In detailed about Peripheral vascular disease, new guidelines and all classification all PVD , investigation and treatment in deailed , add images and other relevant things
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peripheral arterial disease" AND "guidelines"
Searching the Web
peripheral vascular disease 2024 2025 AHA ACC guidelines classification treatment
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
peripheral vascular disease Fontaine Rutherford WIfI classification images diagram 2024
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple textbooks, all classifications, imaging examples, and the latest 2024 guidelines. Let me compile the complete detailed response.
Peripheral Vascular Disease (PVD) - Comprehensive Review
Definition & Overview
Peripheral vascular disease (PVD) is a broad term encompassing all diseases of blood vessels outside the heart and brain - primarily affecting arteries, veins, and lymphatics of the extremities. The most clinically significant subset is Peripheral Artery Disease (PAD), defined as atherosclerotic narrowing or occlusion of arteries supplying the extremities (predominantly the lower limbs).
PAD affects approximately 14.5% of Americans age 70 and older (~4 million individuals). It carries profound systemic risk: patients with PAD have a 2-6x increased risk of cardiovascular death, myocardial infarction, and stroke compared to those without PAD. Diabetics are 15 times more likely to require amputation than non-diabetic PAD patients. - Goldman-Cecil Medicine, p. 765
Etiology and Pathophysiology
Primary Cause
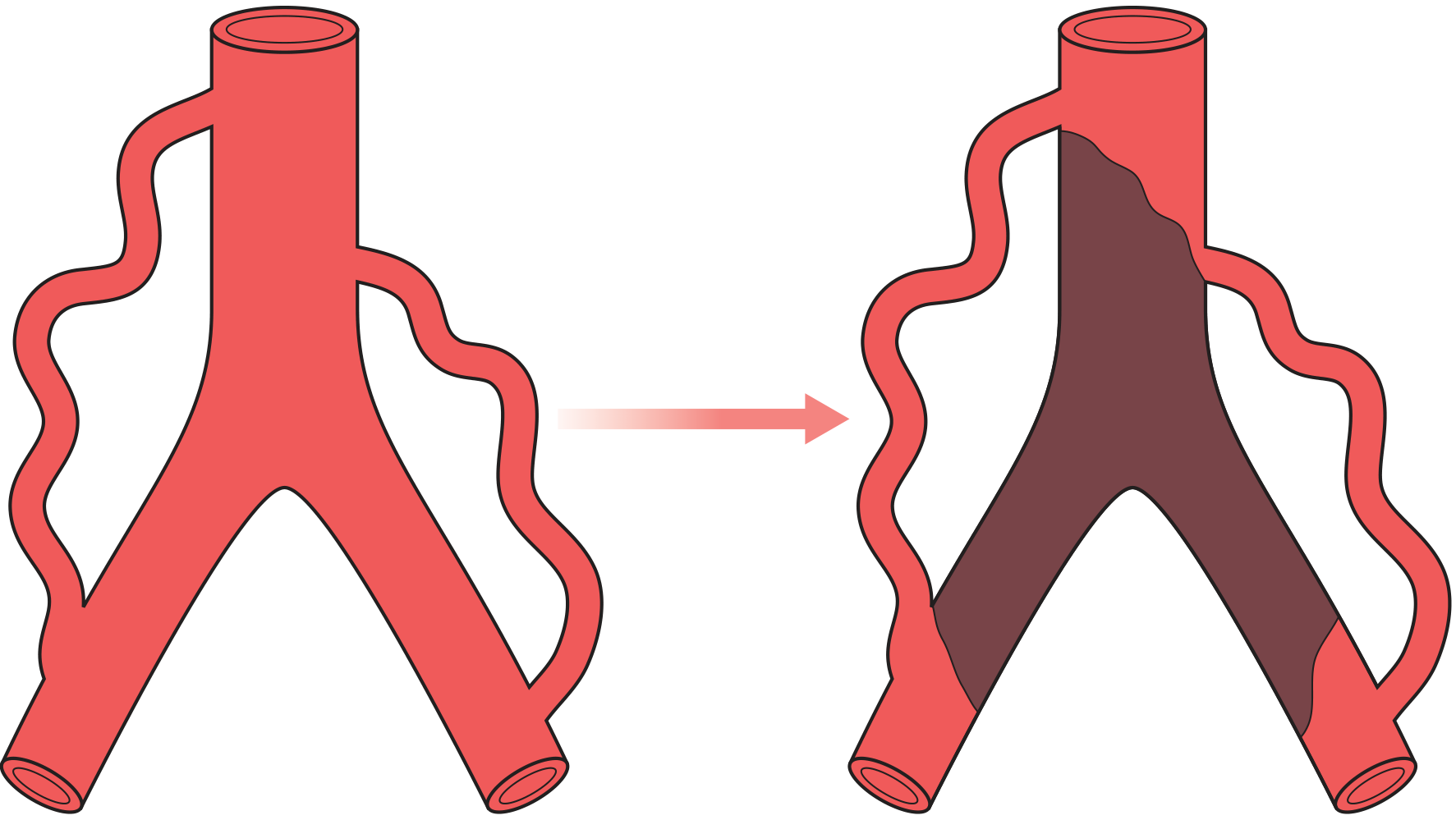
- Atherosclerosis (>90% of cases): lipid accumulation, foam cell formation, plaque development, fibrous cap, eventual stenosis/occlusion
Secondary and Non-Atherosclerotic Causes
| Category | Examples |
|---|---|
| Inflammatory/Autoimmune | Thromboangiitis obliterans (Buerger's), Takayasu's arteritis, giant cell arteritis |
| Thromboembolism | Cardiac emboli (atrial fibrillation, post-MI mural thrombus), aortic aneurysm cholesterol emboli |
| Structural | Popliteal entrapment syndrome, cystic adventitial disease |
| Vasospastic | Raynaud's phenomenon/disease |
| Venous | Chronic venous insufficiency, deep vein thrombosis, varicose veins |
| Lymphatic | Lymphedema (primary/secondary) |
Risk Factors for PAD
- Smoking (strongest modifiable risk factor; severity correlates with pack-years)
- Diabetes mellitus
- Hypertension
- Hyperlipidemia / elevated LDL
- Age >50 years
- Male sex (though women with PAD often present atypically)
