
IMG_20260523_081409.jpg
Interpretation of this cbc
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
iron deficiency anemia toddler microcytic hypochromic
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Now I have enough to provide a thorough interpretation. Let me compile the full analysis.
CBC Interpretation - Baby Mithun, 1 year 6 months, Male
Summary of Results
| Parameter | Result | Reference Range | Status |
|---|---|---|---|
| Haemoglobin (Hb) | 9 g/dL | 10.5 - 13.5 g/dL | Low |
| Total RBC | 3.21 million/cu.mm | 3.7 - 5.3 | Low |
| PCV (Hematocrit) | 27% | 33 - 39% | Low |
| MCV | 63 fL | 70 - 86 fL | Low |
| MCH | 21.6 pg | 23 - 31 pg | Low |
| MCHC | 34.3 g/dL | 30 - 36 g/dL | Normal |
| RDW | 17.7% | 11.5 - 16% | High |
| WBC | 8700 cells/cu.mm | 6000 - 17000 | Normal |
| Platelets | 275,000/cu.mm | 200,000 - 550,000 | Normal |
| MPV | 8.6 fL | 6.8 - 10.2 fL | Normal |
| Neutrophils | 27% | 15 - 46% | Normal |
| Lymphocytes | 66% | 45 - 76% | Normal |
| Eosinophils | 2% | Up to 3% | Normal |
| Monocytes | 5% | 2 - 8% | Normal |
Diagnosis: Microcytic Hypochromic Anemia - Most Likely Iron Deficiency Anemia (IDA)
Key CBC pattern:
- Hb 9 g/dL - moderate anemia (>2 SD below the mean for this age group)
- MCV 63 fL - significantly low (microcytic) - normal for age is 70-86 fL
- MCH 21.6 pg - low (hypochromic)
- RDW 17.7% - elevated (anisocytosis, i.e., unequal RBC sizes) - this is the crucial distinguishing feature
- Low RBC count (3.21) - distinguishes from thalassemia trait (where RBC is usually normal or elevated)
Mentzer Index = MCV / RBC = 63 / 3.21 = 19.6
- Index >13 strongly favors Iron Deficiency Anemia
- Index <13 would favor thalassemia trait
This pattern - low MCV + low MCH + elevated RDW + low RBC count + Mentzer index >13 - is the classic fingerprint of IDA.
Differential Diagnosis of Microcytic Hypochromic Anemia
| Feature | IDA (likely here) | Thalassemia Trait | Anemia of Chronic Disease |
|---|---|---|---|
| RBC count | Low (3.21 here) | Normal/High | Low |
| RDW | Elevated (17.7% here) | Normal | Normal/elevated |
| Mentzer Index | >13 (19.6 here) | <13 | - |
| Serum Iron | Low | Normal | Low |
| Ferritin | Low | Normal | Normal/High |
(Tietz Textbook of Laboratory Medicine, Table 77.6)
Why IDA is Common at This Age
This child is 18 months old - a peak risk age for IDA because:
- Rapid growth demands high iron
- Transition from breast/formula milk to solid foods (dietary iron may be insufficient)
- Cow's milk intake can impair iron absorption and cause occult GI bleeding
- The AAP recommends screening for anemia between 9-12 months precisely for this reason (Harriet Lane Handbook, 23rd ed.)
