Give me detail notes on Abdominal Tuberculosis for surgery subject for MBBS student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
I now have comprehensive content from Bailey & Love, S Das Manual on Clinical Surgery, and Sleisenger & Fordtran. I have enough to write detailed, well-structured MBBS surgery notes. Let me compile them now.
Abdominal Tuberculosis - Detailed Surgery Notes for MBBS
Sources: Bailey & Love's Short Practice of Surgery 28th Ed., S Das Manual on Clinical Surgery 13th Ed., Sleisenger & Fordtran's GI & Liver Disease
1. DEFINITION AND OVERVIEW
Abdominal tuberculosis (TB) refers to tuberculous infection of any organ within the abdominal cavity - the gastrointestinal tract, peritoneum, mesenteric lymph nodes, and solid organs (liver, spleen, pancreas). It is the commonest extra-pulmonary manifestation of TB.
- Accounts for 1-3% of all TB cases worldwide
- Abdomen is involved in approximately 11% of patients with extrapulmonary TB
- Incidence rising in resource-rich countries due to migration and immunosuppression (HIV)
- Mycobacterium avium intracellulare increasingly prevalent with HIV co-infection
2. CLASSIFICATION
Abdominal TB is broadly divided into two major types:
A. Intestinal Tuberculosis
- Ulcerative tuberculosis (terminal ileum)
- Hyperplastic ileocaecal tuberculosis (ileo-caecal region)
B. Tuberculosis of Mesenteric Lymph Nodes (Tabes mesenterica)
C. Tuberculous Peritonitis
- Wet ascitic type (90%)
- Dry plastic type
- Fibrous/Encysted type
3. ETIOLOGY AND PATHOGENESIS
Causative organism: Mycobacterium tuberculosis (human type) - most common; M. bovis (bovine type, via contaminated dairy) less common
Routes of infection:
| Route | Description |
|---|---|
| Direct mucosal penetration | Swallowed organisms in sputum (pulmonary TB) or contaminated food/milk |
| Haematogenous | Miliary spread from pulmonary focus |
| Direct extension | From adjacent affected organs (fallopian tubes, vertebrae) |
| Lymphatic | Via mesenteric lymphatics |
Site predilection: Ileocaecal region (75% of cases) - due to:
- Abundance of lymphoid follicles (Peyer's patches) in terminal ileum
- Relative stasis of intestinal contents
- Close contact with intestinal contents
Risk factors: HIV/AIDS, malignancies (especially lymphoma), glucocorticoid therapy, anti-TNF agents, malnutrition, poor socioeconomic status
4. PATHOLOGY
4.1 Intestinal Tuberculosis - Gross Appearances
The gross appearance is divided into 3 categories (Sleisenger):
- Ulcerative lesions (60%) - multiple superficial transverse ulcers