- Chronic kidney disease / ESRD
- Elevated homocysteine (~1 in 3 PAD patients)
- Elevated C-reactive protein (inflammation drives atherosclerosis)
- Positive family history (heritability ~20%)
Spectrum of PVD - Major Categories
PERIPHERAL VASCULAR DISEASE
├── Arterial Disease (PAD)
│ ├── Chronic Stable (Claudication)
│ ├── Chronic Limb-Threatening Ischemia (CLTI)
│ └── Acute Limb Ischemia (ALI)
├── Venous Disease
│ ├── Chronic Venous Insufficiency
│ ├── Deep Vein Thrombosis
│ └── Varicose Veins
└── Lymphatic Disease
└── Lymphedema
Classification Systems
1. Fontaine Classification (1954) - Chronic PAD
| Stage | Clinical Findings |
|---|---|
| I | Asymptomatic |
| IIa | Mild claudication (symptoms >200 m walking distance) |
| IIb | Moderate-severe claudication (symptoms <200 m) |
| III | Ischemic rest pain, mostly in feet |
| IV | Necrosis and/or gangrene of the limb |
Fontaine is symptom-based only and lacks objective criteria.
2. Rutherford Classification (1986, revised) - Chronic Limb Ischemia
| Grade | Category | Clinical Findings | Objective Criteria |
|---|---|---|---|
| 0 | 0 | Asymptomatic | Normal treadmill or reactive hyperemia test |
| I | 1 | Mild claudication | Completes treadmill; post-exercise ankle pressure >50 mmHg but ≥20 mmHg below resting |
| I | 2 | Moderate claudication | Between categories 1 and 3 |
| I | 3 | Severe claudication | Cannot complete treadmill; post-exercise ankle pressure <50 mmHg |
| II | 4 | Ischemic rest pain | Resting ankle pressure <40 mmHg; toe pressure <30 mmHg |
| III | 5 | Minor tissue loss (non-healing ulcer, focal gangrene) | Resting ankle pressure <60 mmHg; toe pressure <40 mmHg |
| III | 6 | Major tissue loss (above transmetatarsal level) | Same as category 5 |
Rutherford adds objective hemodynamic criteria, making it more precise than Fontaine.
- Current Surgical Therapy 14e, p. 1142
3. Rutherford Classification - Acute Limb Ischemia (ALI)
| Grade | Category | Sensory Loss | Motor Deficit | Arterial Doppler | Venous Doppler | Prognosis |
|---|---|---|---|---|---|---|
| I | Viable | None | None | Audible | Audible | No immediate threat |
| IIA | Marginally threatened | None or minimal (toes only) | None | Inaudible | Audible | Salvageable if promptly treated |
| IIB | Immediately threatened | More than toes | Mild/moderate | Inaudible | Audible | Salvageable with immediate revascularization |
| III | Irreversible | Profound/insensate | Paralyzed (major) | Inaudible | Inaudible | Limb irreversibly damaged - amputation |
Grade III ALI = primary amputation, no revascularization.
