Tracheoesophageal fistula 10 marks answer for ms ent
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive information to write a thorough 10-mark MS ENT answer. Let me compose it.
Tracheoesophageal Fistula (TEF) - 10 Mark Answer (MS ENT)
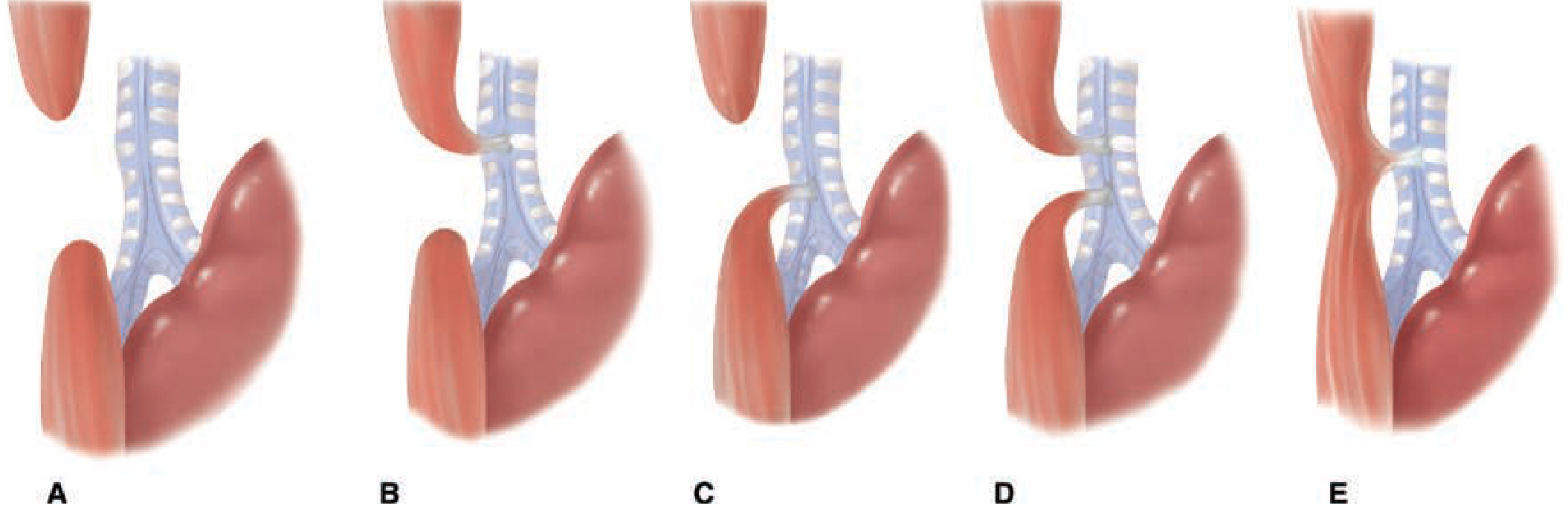
Fig: Five anatomical varieties of EA-TEF (Schwartz's Principles of Surgery)
Definition
A tracheoesophageal fistula (TEF) is an abnormal communication between the trachea and the esophagus. It may be congenital (the most common type, usually associated with esophageal atresia) or acquired (secondary to trauma, malignancy, or prolonged intubation/tracheostomy).
Embryology
The trachea and esophagus share a common embryologic origin from the primitive foregut. At approximately 4 weeks of gestation, the laryngotracheal groove forms as a diverticulum off the anterior aspect of the proximal foregut. This groove progressively deepens, with tracheoesophageal folds fusing in the midline to form the tracheoesophageal septum, thereby separating the trachea anteriorly from the esophagus posteriorly.
Failure of complete or proper fusion of these folds results in a defective tracheoesophageal septum, producing TEF - with or without associated esophageal atresia.