- Hypertrophic lesions (10%) - scarring, fibrosis, heaped-up mass; can mimic carcinoma
- Ulcerohypertrophic (30%) - combination of both
4.2 Ulcerative Type (Severe form)
- Results from inhalation of tubercle bacilli in sputum in a case of pulmonary TB (human type)
- Multiple ulcers at terminal ileum with transverse orientation (long axis of ulcer is transverse - important feature)
- Serosa overlying the ulcer becomes thickened - perforation is therefore unusual
- Healing leads to stricture formation with luminal narrowing
- Patient is usually a known case of pulmonary TB
4.3 Hyperplastic Type (Ileocaecal TB - when host resistance is stronger)
- Infection starts in lymphoid follicles and spreads to submucous and subserous planes
- Marked inflammatory reaction causing hyperplasia and thickening of terminal ileum wall
- Regional lymph nodes become matted along with involved terminal ileum and caecum - forming a lump
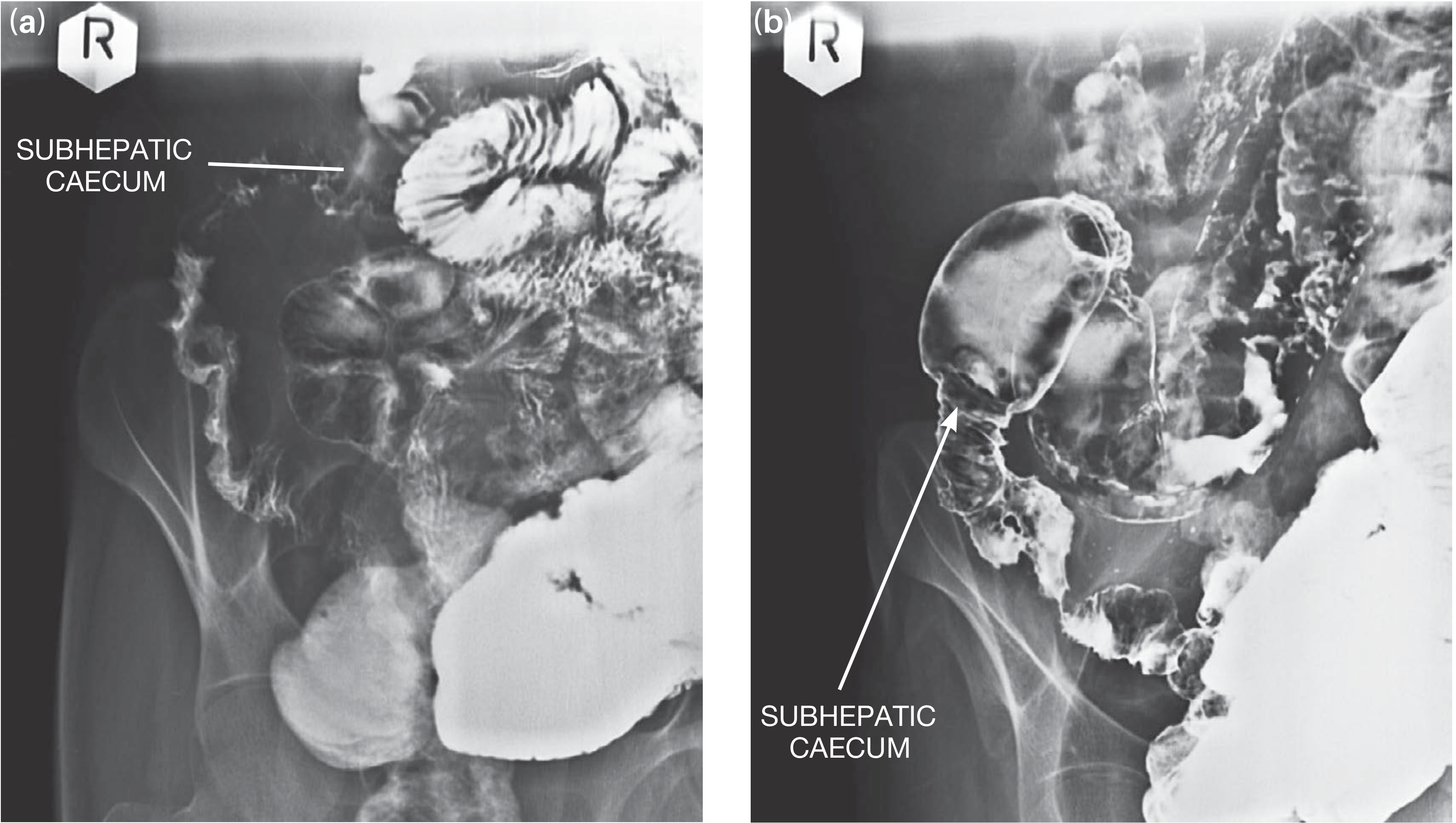
- As a result of fibrosis, shortening of bowel occurs with:
- Caecum pulled up into a subhepatic position
- Widening of the ileocaecal angle beyond 90°
- Lumen becomes narrowed - intestinal obstruction
- Macroscopically can be confused with Crohn's disease
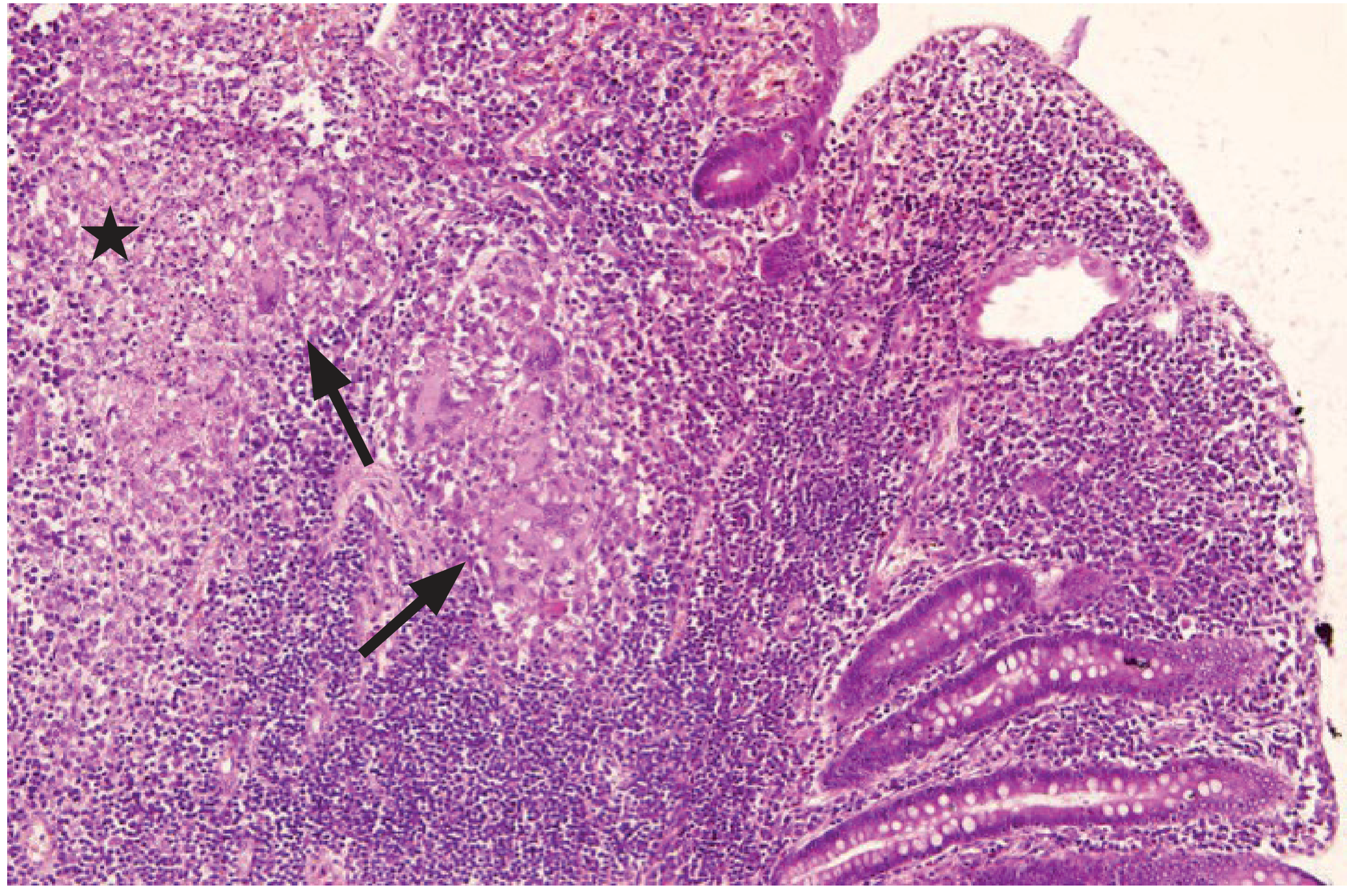
4.4 Histology
- Distinguishing lesion: caseating epithelioid cell granuloma with Langhans giant cells
- Seen in 50-80% of cases
- AFB detected by Ziehl-Neelsen stain in ~20% of mucosal samples
- PCR is more sensitive (~65%) on tissue or stool
4.5 Tuberculous Peritonitis
Spread to peritoneum occurs through:
- Gastrointestinal tract (typically ileocaecal region) via mesenteric lymph nodes
- Direct haematogenous spread (miliary form)
- Occasionally from cavitating pulmonary TB, lymphatics, or Fallopian tubes
- 50-80% of patients with abdominal TB have peritoneal involvement
Types of tuberculous peritonitis:
- Wet ascitic type (90%) - generalised or loculated ascites; multiple tubercle deposits on both peritoneal layers
- Dry plastic type - fibrotic fixed loops of bowel and omentum matted together; may present with subacute intestinal obstruction; ascites absent
- Fibrotic/Cocoon type - encasement of bowel loops in a fibrotic sac (abdominal cocoon); presents with obstruction
4.6 Tuberculosis of Mesenteric Lymph Nodes (Tabes Mesenterica)
- Rare, mainly seen in children
- Both human and bovine types enter mesenteric nodes through Peyer's patches
- Enlarged lymph nodes felt as firm, discrete, round nodules to the right of the umbilicus
5. CLINICAL FEATURES
5.1 Symptoms
| Symptom | Details |