- Bailey & Love's Surgery 28e, p. 1033
4. WIfI Classification (SVS, 2014) - Chronic Limb-Threatening Ischemia
The Wound, Ischemia, and foot Infection (WIfI) classification addresses the three critical pillars determining amputation risk and need for revascularization:
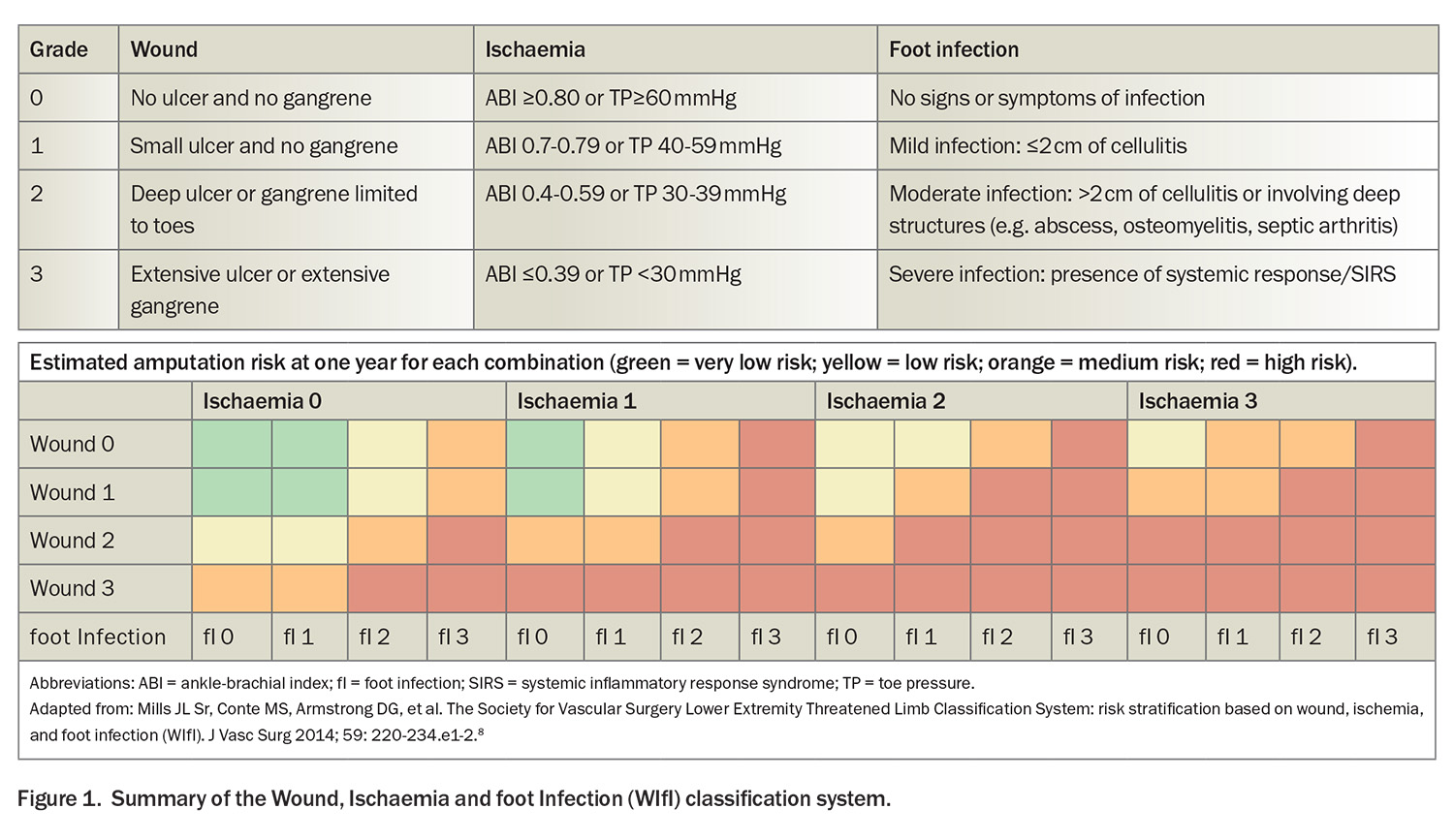
Each domain is graded 0-3:
- Wound (W): 0=no ulcer/gangrene, 1=small ulcer, 2=deep ulcer/toe gangrene, 3=extensive ulcer/gangrene
- Ischemia (I): 0=ABI ≥0.80, 1=ABI 0.70-0.79, 2=ABI 0.40-0.59, 3=ABI ≤0.39
- foot Infection (fI): 0=none, 1=mild (≤2 cm cellulitis), 2=moderate (deep structures involved), 3=severe (SIRS present)
The combination of all three scores predicts 1-year amputation risk (very low to high) and guides revascularization decisions. Endorsed by the 2024 ACC/AHA PAD Guidelines as the preferred risk stratification tool for CLTI.
