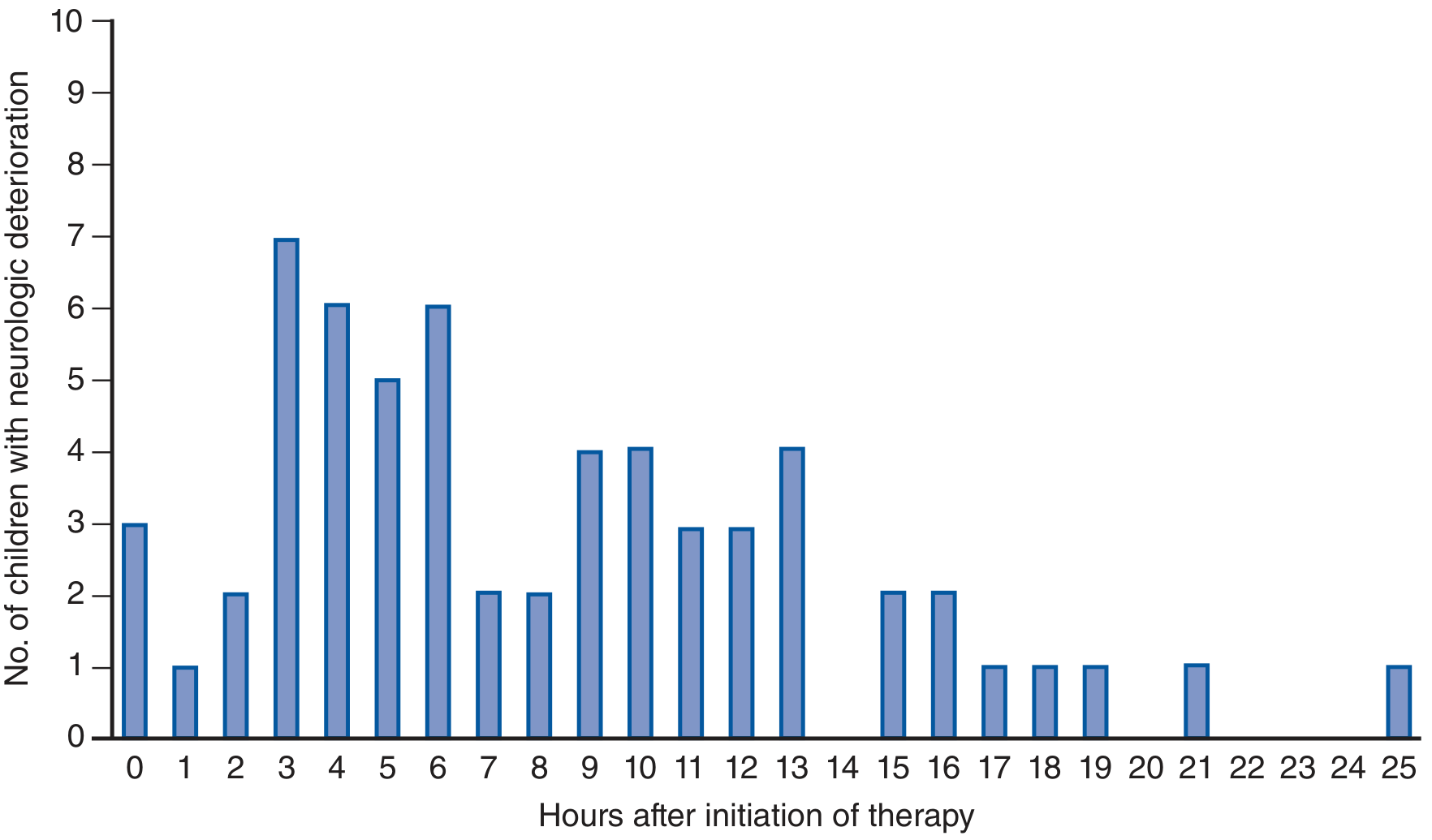
Neurologic deterioration peaks around 3-6 hours after therapy starts.
Clinical Features
- Severe headache, declining mental status, seizures, papilledema (premonitory signs in ~50%)
- Respiratory arrest may be the first sign - act before CT confirmation if clinical suspicion is high
- Once respiratory arrest has occurred, meaningful recovery is unlikely
Treatment
- Mannitol 0.25-1 g/kg IV bolus (standard of care)
- Hypertonic saline (3%): 5-10 mL/kg over 30 minutes (case series show improvement with 10 mL/kg over 30 min)
- Fluid restriction - minimize additional fluids
- Intubate if necessary; appropriate airway management
- Transfer to pediatric ICU
Disposition
-
Most children with DKA require ICU admission for intensive monitoring and insulin infusion
-
Discharge home can be considered only if:
- pH >7.35 and bicarbonate >20 mEq/L
- Known and resolving precipitant
- Good clinical appearance
- Solid social situation with reliable follow-up
-
In ~69% of patients with starting pH >7.20 or bicarbonate >10 mEq/L, acidosis resolves within 6 hours
Summary Table: Pediatric DKA Management
| Step | Action |
|---|---|
| Initial fluid | 20 mL/kg NS over 1 hour if hypotensive; repeat until normotensive |
| Fluid maintenance | 1.5x maintenance NS; replace deficit over 24-48 hours |
| Insulin | 0.1 units/kg/hour regular insulin (no bolus); never <0.05 units/kg/hour |
| Add dextrose | When glucose <250 mg/dL; keep glucose 150-300 mg/dL |
| K+ (3.5-5.5) | 30 mEq/L (half KCl, half KPO₄) if urinating |
| K+ (<3.5) | 40 mEq/L; do not start insulin if K+ <3.0 |
| Bicarbonate | Only pH <7.0 with hemodynamic collapse; 0.5-2 mEq/kg over 1-2 hours |
| Cerebral edema Tx | Mannitol 0.25-1 g/kg OR 3% NaCl 5-10 mL/kg; fluid restriction; intubate if needed |
| Monitoring | Glucose hourly; electrolytes/VBG every 2 hours; continuous ECG |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 147 (pp. 1013-1016)
- Shah A et al. Early vs. late initiation of long-acting basal insulin in pediatric DKA - Eur J Pediatr 2025 (PMID: 41296041) - Meta-analysis supporting early basal insulin overlap to shorten DKA resolution by 3-5 hours
This is a shared conversation. Sign in to Orris to start your own chat.