- Incidence: 1 in 3000-4500 live births; slight male predominance
- TEF is the most common birth defect of the lower respiratory tract
Classification (Gross-Vogt / Five Types)
| Type | Description | Incidence |
|---|---|---|
| A | Isolated esophageal atresia (EA) - no TEF | 8-10% |
| B | EA with proximal TEF (between proximal esophageal pouch and trachea) | ~1% |
| C | EA with distal TEF (blind upper pouch; lower esophagus connects to trachea near bifurcation) | ~85% - most common |
| D | EA with both proximal and distal TEF | ~2% |
| E (H-type) | TEF without EA; fistula connects trachea and esophagus in an H-shaped configuration | ~4-8% |
The H-type fistula is particularly important as it has no esophageal atresia and may present late with recurrent chest infections.
Associated Anomalies
Up to 50% of patients have other congenital anomalies. These are grouped under the VACTERL association:
- V - Vertebral anomalies
- A - Anorectal defects (imperforate anus)
- C - Cardiac defects (~38% - most common associated anomaly)
- TE - Tracheoesophageal fistula
- R - Renal anomalies (~15%)
- L - Limb defects (radial limb hypoplasia)
CHARGE syndrome is another association (Coloboma, Heart defects, Atresia choanae, Retarded growth, Genital abnormalities, Ear abnormalities).
Skeletal defects occur in ~19%, neurological defects in ~15%.
Clinical Features
Congenital TEF with EA (Types A-D)
Antenatal:
- Polyhydramnios (fetus cannot swallow amniotic fluid; no gastric filling)
- Failure to visualize the fetal stomach on ultrasound
Postnatal - classical triad:
- Excessive drooling/frothing from birth (accumulation of saliva in blind esophageal pouch)
- Choking and cyanosis with first feed - aspiration of milk
- Abdominal distension - air enters stomach via fistula during crying
Additional features:
- Repeated regurgitation and respiratory distress
- Chemical pneumonitis from reflux of gastric acid through distal TEF into lungs
- Inability to pass a nasogastric tube (coils in the upper pouch at ~10 cm from gum margin)
H-type TEF (Type E) - presents later
- Recurrent chest infections (aspiration pneumonia)
- Coughing/choking during feeds ("Oehlecker test" - positive coughing when methylene blue dye is injected into esophagus)
- Abdominal distension (borborygmi/gas)
- Subtle symptoms - may be diagnosed in later infancy or childhood
Acquired TEF
Caused by:
- Prolonged cuffed endotracheal/tracheostomy tube (pressure necrosis of the posterior "party wall" between trachea and esophagus, especially with concurrent large-bore NG tube)
- Esophageal or tracheal malignancy
- Trauma, foreign body, radiation necrosis
- Occurs in <1% of tracheostomies
Features: recurrent aspiration pneumonia, coughing when swallowing, ventilator air leak
Diagnosis
Neonatal (Types A-D)
- Inability to pass orogastric/nasogastric tube - tube coils at 10 cm; confirmed on chest X-ray (coiled tube in upper pouch)
- Plain chest X-ray:
- Coiled catheter in upper pouch
- Air in the stomach/GI tract = confirms distal fistula (Type C)
- Absent gastric air = isolated EA (Type A)
- Lung consolidation/collapse from aspiration
- Contrast esophagram (used cautiously) - documents the anatomy; risk of aspiration
- Echocardiography - to exclude cardiac anomalies (mandatory pre-operatively)
- Renal ultrasound, skeletal X-rays - screen for VACTERL anomalies
H-type TEF
- Barium esophagram (videofluoroscopy) - may miss small fistulas; H-type fistula typically runs obliquely (tracheal opening is superior to esophageal opening)
- Bronchoscopy + esophagoscopy - gold standard; methylene blue or Lipiodol injection into esophagus identifies the fistula opening in the trachea
Pre-operative Management
- Nurse in 30-45° head-up position to minimize aspiration
- Sump catheter (Replogle tube) on continuous suction in the upper pouch