|---|---|
| Abdominal pain | Most common (80-90%); nonspecific chronic pain; central constant discomfort |
| Weight loss | Due to malabsorption, malnutrition, systemic TB |
| Fever | Evening rise in temperature with sweating |
| Diarrhoea/Constipation | Alternating; fetid odour stools with pus and occult blood in ulcerative type |
| Abdominal distension | In peritonitis/ascites |
| Abdominal lump | Right iliac fossa mass in hyperplastic type (25-50% of patients) |
5.2 Signs
- Chronically ill patient with pallor, cachexia
- "Doughy" feel to abdomen - from areas of localised ascites (peritonitis)
- RIF mass in hyperplastic type - firm, irregular, variable mobility
- Slight tenderness in right iliac fossa (ulcerative type)
- In mesenteric TB: firm discrete nodules right of umbilicus
5.3 Presentations of Mesenteric TB
- Cause of abdominal pain - central constant discomfort, umbilical tenderness
- General symptoms only - weight loss, anorexia, pallor, evening fever
- Intestinal obstruction - coil of small intestine adherent to caseating node
- Indistinguishable from appendicitis - pain, vomiting, RIF tenderness
5.4 Emergency Presentations
- Distal small bowel obstruction from strictures (most common emergency presentation)
- Perforation - uncommon (serosa usually thick), but can occur even during treatment
- Peritonitis - may present acutely
6. INVESTIGATIONS
6.1 Blood Tests
- FBC: Mild anaemia with normal/mildly raised WBC
- ESR/CRP: Raised inflammatory markers
- Albumin: Low (hypoproteinaemia)
- Mantoux/Tuberculin skin test: May be positive (not always reliable)
- IFN-γ release assays (IGRA): For subclinical infection detection
6.2 Stool
- Occult blood (ulcerative type)
- AFB staining (low yield) - PCR more sensitive
6.3 Imaging
Chest X-ray:
- Pulmonary infiltration (though chest films may be normal in up to 50% of intestinal TB cases)
- Miliary pattern in haematogenous spread
Plain Abdominal X-ray:
- Features of small bowel obstruction: dilated jejunum (concertina/valvulae conniventes effect), featureless ileum with fluid between loops
Barium Meal and Follow-Through (very important examination):
- Ulcerative type: Non-filling or inadequate filling of terminal ileum, caecum and proximal ascending colon due to narrowing and hypermotility
- Hyperplastic type: Long narrow constricted terminal ileum with ascending colon; caecum in high (subhepatic) position
- String sign of Kantor in Crohn's disease (narrow, smooth terminal ileum) - helps differentiate
- Widened ileocaecal angle >90° in hyperplastic type
Ultrasonography:
- May show localised/generalized ascites
- Lymphadenopathy
- Thickened bowel loops
CT Abdomen:
- Diffuse thickening of peritoneum, mesentery and/or omentum
- Ascites (often loculated)
- Enlarged mesenteric lymph nodes
- Bowel wall thickening and strictures
6.4 Endoscopy (Colonoscopy with Biopsy)
Most useful diagnostic procedure - essential when TB is suspected:
- Mucosal biopsy for histopathology
- AFB staining/PCR
- Culture with drug sensitivities
- Typical appearances: transverse ulcers, deformed ileocaecal valve, both sides of ICV involved (incompetent valve - helps distinguish from Crohn's where only one side typically involved)
Note: Isolation masks required in endoscopy suite when TB is suspected
6.5 Ascitic Fluid Analysis (in peritoneal TB)
- Straw-coloured exudate
- Protein >25-30 g/L
- WBC >500/mL; Lymphocytes >40%
- AFB smear - often not diagnostic (low yield)
- Culture - takes 4-8 weeks
- Adenosine Deaminase (ADA) in ascitic fluid - high sensitivity and specificity for peritoneal TB
- Xpert MTB/RIF assay - value still being determined
6.6 Laparoscopy + Peritoneal Biopsy
- Couples typical macroscopic appearances (peritoneal tubercles) with histology
- Very helpful when ascitic fluid tests are inconclusive
7. DIFFERENTIAL DIAGNOSIS
For RIF Mass (Hyperplastic Type):
| Condition | Distinguishing Features |
|---|---|
| Crohn's Disease | Caecum in normal position (not elevated); "string sign of Kantor"; anal complications (fissures, fistulae common); no constitutional TB features |
| Carcinoma of Caecum | Elderly patient; hard irregular fixed lump; occult blood + rapid weight loss; no systemic TB features; barium: irregular filling defect in caecum with normal terminal ileum |
| Actinomycosis | Extremely hard, woody lump; multiple sinuses; sulfur granules in discharge |
| Amoebic Typhlitis | Primarily diarrhoea; rarely produces lump; endemic area; sigmoidoscopy helpful |
| Appendix mass | Acute onset history; tender; no systemic TB |
For Intestinal Obstruction:
- Other causes of small bowel obstruction (adhesions, hernias, volvulus)
For Peritonitis / Ascites:
- Malignant peritoneal carcinomatosis - distinction difficult, often requires biopsy
- Cirrhotic ascites
- Ovarian malignancy
8. COMPLICATIONS
- Intestinal obstruction (most common) - from strictures of terminal ileum/ascending colon
- Perforation - uncommon (thick serosa); can occur even during treatment
- Peritonitis - from perforation
- Fistula formation - enteroenteric, enterocutaneous
- Malabsorption - from obstruction leading to SIBO (small intestinal bacterial overgrowth)