5. TASC II Classification - Anatomic Distribution (Aortoiliac & Femoropopliteal)
| Type | Aortoiliac | Femoropopliteal | Management |
|---|---|---|---|
| A | Short stenoses ≤3 cm, unilateral or bilateral CIA | Single stenosis ≤10 cm or occlusion ≤5 cm | Endovascular preferred |
| B | Infrarenal aortic stenosis, short CIA/EIA lesions | Multiple lesions, single stenosis ≤15 cm | Endovascular preferred |
| C | Bilateral CIA/EIA, unilateral EIA occlusion | Multiple stenoses/occlusions >15 cm, recurrent post-stent | Surgery preferred |
| D | Chronic total aortic occlusion, diffuse bilateral disease | Complete CFA/SFA occlusion, total popliteal occlusion | Surgery preferred |
Clinical Presentation
Symptomatic Spectrum
1. Asymptomatic PAD
- ABI <0.9 but no symptoms (most common presentation - ~50% of cases)
- Still carries full cardiovascular risk
2. Intermittent Claudication (IC)
- Reproducible cramping, aching, or fatigue in muscle groups during exercise, relieved within 2-5 minutes of rest
- Calf claudication = femoropopliteal disease
- Buttock/thigh claudication = aortoiliac disease (Leriche syndrome: bilateral buttock claudication + impotence)
- Must be distinguished from pseudo-claudication (neurogenic - spinal stenosis): pain on standing, relieved by bending forward, not purely by rest
3. Chronic Limb-Threatening Ischemia (CLTI)
- Rest pain (typically worse at night, relieved by hanging leg down)
- Ischemic ulcers (punched-out, painful, on tips of toes/pressure areas, no granulation tissue)
- Gangrene
4. Acute Limb Ischemia (ALI)
The "6 P's":
- Pain (severe, sudden onset)
- Pallor
- Pulselessness
- Parasthesia (numbness)
- Paralysis (late, ominous sign)
- Perishing cold (poikilothermia)
Causes: Embolism (cardiac source in AF/post-MI) vs. thrombosis in-situ (pre-existing stenosis + plaque rupture)
Investigations
Non-Invasive Vascular Studies
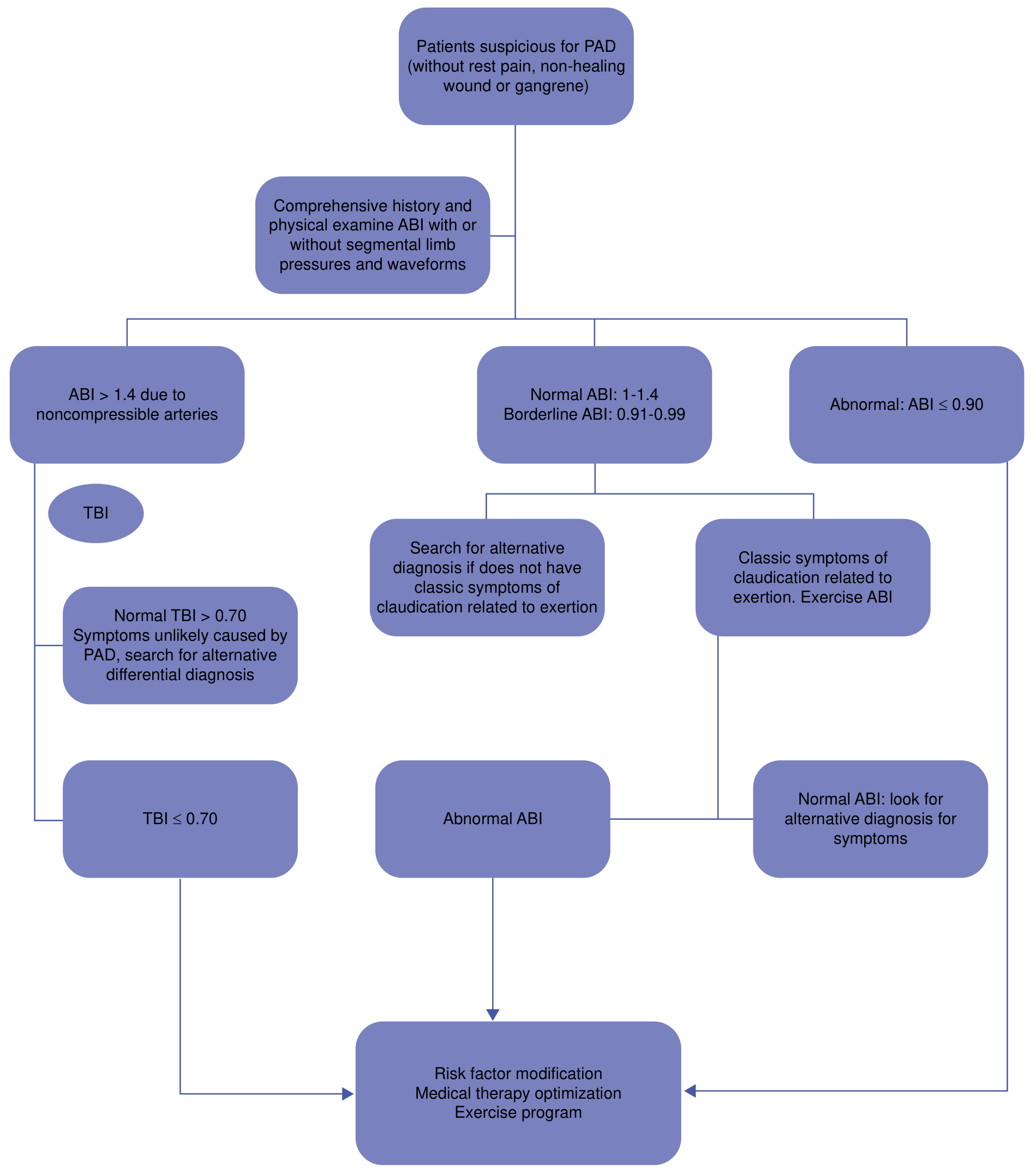
1. Ankle-Brachial Index (ABI) - First-line investigation
| ABI Value | Interpretation |
|---|---|
| >1.40 | Non-compressible (calcified vessels - seen in DM, ESRD); use TBI instead |
| 1.00 - 1.40 | Normal |
| 0.91 - 0.99 | Borderline |
| ≤0.90 | Diagnostic of PAD |
| <0.50 | Severe disease |
| <0.30 | Threatened limb |
Technique: Highest ankle pressure (DP or PT) ÷ higher brachial pressure = ABI. Use continuous-wave Doppler.
