Acute onset painless vision loss detailed information
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"acute vision loss" AND diagnosis
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the detailed, well-organized response.
Acute Onset Painless Vision Loss - Comprehensive Overview
Acute painless vision loss is one of ophthalmology's true emergencies. The key initial question is monocular vs. binocular - monocular loss is almost always a problem in that eye itself (retina, optic nerve, ocular vasculature), while binocular loss points to a retrochiasmal or intracranial process.
Classification by Anatomy
| Laterality | Location | Key Conditions |
|---|---|---|
| Monocular | Retinal vascular | CRAO, BRAO, CRVO |
| Monocular | Vitreous/retina | Vitreous hemorrhage, retinal detachment |
| Monocular | Optic nerve | AION (arteritic/non-arteritic) |
| Monocular | Transient | Amaurosis fugax |
| Binocular | Occipital cortex | Posterior circulation stroke |
1. Central Retinal Artery Occlusion (CRAO)
The most urgent ocular emergency.
Pathophysiology
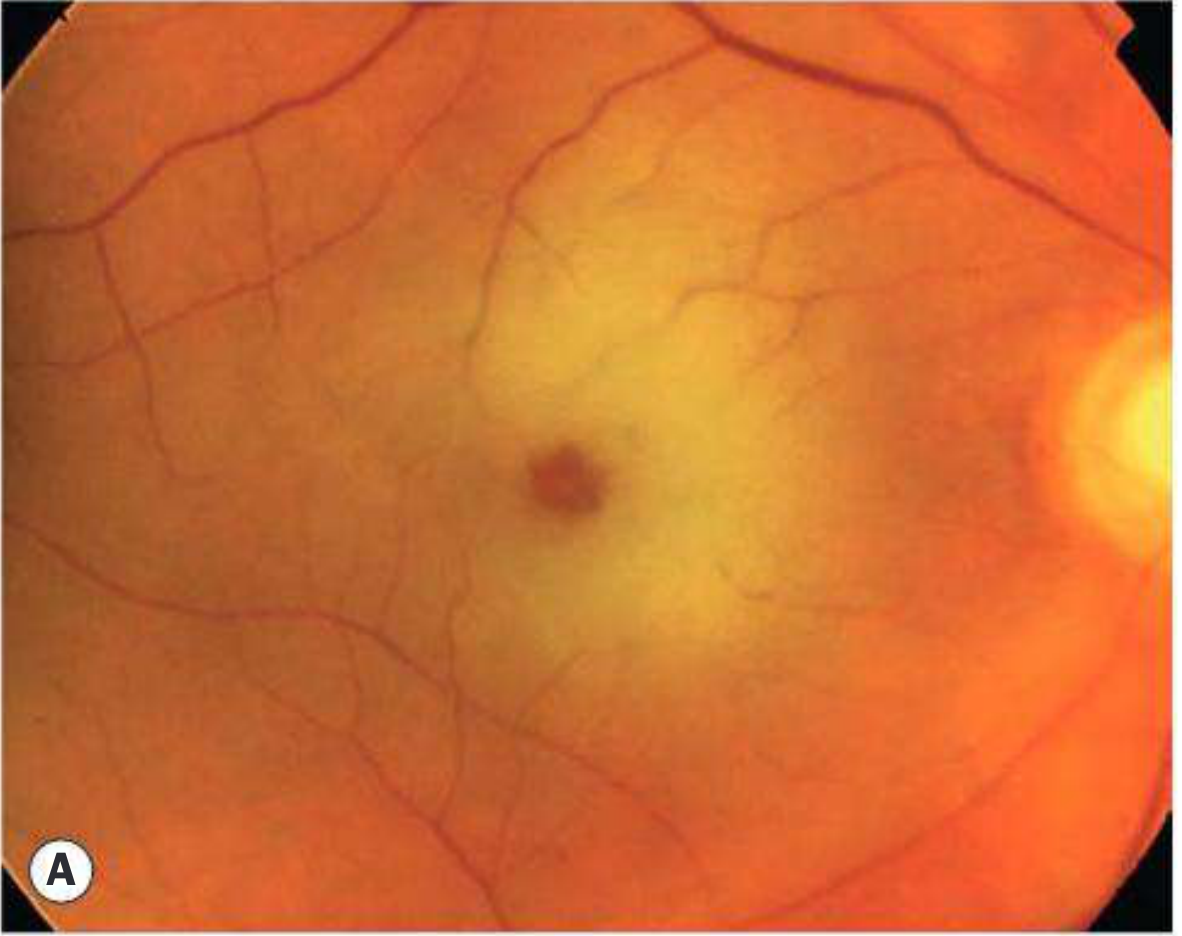
The central retinal artery - the first branch off the ophthalmic artery - supplies the inner retina. Occlusion causes ischemic infarction of the inner retina. The macula (thinnest part of the retina) allows the intact underlying choroidal circulation to remain visible, creating the classic "cherry-red spot" - the fovea retains its normal orange-red color while the surrounding pale ischemic retina creates the contrast.