Next Steps Recommended
- Serum ferritin + serum iron + TIBC - to confirm IDA (ferritin will be low, TIBC elevated)
- Peripheral blood smear - to look for pencil cells, target cells, anisocytosis, poikilocytosis
- Reticulocyte count - if not already done; will be low/normal in IDA (hypoproliferative)
- Lead level - at this age, lead poisoning is a differential (leads to microcytic anemia with basophilic stippling on smear)
- If IDA confirmed: Dietary history + iron supplementation (elemental iron 3-6 mg/kg/day) and recheck Hb in 4 weeks
- If ferritin is normal, order Hb electrophoresis to rule out thalassemia trait
Reassuring Findings
- WBC (8700) and differential are completely normal - no signs of infection or bone marrow failure
- Platelets (275,000) are normal
- MCHC (34.3) is at the lower end of normal - consistent with IDA but not severely hypochromic
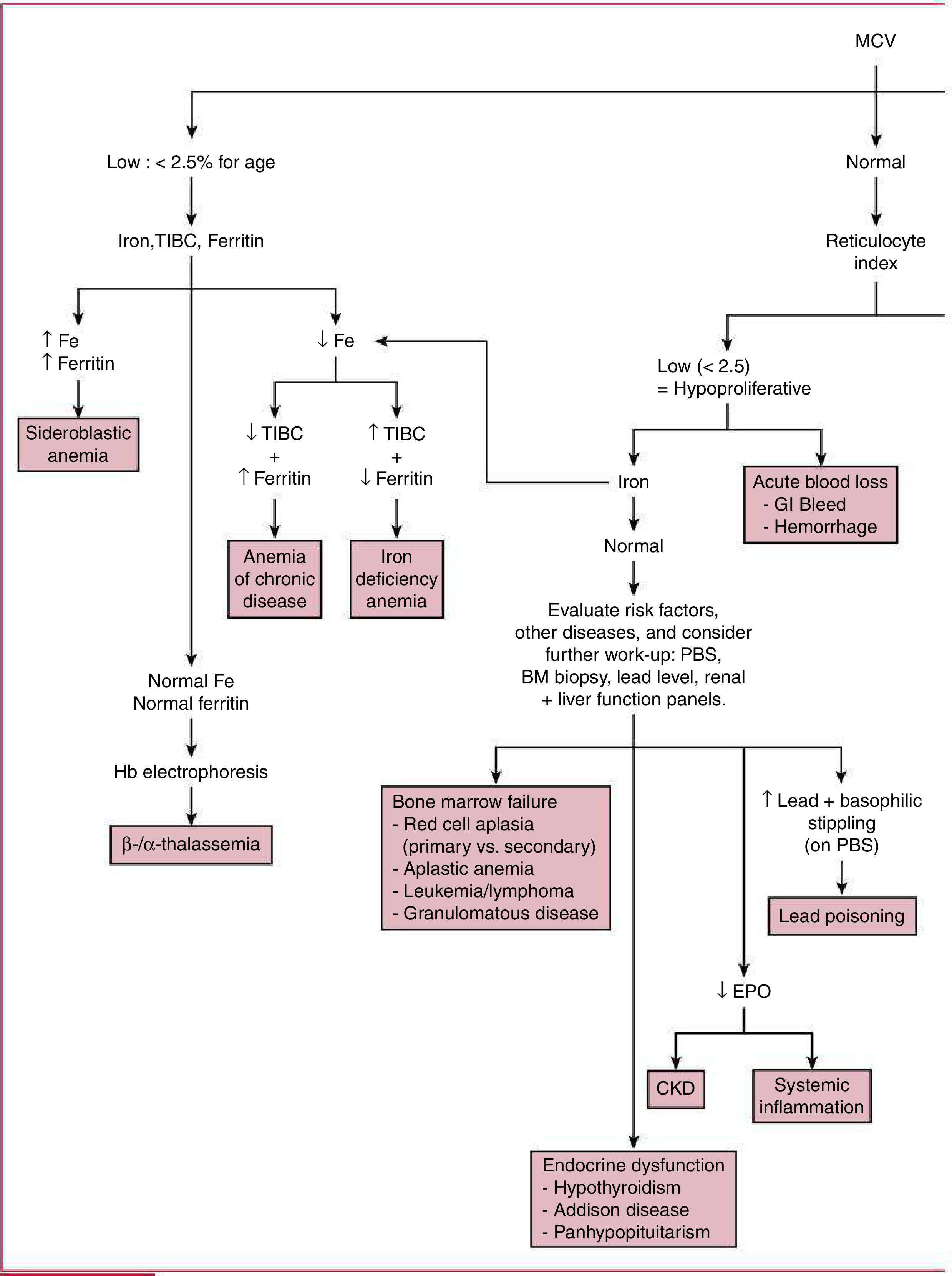
Approach to pediatric anemia based on MCV and reticulocyte index - Harriet Lane Handbook, 23rd ed., Fig. 14.1
This child should be followed up with an iron studies panel and, if IDA is confirmed, iron supplementation with dietary counseling. If the child does not respond to iron therapy in 4 weeks, thalassemia workup (Hb electrophoresis) should follow.
This is a shared conversation. Sign in to Orris to start your own chat.