2. Toe-Brachial Index (TBI)
- Used when ABI is falsely elevated (non-compressible arteries in DM/CKD)
- Normal TBI: 0.70-0.80
- Minimum toe pressure for wound healing: 30 mmHg (40 mmHg in diabetics)
- Diagnostic of PAD: TBI <0.70
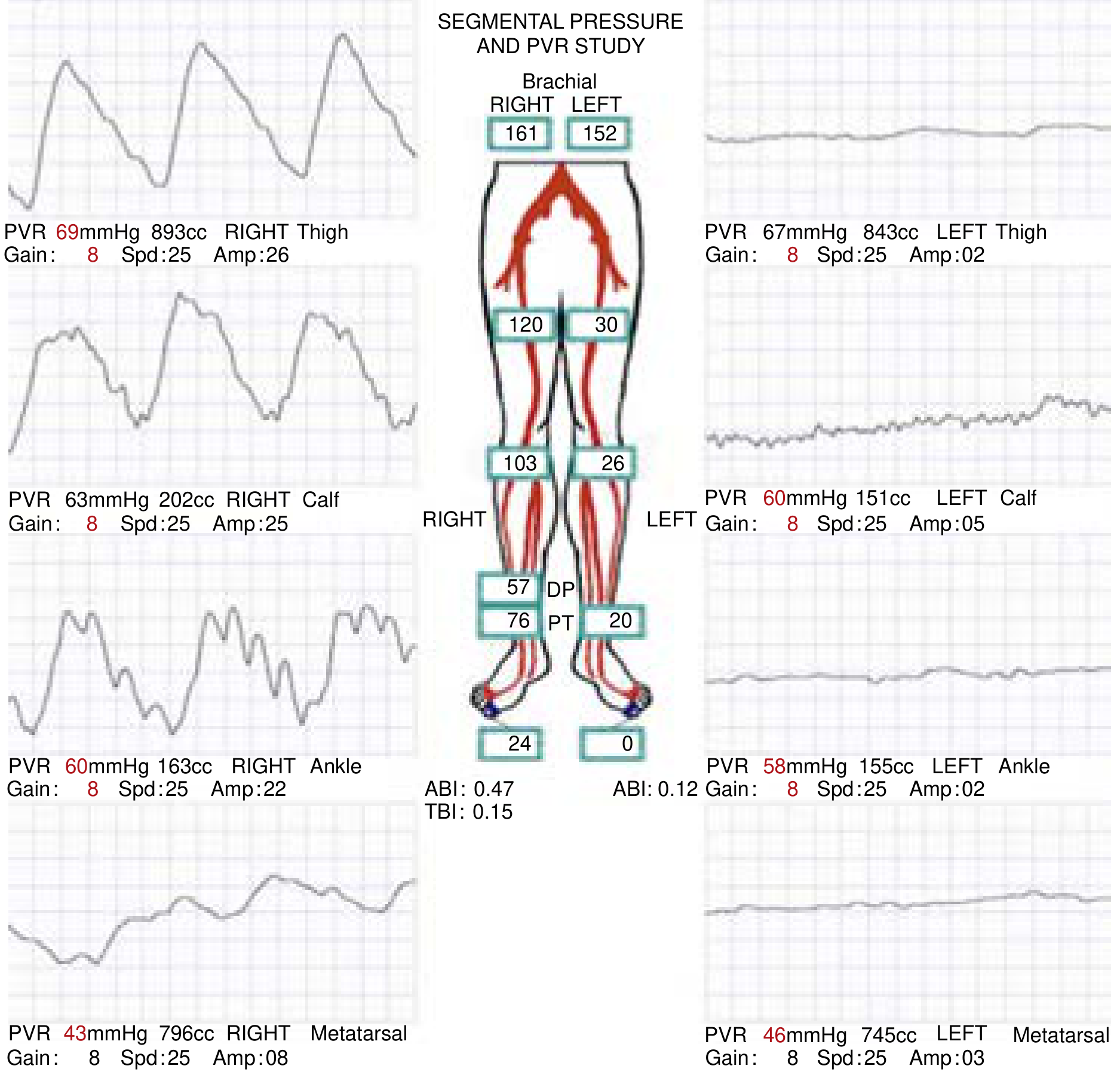
3. Segmental Limb Pressures
- Pressure cuffs at thigh, calf, ankle
- Gradient >20 mmHg between adjacent segments = significant stenosis
- Localizes level of disease
4. Pulse Volume Recordings (PVR)
- Plethysmographic waveform analysis at each segment
- Normal = triphasic; PAD = biphasic, then monophasic, then flat
5. Exercise ABI
- Standard protocol: 3.2 km/hr at 12% incline for 5 minutes
- Post-exercise ABI drop >20% = significant PAD
- Useful when resting ABI is normal but symptoms are classic
6. Duplex Ultrasound
- Combines B-mode imaging + Doppler velocity
- Sensitivity/specificity >90% for ≥50% stenosis
- Peak systolic velocity ratio >2.0 = >50% stenosis
- First-line for surveillance of bypass grafts and stents
Imaging
7. Computed Tomography Angiography (CTA)

- Requires iodinated IV contrast + ionizing radiation
- Excellent visualization of stents and calcified plaque
- ~1/4 radiation of DSA
- Faster and easier than MRA
8. Magnetic Resonance Angiography (MRA)
- No ionizing radiation; gadolinium contrast (avoid in GFR <60 - risk of nephrogenic systemic fibrosis)
- Cannot be used with ferromagnetic implants (pacemakers, ICDs)
- Tends to overestimate stenosis at vessel ostia (turbulent flow artifact)
- Better soft tissue contrast than CTA
9. Digital Subtraction Angiography (DSA)
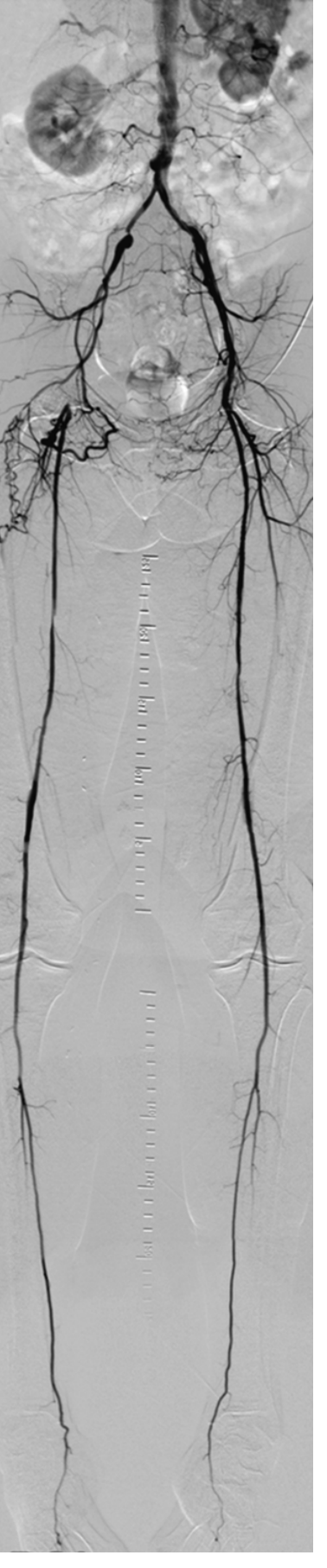
- Gold standard for diagnosis and pre-procedural planning
- Allows concurrent intervention (angioplasty/stenting)
- Complications: contrast allergy 0.1%, access-site bleeding, contrast-induced nephropathy
- Reserved for pre-intervention planning or when non-invasive imaging is inconclusive
PAD Diagnosis Algorithm
Laboratory Tests
- CBC (anemia, polycythemia)
- Lipid panel (LDL-C target <70 mg/dL in established PAD)
- HbA1c and fasting glucose (diabetes screen/monitoring)
- BMP/CMP (renal function - contrast planning)
- Coagulation studies (PT, PTT, INR)
- Homocysteine (elevated in ~33% of PAD patients)
- CRP / ESR (inflammation markers)
- Hypercoagulable workup (if young patient, atypical presentation, or bilateral disease without typical risk factors)
2024 ACC/AHA Guidelines - Key Updates
The 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline (published June 2024, Circulation) represents the most comprehensive update in nearly a decade:
Major New Recommendations
1. Screening (Class I)
- ABI screening recommended for patients >65 years, or >50 years with DM + smoking history
- Women with PAD often present atypically - sex-aware screening emphasized
