Laryngeal framework surgeries (thyroplasties) according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I have comprehensive material from both major ENT textbooks. Now I'll compile a thorough, well-structured answer.
Laryngeal Framework Surgery (Thyroplasty)
Historical Background
Laryngeal framework surgery was first described by Payr in 1915. The field was transformed by Nobuhiko Isshiki, who pioneered the use of alloplastic materials (Silastic), stressed performing the procedure under local anaesthesia to allow real-time voice feedback during surgery, and introduced the now-standard classification of four thyroplasty types.
The fundamental principle is that framework surgery modifies the glottic aperture, plane of vocal fold closure, and vocal fold length - all without invading the vocal fold itself, thereby preserving laryngeal dynamics and avoiding alterations in mass or stiffness of the folds.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 1034
- Cummings Otolaryngology Head and Neck Surgery, p. 1156
Isshiki Classification - Four Types
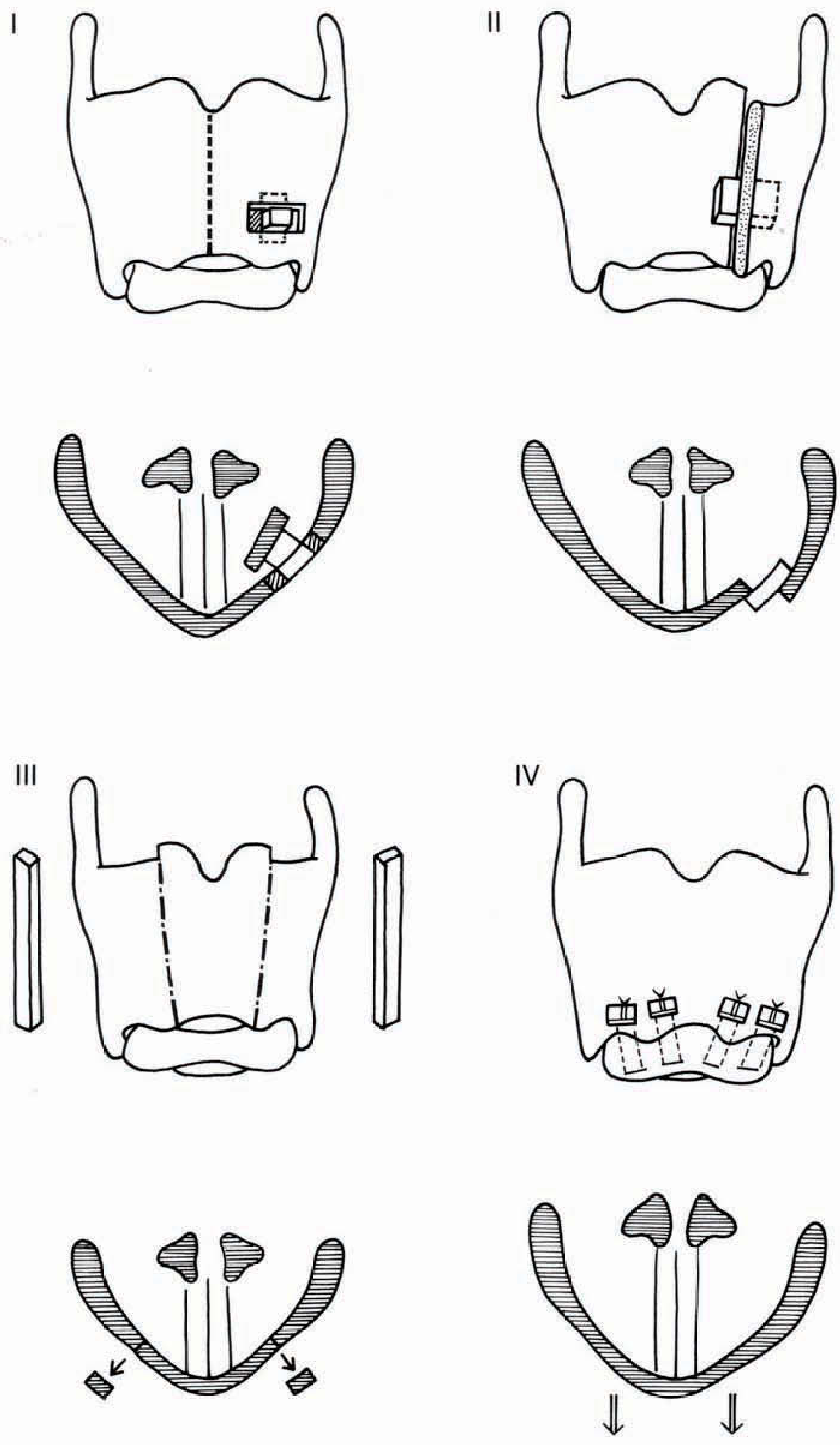
Figure: Isshiki Types I-IV laryngeal framework thyroplasties. Top row = frontal view of thyroid cartilage with implant placement; bottom row = cross-sectional view of glottis showing the resulting vocal fold position.
