Pathophysiology of foreign body in bronchus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"foreign body" AND "bronchus" AND pathophysiology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough answer. Here is a comprehensive breakdown:
Pathophysiology of Foreign Body in Bronchus
1. Why the Right Bronchus?
The right main bronchus is involved more frequently (approximately 60% of cases) than the left (30%), with the remainder in the trachea or larynx. This is explained by the anatomy:
-
The right main bronchus is wider in diameter and takes a more vertical, straighter course from the trachea compared to the left
-
The left main bronchus diverts at a sharper angle
-
This anatomical relationship is established from fetal development and persists into adult life
-
The Developing Human: Clinically Oriented Embryology, p. 810; K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology
2. Degrees of Bronchial Obstruction - The Key Mechansim
The pathophysiology depends entirely on the degree of airway occlusion produced by the foreign body. Three classic patterns exist:
A. Bypass (Partial, Bidirectional) Obstruction
Air can flow both in and out around the object. This produces:
- Mild cough and wheeze
- No major air trapping early on
- Mucosal irritation and inflammation at the site of contact
B. Check-Valve (Ball-Valve / Obstructive Emphysema) Mechanism
This is the most pathophysiologically important and clinically recognizable pattern.
Mechanism:
- On inspiration: the intrathoracic pressure decreases, which dilates the bronchial lumen, allowing air to flow past the foreign body into the distal lung
- On expiration: the intrathoracic pressure increases, compressing the bronchial wall around the foreign body, effectively sealing the airway and trapping the inhaled air
Result: Progressive air trapping and obstructive (hyperinflation) emphysema of the ipsilateral lung. The affected lung cannot empty - it becomes hyperinflated while the contralateral lung remains normal.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, p. 431-432
This ball-valve effect is what produces the characteristic chest X-ray findings (see below).
C. Stop-Valve (Complete Obstruction) / Atelectasis Mechanism
- Total occlusion prevents air from entering or leaving the affected segment/lobe
- Gas already trapped distal to the foreign body is gradually absorbed by the capillaries
- Result: collapse (atelectasis) of the distal lung
- This is more common with impaction of large foreign bodies or with delayed presentation where swelling/granulation tissue converts a partial obstruction to complete obstruction
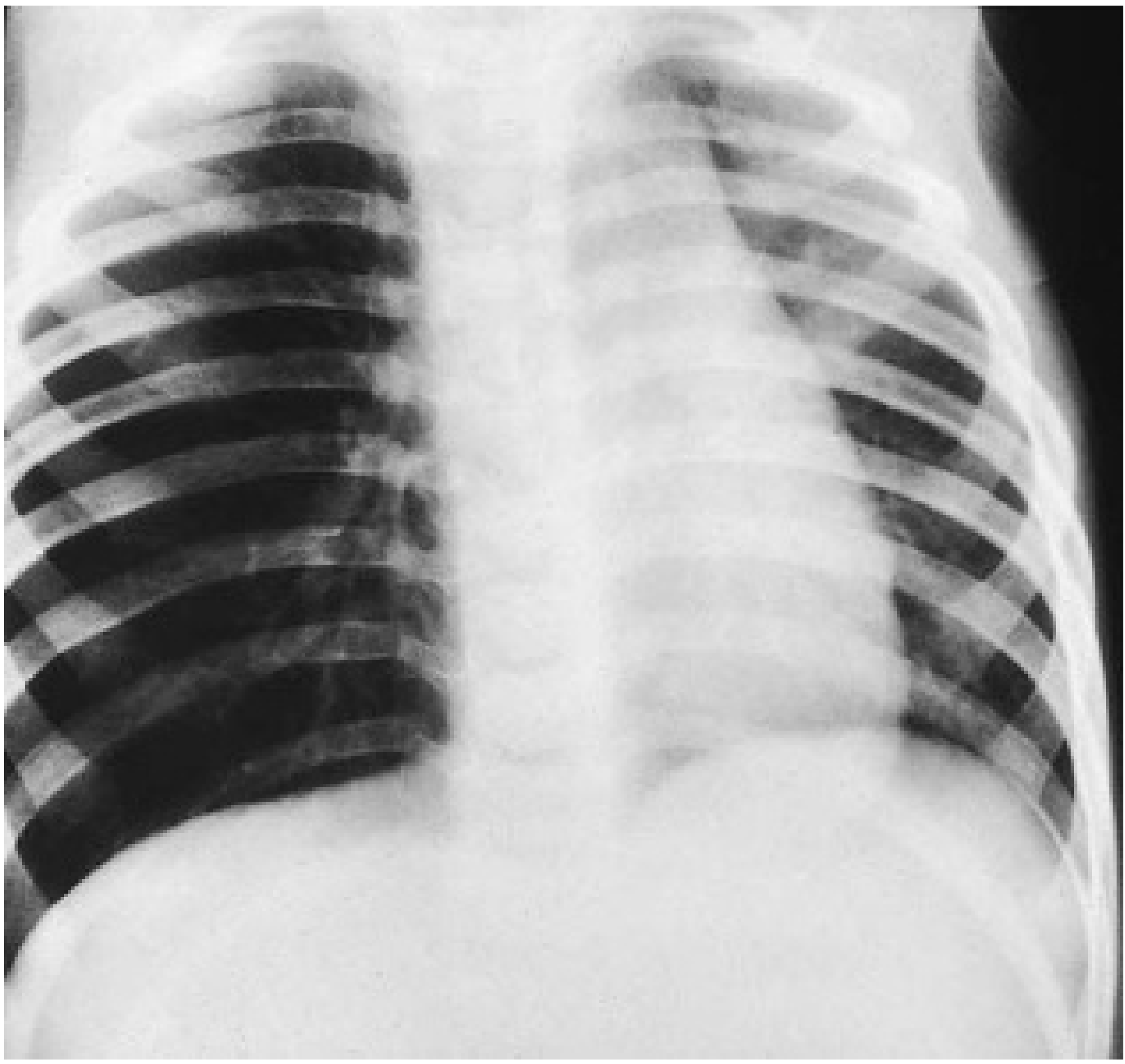
3. Radiological Correlates of the Pathophysiology
Chest X-ray (sensitivity ~73%, specificity ~45% - so a normal film does not exclude foreign body):
| Finding | Underlying Mechanism |
|---|---|
| Hyperinflation of ipsilateral lung | Ball-valve air trapping (check-valve effect) |
| Mediastinal shift away from the foreign body | Ipsilateral hyperinflation pushes mediastinum contralaterally |
| Elevated contralateral hemidiaphragm | Mediastinal shift secondary to ball-valve effect |
| Atelectasis / consolidation | Complete obstruction with distal gas absorption |
| Radiopaque object seen | Less than 25% of foreign bodies are radiopaque |
| Normal film | Seen in 11-26% of cases |
Inspiratory-expiratory films / decubitus views:
- On inspiration: the affected (hyperinflated) side appears relatively lucent/unchanged
- On expiration: the normal contralateral lung deflates and appears more opaque, while the obstructed side remains hyperinflated - this asymmetry confirms air trapping
4. Local Tissue Response (Inflammatory Pathophysiology)
Once lodged, the foreign body triggers a local inflammatory cascade:
- Mucosal irritation - immediate: cough reflex, mucosal edema, bronchospasm
- Neutrophilic infiltration - over hours to days: acute inflammation, increased secretions
- Granulation tissue formation - over days to weeks, especially with organic foreign bodies (peanuts, beans). Peanut oil is particularly inflammatory and accelerates granuloma formation
- Mucosal ulceration - due to direct pressure necrosis, particularly at the point of contact
- Post-obstructive infection - static secretions distal to the obstruction become colonized, leading to recurrent/chronic pneumonia, lung abscess, or ultimately bronchiectasis
Vegetable matter (especially dried beans) is particularly problematic - it absorbs moisture and swells after aspiration, converting a partial obstruction to complete obstruction and intensifying the inflammatory response.
5. Complications: Time-Dependent Pathophysiology
The duration of foreign body retention directly determines the severity of downstream pathology:
| Duration | Pathological Process |
|---|---|
| Acute (< hours) | Mucosal edema, bronchospasm, reflex cough |
| < 1 month | Partial/complete obstruction, air trapping or atelectasis; most patients recover completely after removal |
| 1-3 months | Granulation tissue, recurrent pneumonitis, partial recovery |
| > 3 months | Bronchiectasis, chronic inflammation, lung fibrosis; only ~30% recover completely |
- Scott-Brown's Otorhinolaryngology, p. 431: "When present for less than 1 month, all patients recovered completely but, if present for more than 3 months, only 30% recovered."
6. Symptom-Pathophysiology Correlation
| Symptom/Sign | Mechanism |
|---|---|
| Initial choking, gagging | Stimulation of laryngeal/tracheal receptors |
| Symptoms resolve briefly after initial episode | Foreign body passes beyond the vocal cords to the bronchus, where reflex sensitivity is lower |
| Unilateral wheeze | Turbulent airflow past partial obstruction |
| Decreased breath sounds ipsilaterally | Reduced airflow distal to the obstruction |
| Cyanosis | Ventilation-perfusion mismatch - perfusion continues to a non-ventilated lobe |
| Recurrent pneumonia (same lobe) | Post-obstructive infection from stagnant secretions |
| Chronic cough, bronchiectasis | Long-standing bronchial inflammation and structural remodeling |
- K.J. Lee's Essential Otolaryngology; Scott-Brown's, p. 431
Summary
The core pathophysiology of bronchial foreign body centers on the check-valve (ball-valve) mechanism: inspiratory dilation allows air past the object, but expiratory compression traps it, producing ipsilateral obstructive emphysema and mediastinal shift. Alternatively, complete obstruction leads to atelectasis. Superimposed on this mechanical obstruction is a time-dependent inflammatory response - from acute mucosal edema, through granulation tissue formation, to chronic bronchiectasis - driven by the nature of the object (organic matter is most inflammatory) and duration of impaction.
This is a shared conversation. Sign in to Orris to start your own chat.