- New: "Risk Amplifiers" table including CKD, ESRD, history of prior MACE
2. Antiplatelet Therapy (Class I)
- Aspirin 75-325 mg/day OR clopidogrel 75 mg/day for symptomatic PAD
- NEW - Rivaroxaban 2.5 mg BID + Aspirin 100 mg/day: Class I recommendation for patients with symptomatic PAD, based on the COMPASS trial (27% reduction in MACE + MALE)
- Single antiplatelet still preferred over DAPT for claudication alone
3. Supervised Exercise Therapy (Class I - strongest evidence)
- 3 sessions/week × 12 weeks of supervised exercise
- Effect size rivals or exceeds stenting for claudication
- Must be prescribed before or alongside revascularization for claudication
4. Statin Therapy (Class I)
- High-intensity statin for all PAD patients regardless of LDL
- LDL-C goal <70 mg/dL for CLTI; consider PCSK9 inhibitors if not achieved
5. CLTI Management (WIfI-driven)
- WIfI score mandated before revascularization decisions
- Multidisciplinary team-based care (vascular surgeon, podiatrist, wound care, endocrinologist)
- Revascularization should aim to restore "straight-line pulsatile flow" to the foot
6. Foot Care (New Section)
- Structured foot inspection at every visit for all PAD patients
- Footwear assessment and patient education
7. 2024 ESC Guidelines (September 2024, Eur Heart J, PMID 39210722)
- Align largely with ACC/AHA
- Emphasize rivaroxaban + aspirin for LEAD (lower extremity artery disease) with high ischemic/low bleeding risk
- Recommend CTA or MRA as first-line imaging (before DSA)
Treatment
A. Medical (Guideline-Directed Therapy)
1. Smoking Cessation (Class I - strongest recommendation)
- Single most effective intervention to slow PAD progression
- Bupropion and varenicline improve abstinence rates
- Reduces mortality, limb loss, and graft failure
2. Antiplatelet Agents
- Aspirin 75-325 mg/day
- Clopidogrel 75 mg/day (equal or superior to aspirin; preferred in aspirin intolerance)
- Rivaroxaban 2.5 mg BID + Aspirin 100 mg (2024 ACC/AHA Class I for symptomatic PAD without high bleeding risk - COMPASS/VOYAGER PAD evidence)
- Ticagrelor: no proven advantage over clopidogrel in EUCLID trial
3. Statins
- High-intensity (atorvastatin 40-80 mg or rosuvastatin 20-40 mg)
- LDL goal <70 mg/dL; add ezetimibe or PCSK9 inhibitor if needed
- Additional benefit: increases claudication walking distance (2 independent trials)
4. Antihypertensive Therapy
- Target BP <130/80 mmHg
- ACE inhibitors preferred (ramipril: 25% reduction in cardiac events in PAD patients)
- Beta-blockers: previously feared to worsen claudication - disproven in RCT; safe to use
5. Diabetes Management
- HbA1c goal <7.0% (SVS guidelines)
- SGLT2 inhibitors and GLP-1 agonists have additional cardiovascular benefit
6. Pharmacotherapy for Claudication