- Gastrointestinal haemorrhage - from ulceration
- Abdominal cocoon (sclerosing encapsulating peritonitis) - encasement of bowel in fibrotic sac
- Caseating mesenteric nodes discharging through umbilicus to form sinus/fistula
9. TREATMENT
9.1 Medical Treatment (Primary Treatment)
Standard multidrug anti-tubercular therapy (ATT):
- Intensive phase (2 months): HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol)
- Continuation/Maintenance phase (4-10 months): HR (Isoniazid + Rifampicin)
- Total duration: 6-12 months (9-12 months commonly used for abdominal/extrapulmonary TB)
Important: Multidrug resistance may be higher for abdominal than for pulmonary TB
Supportive treatment:
- Nutritional support and hydrotherapy
- Correct anaemia
- Vitamin supplementation
Follow-up after completion of medical treatment:
- Reimaging of small bowel to look for significant strictures
- If features of subacute intermittent obstruction persist - surgical intervention planned
9.2 Surgical Treatment
Indications for surgery:
- Intestinal obstruction (acute or chronic/subacute) - from strictures
- Perforation
- Failure to respond to medical treatment
- Diagnostic uncertainty (to exclude malignancy)
- Abdominal mass requiring clarification
- Fistula formation
- Haemorrhage uncontrolled
Elective Surgical Options:
| Procedure | Indication |
|---|---|
| Limited ileocolic resection with anastomosis (terminal ileum + ascending colon) | Hyperplastic ileocolic disease (standard procedure) |
| Strictureplasty | Single ileal stricture (bowel-preserving) |
| Bowel resection | Multiple closely placed strictures |
| Right hemicolectomy | Extensive ileocolic disease |
Surgical principles in elective setting are very similar to those for Crohn's disease - resections should be kept as conservative as possible to preserve bowel length
Emergency Surgery (great challenge - these patients are very ill):
The emergency patient:
- Usually from poor socioeconomic background (late presentation)
- Extremely ill from dehydration, malnutrition, anaemia, and possibly active pulmonary TB
- Vigorous resuscitation precedes operation
Minimum life-saving procedure at laparotomy:
- Resection of diseased segment + proximal ileostomy + distal ileal/colonic mucus fistula (avoids anastomosis which has high leak risk in setting of active infection and poor general condition)
- If general condition permits (rarely): one-stage resection and anastomosis
Post-emergency surgery management:
- Combined care of physician and surgeon