- IV antibiotics - for aspiration pneumonia
- IV fluids / total parenteral nutrition
- Avoid positive pressure ventilation if possible (worsens gastric distension via fistula)
- If ventilation is essential - place ETT tip distal to fistula; use low-pressure ventilation
- Echocardiography - identify cardiac anomalies; determines operative approach (left-sided arch = right thoracotomy)
- Surgery is not a true emergency unless ventilation is impossible; aim for repair within 24-48 hrs of stabilization
Waterston's Waterston's risk classification (older system):
- Group A: >2.5 kg, healthy - low risk
- Group B: 1.8-2.5 kg, or mild pneumonia or moderate anomaly
- Group C: <1.8 kg, or severe pneumonia or severe cardiac anomaly - high risk
Surgical Treatment
Standard Repair (Type C - most common)
Approach: Right extrapleural thoracotomy (3rd or 4th intercostal space); video-assisted thoracoscopic surgery (VATS) is increasingly used
Steps:
- Identify and divide the azygos vein
- Identify and ligate/divide the fistula at its tracheal end (tracheal side closed with absorbable sutures)
- Mobilise proximal and distal esophageal pouches
- Primary end-to-end esophageal anastomosis
Long-gap EA (gap >3 cm or 2 vertebral bodies)
- Foker technique - external traction sutures to gradually elongate the esophageal stumps prior to anastomosis
- Gastric transposition or colonic/jejunal interposition - if primary anastomosis not possible
H-type TEF (Type E)
- Right cervical approach (fistula usually lies at C5-C7 level)
- Fistula is divided and both ends closed
- Alternatively, endoscopic obliteration with cauterization or trichloroacetic acid (especially for recurrent fistulas)
Acquired TEF (Post-tracheostomy)
- Interposition of viable muscle flap (sternohyoid, sternocleidomastoid, or strap muscles) between the repaired tracheal and esophageal defects
- Esophageal stenting as a temporizing measure in malignant TEF
Complications
Post-operative Complications
| Complication | Frequency/Notes |
|---|---|
| Anastomotic leak | 10-15%; major cause of morbidity |
| Anastomotic stricture | Most common long-term complication; treated with balloon dilatation |
| Gastroesophageal reflux disease (GERD) | Very common; disrupted lower esophageal sphincter |
| Recurrent TEF | ~5-10%; presents with recurrent aspiration |
| Tracheomalacia (TM) | Common; barking cough ("TOF cough"), episodic cyanosis ("dying spells") |
| Esophageal dysmotility | Long-term swallowing difficulty |
| Pulmonary complications | Only ~20% have normal pulmonary function at long-term follow-up (Helsinki study) |
Prognosis
- With modern neonatal surgical care, survival exceeds 90% in uncomplicated cases
- Mortality is determined mainly by severity of associated cardiac anomalies and degree of prematurity
- Long-term quality of life is good in most survivors, though GERD and dysmotility require ongoing management
Summary Points for MS ENT Exam
- Most common type = Type C (EA + distal TEF) - 85%
- Commonest presentation = excessive drooling, cyanosis with feeds, abdominal distension
- Key investigation = inability to pass NG tube + chest X-ray
- Approach = right extrapleural thoracotomy
- Operation = fistula ligation + primary esophageal anastomosis
- Most common long-term complication = anastomotic stricture + GERD
- H-type TEF = no EA, presents late, diagnosed by esophagoscopy/bronchoscopy, repaired via cervical approach
- Acquired TEF = most commonly from prolonged tracheostomy + NG tube (pressure necrosis of party wall)
Sources: Cummings Otolaryngology Head and Neck Surgery; Schwartz's Principles of Surgery 11e; The Developing Human - Clinically Oriented Embryology (Moore & Persaud); Cummings Otolaryngology (block2, block46)
This is a shared conversation. Sign in to Orris to start your own chat.