| Drug | MOA | Dose | Notes |
|---|---|---|---|
| Cilostazol (FDA-approved) | PDE-III inhibitor; vasodilation + antiplatelet | 100 mg BID | Contraindicated in heart failure; improves walking distance ~40-50% |
| Pentoxifylline (FDA-approved) | Reduces blood viscosity + platelet aggregation | 400 mg TID (max 1800 mg/day) | Modest effect; SE: nausea, headache |
7. Homocysteine
- Folic acid + B12 lowers homocysteine levels, but no RCT evidence for reduction in cardiovascular events
B. Supervised Exercise Therapy
- 3 sessions/week for 12 weeks minimum (ideally 26 weeks)
- Walking until claudication onset → rest → resume
- Improves walking distance, functional capacity, and quality of life
- Class I, Level A evidence in 2024 ACC/AHA guidelines
- Effect rivals endovascular revascularization for claudication (CLEVER trial: exercise = stenting for quality of life at 18 months)
C. Endovascular Revascularization
Indications
- Claudication: failed ≥3 months of medical + exercise therapy AND lifestyle-limiting symptoms
- CLTI: urgent; preferred when anatomy suitable
- ALI: emergent (onset <14 days preferred over open surgery)
Endovascular Procedures
| Procedure | Description | Best For |
|---|---|---|
| Balloon angioplasty (PTA) | Balloon inflated to compress plaque | Short stenoses; adjunct to stenting |
| Stenting | Bare metal or nitinol self-expanding stent | Aortoiliac (TASC A/B); SFA |
| Drug-coated balloon (DCB) | Paclitaxel-coated balloon; reduces restenosis | SFA and popliteal lesions |
| Drug-eluting stent (DES) | Everolimus/paclitaxel-eluting | Improving outcomes in SFA |
| Atherectomy | Plaque removal (rotational, laser, directional) | Heavily calcified lesions |
| Thrombolysis (intra-arterial) | rtPA 0.05-0.1 mg/kg/hr intra-arterially | ALI <14 days; native artery/graft thrombosis |
| Mechanical thrombectomy | Aspiration catheter | ALI; adjunct to thrombolysis |
| Venous arterialization | Reverses flow in veins to bypass occluded arteries | "No-option" CLTI (no bypass targets) |
D. Open Surgical Revascularization
Indications
- TASC C/D lesions (complex, long segment)
- Failed endovascular procedures
- ALI >14 days (surgical thrombectomy)
- High surgical risk anatomy unsuitable for endovascular
Bypass Surgery Options
| Bypass | Conduit | Best Outcomes |
|---|---|---|
| Aortobifemoral bypass | Dacron/PTFE | Aortoiliac occlusive disease |
| Femoro-popliteal bypass | Great saphenous vein (GSV) preferred | Above/below knee popliteal targets |
| Femoro-tibial bypass | GSV preferred; PTFE with vein cuff | CLTI with tibial artery targets |
| Axillo-femoral bypass | PTFE | High-risk patients, infected aorta |
GSV remains the best conduit for infrainguinal bypass; 5-year patency ~60-75% for below-knee bypass.