- Full course of standard multidrug ATT (6-12 months)
- Nutritional rehabilitation
- Reassessment when disease no longer active (normalised inflammatory markers, weight gain, negative sputum culture)
- Then closure of stoma and reversal procedure if required
9.3 Management of Tuberculous Peritonitis
- Principally supportive (nutrition and hydration) + medical (systemic ATT)
- Surgery required for specific complications (intestinal obstruction, cocoon)
- Laparoscopy can be used for diagnosis (peritoneal biopsy)
- Thorough peritoneal lavage if needed
10. KEY COMPARISON: TB vs CROHN'S DISEASE
| Feature | Intestinal TB | Crohn's Disease |
|---|---|---|
| Site | Ileocaecal, both sides of ICV | Terminal ileum most common |
| Ileocaecal valve | Both sides involved - incompetent | Usually one side |
| Caecum position | Pulled up (subhepatic) | Normal position |
| Anal complications | Rare | Common (fissures, fistulae - 80%) |
| Barium | Narrow constricted terminal ileum + subhepatic caecum | String sign of Kantor, skip lesions |
| Histology | Caseating granuloma, AFB | Non-caseating granuloma, no AFB |
| Response to ATT | Responds | No response |
| AFB/Culture | May be positive | Negative |
| Endemic area | Yes | More in developed countries |
| Cobblestoning | Absent | Present on endoscopy |
11. QUICK EXAM SUMMARY
"Hot points" for MCQs and OSCEs:
- Most common site: ileocaecal region (terminal ileum + caecum)
- Most common form of peritoneal TB: wet ascitic type (90%)
- Ulcer orientation in intestinal TB: transverse (unlike carcinoma where it is along long axis)
- Perforation rare because: serosa is thickened
- Caecum in hyperplastic type is pulled to: subhepatic position with ICA >90°
- Differentiating feature from Crohn's: both sides of ileocaecal valve involved (incompetent ICV) in TB
- Best investigation for diagnosis: colonoscopy with biopsy (histology + culture)
- Specific ascitic fluid test: Adenosine deaminase (ADA) - high sensitivity for peritoneal TB
- Emergency surgery approach: resection + proximal ileostomy + mucus fistula (avoid anastomosis)
- Standard surgical approach in elective setting: conservative resection (ileocolic resection / strictureplasty)
- ATT duration: 6-12 months (intensive 2 months + continuation 4-10 months)
Sources: Bailey & Love's Short Practice of Surgery 28th Edition (Ch. 6), S Das Manual on Clinical Surgery 13th Edition (Ch. 34-35), Sleisenger & Fordtran's GI & Liver Disease (Ch. 110), Bailey & Love Tuberculous Peritonitis (Ch. 65)
This is a shared conversation. Sign in to Orris to start your own chat.