Type I - Medialization Thyroplasty
Purpose: Medialize (push inward) a paralyzed or laterally displaced vocal fold.
Mechanism: An implant is inserted through a rectangular window cut in the thyroid lamina into the paraglottic space, displacing the vocal fold medially without entering the laryngeal lumen.
Indications:
- Unilateral vocal fold paralysis (most common indication)
- Vocal fold bowing from presbylaryngis (aging)
- Cricothyroid joint fixation
- Sulcus vocalis
- Soft tissue defects after surgical excision
- Bilateral bowed vocal folds (bilateral procedure possible)
Patient selection timing: In idiopathic unilateral paralysis, waiting up to 12 months for spontaneous recovery is recommended. Injection laryngoplasty bridges the gap during this period. Thyroplasty is considered when recovery is unlikely or when dysphagia/severe dysphonia demands earlier intervention.
Favorable factors for framework surgery (over injection):
- Dysphagia
- High vocal demand or disability
- Poor functional prognosis
- Large glottic gap (2-3 mm)
- Posterior glottic gap
- Shortened life expectancy
Implant materials: Silastic (carved from block or prefabricated - Netterville/Montgomery systems), dense hydroxyapatite (VoCoM), expanded polytetrafluoroethylene (Gore-Tex strips). Gore-Tex has risk of granulomatous reaction and extrusion. All materials are biologically inert.
Advantages over injection laryngoplasty:
- Precise, predictable, and durable
- Reversible (implant can be repositioned or removed)
- Performed under local anaesthesia - patient voice guides surgeon intraoperatively
- Structural integrity of vocal fold preserved
- Prosthesis is lateral to inner perichondrium; vocal fold oscillation mechanics maintained
- Can be safer for high-risk patients than injection under general anaesthesia
Disadvantages:
- Open procedure with external incision
- Technically more demanding
- Closure of posterior glottis may be limited (arytenoid adduction often needed for posterior gap)
Anesthesia: Local anaesthesia with or without IV sedation. Patient phonation and endoscopic visualization guide implant sizing and positioning.
Window dimensions and location: A paramedian horizontal incision is made. The thyroid cartilage window is cut at the appropriate level - the "critical point" marking the inferior margin ensures the implant medializes the true vocal fold, not the ventricle. Poor results are classically due to the window being placed too superiorly.
Outpatient feasibility: Recent evidence shows Type I thyroplasty can be performed as an outpatient procedure in most cases. Hospital observation is warranted for: bilateral procedures, obstructive sleep apnoea, anticoagulation requiring bridging, and other high-risk comorbidities.
- Cummings, p. 1156-1157
Type II - Lateralization Thyroplasty
Purpose: Lateralize (push outward) one or both vocal folds to widen the glottic airway.
Mechanism: An implant is placed on the lateral aspect of the thyroid lamina to push the vocal fold away from the midline, increasing the airway lumen.
Indications:
-
Bilateral adductor spasmodic dysphonia (focal laryngeal dystonia) - reported effective for adductor spasmodic dysphonia
-
Bilateral vocal fold paralysis in adducted position causing airway obstruction (as an alternative to laser cordotomy or tracheotomy)
-
Respiratory distress from bilateral paralysis in near-midline position
-
Scott-Brown's, p. 1034; K.J. Lee's Essential Otolaryngology
Type III - Shortening (Relaxation) Thyroplasty
Purpose: Reduce vocal fold tension and length to lower the fundamental frequency (pitch) of the voice.
Mechanism: A vertical segment of the anterior thyroid cartilage is removed, allowing the thyroid laminae to slide together (be approximated anteriorly), reducing the antero-posterior diameter of the larynx and therefore reducing vocal fold tension and length.