Amputation
- Class III ALI (irreversible ischemia)
- Unreconstructable CLTI with uncontrolled infection/sepsis
- Levels: digital → transmetatarsal → below-knee (BKA) → above-knee (AKA)
- Early rehabilitation with prosthesis is the goal
E. Treatment by Clinical Syndrome - Summary
| Clinical State | Priority | Key Interventions |
|---|---|---|
| Asymptomatic PAD | Cardiovascular risk reduction | Statin, antiplatelet, BP control, smoking cessation |
| Claudication | QoL improvement | Exercise therapy first (12 weeks) → cilostazol → consider revascularization if lifestyle-limiting |
| CLTI | Limb salvage | Urgent revascularization; WIfI scoring; wound care; MDT |
| ALI Grade I-IIB | Emergency limb salvage | Anticoagulation (UFH) immediately → endovascular (<14 days) or surgical (>14 days) |
| ALI Grade III | Prevent systemic complications | Primary amputation; beware reperfusion injury, rhabdomyolysis, compartment syndrome |
Complications and Prognosis
- Cardiovascular mortality: Leading cause of death in PAD (MI, stroke)
- Limb loss: 1-year major amputation rate in CLTI ~20-25%
- Reperfusion injury: After revascularization in ALI - compartment syndrome, rhabdomyolysis, hyperkalemia, renal failure
- Graft failure: 30-40% of femoro-popliteal bypasses occlude within 5 years
- Restenosis: Major limitation of endovascular therapy (10-40% within 1 year for SFA stenting)
Recent Evidence (2024-2025)
| PMID | Study | Finding |
|---|---|---|
| 38743805 | 2024 ACC/AHA PAD Guideline | Rivaroxaban + aspirin Class I; WIfI mandated; exercise therapy prioritized |
| 39210722 | 2024 ESC Peripheral & Aortic Disease Guidelines | Updated European guidance including upper extremity PAD, mesenteric ischemia |
| 40316185 | SVS 2025 Focused Update: Intermittent Claudication | Updated evidence for endovascular vs exercise for claudication |
| 39474992 | Cochrane 2024: Toe-brachial index | TBI highly accurate for PAD diagnosis, particularly in non-compressible ABI patients |
Key Pearls for Clinical Practice
- ABI is the cornerstone - measure in any patient with leg symptoms, DM over 50, or age over 65
- ABI >1.40 in diabetics/ESRD → get TBI instead (non-compressible arteries give false normal reading)
- Exercise therapy before stenting for claudication - equal or better outcomes in multiple trials
- Rivaroxaban 2.5 mg BID + aspirin is now Class I for symptomatic PAD in the 2024 guidelines
- Rutherford Grade III ALI (sensory + motor loss + no Doppler signals) = go straight to amputation - no angiography
- WIfI score before every CLTI revascularization decision
- Cilostazol is contraindicated in heart failure (any class) - important prescribing restriction
- Women with PAD often present without classic claudication - lower threshold for ABI testing
- Buerger's disease (thromboangiitis obliterans): young male smokers, distal involvement, no atherosclerosis risk factors - complete smoking cessation is the only proven therapy
Sources: Current Surgical Therapy 14e; Goldman-Cecil Medicine; Fuster & Hurst's The Heart 15e; Bailey & Love's Surgery 28e; 2024 ACC/AHA PAD Guideline (PMID 38743805); 2024 ESC Guidelines (PMID 39210722); 2025 SVS Claudication Update (PMID 40316185)
This is a shared conversation. Sign in to Orris to start your own chat.