Indications:
- Mutational falsetto (puberphonia/ventricular phonation) - to lower pitch
- Male-to-female gender-affirming voice correction in the reverse direction
- Spastic dysphonia (historically)
Type IV - Cricothyroid Approximation (Pitch-Raising Thyroplasty)
Purpose: Increase vocal fold tension and length to raise the fundamental frequency (pitch).
Mechanism: Sutures are placed to approximate (pull together) the cricoid and thyroid cartilages anteriorly, mimicking the action of the cricothyroid muscle. This stretches and tenses the vocal folds, raising pitch.
Indications:
- Female gender-affirming voice surgery (male-to-female transgender patients) - most common current use
- Raising pitch in patients with abnormally low voice
Adjunctive Procedures
Arytenoid Adduction (AAd)
Frequently combined with Type I thyroplasty, especially when there is a posterior glottic gap or a laterally displaced arytenoid that thyroplasty alone cannot correct.
Mechanism: A suture is placed through the muscular process of the arytenoid (the origin of the lateral cricoarytenoid muscle). Anterior traction on this suture internally rotates the arytenoid, displacing the vocal process medially - mimicking the action of the lateral cricoarytenoid (LCA) muscle. The suture is secured to the inferior cornu of the thyroid ala.
Adduction arytenoidopexy (less common alternative): The cricoarytenoid joint capsule is opened and the arytenoid is sutured directly to the cricoid crest in optimal phonatory position.
Evidence: Animal model research shows that combined arytenoid adduction + thyroplasty produces superior acoustic and aerodynamic results compared to thyroplasty alone in flaccid laryngeal paralysis. Two clinical studies have demonstrated significantly better posterior gap closure with the combined procedure.
Arytenoid Abduction (AAb)
Mimics the posterior cricoarytenoid (PCA) muscle - the sole abductor of the vocal fold. A suture in the muscular process applies posteroinferior traction, rotating the vocal process laterally and superiorly to open the airway.
Indications:
-
Bilateral laryngeal paralysis with airway obstruction
-
Unilateral paralysis with anterior arytenoid prolapse causing airway obstruction
-
Combined with AAd when the paralyzed arytenoid sags inferiorly (the abduction suture corrects the vertical position while adduction achieves medial closure)
-
Cummings, p. 1157-1158
Complications
| Complication | Notes |
|---|---|
| Airway obstruction | Most serious; medialization narrows the airway, compounded by postoperative oedema and haematoma |
| Laryngeal lumen perforation | Increases infection risk and implant extrusion |
| Suboptimal voice outcome | Most common complication; revision rates 5.4-14% (up to 33% when adjunctive fat injection included) |
| Implant malposition | Too anterior or too superior position; persistent posterior gap; under-medialization |
| Granulomatous reaction | Especially with Gore-Tex (PTFE); multinucleated giant cells reported |
| Implant extrusion | Known complication, particularly with Gore-Tex |
Common causes of poor voice results:
- Persistent posterior gap (most common technical failure)
- Under-medialization
- Implant in too anterior or too superior position
- Scott-Brown's, p. 1034; Cummings, p. 1157
Reinnervation Procedures
Reinnervation is an alternative or adjunct to framework surgery, best suited when the vocal fold is completely denervated (e.g., recurrent laryngeal nerve was sectioned - immediate re-anastomosis is treatment of choice at time of injury).
-
Ansa cervicalis-to-RLN anastomosis (Crumley) - most studied technique
-
Hypoglossal nerve - also studied
-
Reinnervation improves bulk and tone of vocal fold muscle but does not restore physiologic motion (due to complex innervation of intrinsic laryngeal muscles)
-
Symptom improvement may take weeks to months
-
Often combined with other rehabilitation techniques
-
Scott-Brown's, p. 1035
Summary Table - Isshiki Thyroplasty Classification
| Type | Name | Action | Main Indication |
|---|---|---|---|
| I | Medialization thyroplasty | Pushes vocal fold medially | Unilateral VF paralysis, bowing |
| II | Lateralization thyroplasty | Pushes vocal fold laterally | Bilateral adductor spasmodic dysphonia, bilateral paralysis in adducted position |
| III | Relaxation (shortening) thyroplasty | Reduces VF tension/length - lowers pitch | Mutational falsetto, excessive pitch |
| IV | Cricothyroid approximation | Increases VF tension/length - raises pitch | Gender-affirming voice surgery (MTF), abnormally low pitch |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 67, pp. 1034-1035
- Cummings Otolaryngology Head and Neck Surgery, Chapters 62-63, pp. 1156-1158
- K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.