Causes
- Carotid or cardiac embolism (most common)
- Retinal artery thrombosis
- Giant cell arteritis (GCA) - particularly in elderly; absence of light perception strongly suggests GCA or ophthalmic artery occlusion
- Vasculitis (SLE, polyarteritis nodosa)
- Sickle cell disease
- Hypercoagulable states
- Vasospasm (migraine)
- Elevated IOP (glaucoma)
Clinical Features
- Sudden (seconds), profound, painless, monocular vision loss - except in GCA where there may be pain
- Often preceded by episodes of amaurosis fugax
- Afferent pupillary defect (RAPD) - often total (amaurotic pupil)
- VA severely reduced; final VA worse than 6/120 in two-thirds of cases
Fundoscopic Findings
- Cherry-red spot at the macula (pathognomonic)
- Pale, opaque retina in all quadrants
- Arterial attenuation and "cattle-trucking" (segmented blood column)
- Peripapillary retinal swelling
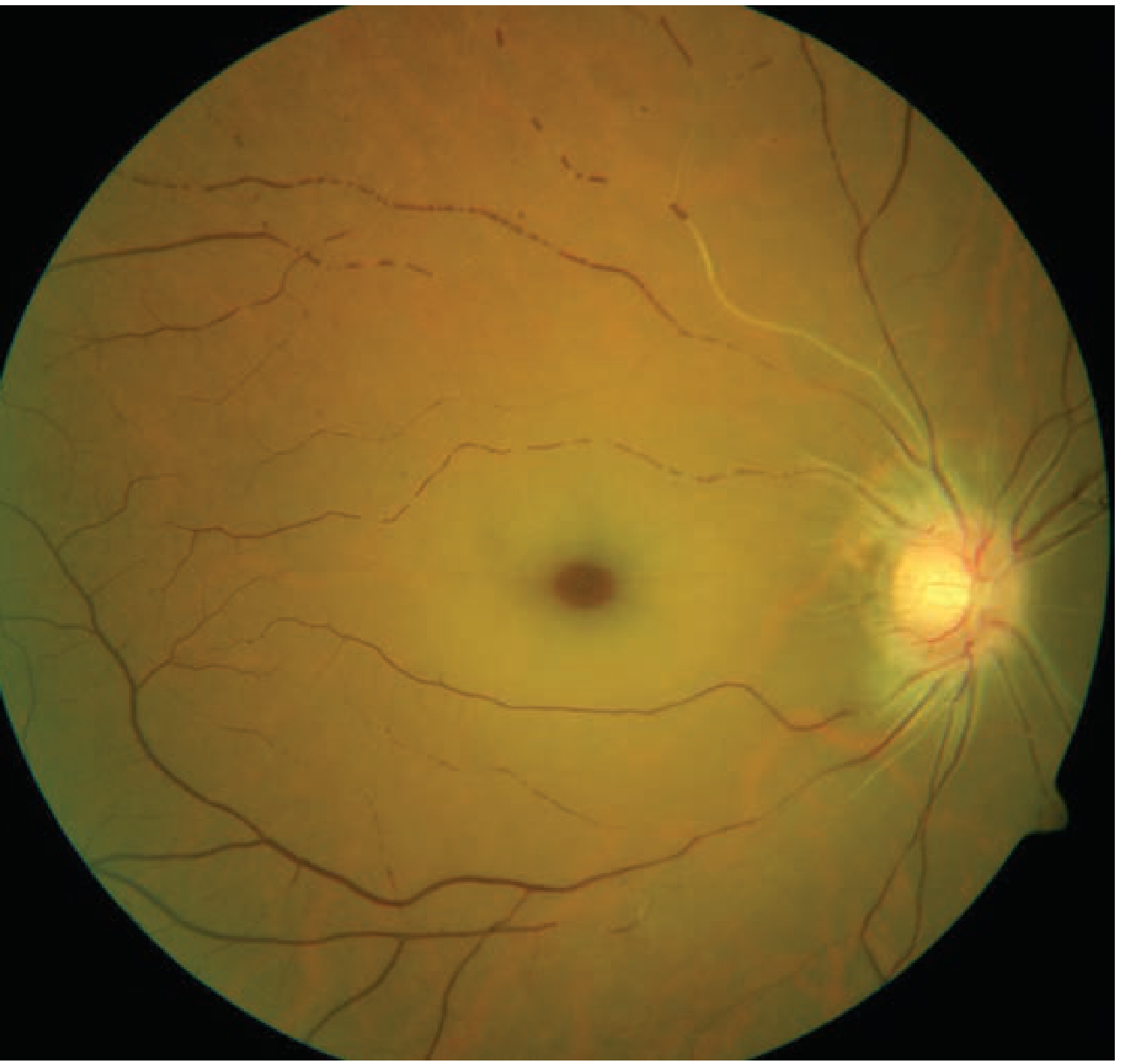
CRAO with cherry-red spot (Kanski's Clinical Ophthalmology):
CRAO from Tintinalli's Emergency Medicine (note retinal pallor and visible plaques in vessels):
Cilioretinal Artery Variant
In ~20-25% of eyes, a cilioretinal artery (arising from the posterior ciliary circulation) supplies a sector of the macula. When present, it can preserve central vision even in complete CRAO.
Treatment (Time-Critical)
Irreversible retinal damage occurs within 4-6 hours. All treatments have limited evidence:
- Ocular massage - 10-15 seconds of pressure followed by release for 3-5 minutes; aims to dislodge emboli mechanically
- Anterior chamber paracentesis - withdraws aqueous to lower IOP acutely
- IOP-lowering agents - topical timolol, systemic acetazolamide
- Breathing into a paper bag - raises pCO2, inducing vasodilation (limited evidence)
- IV tPA (alteplase 0.9 mg/kg) - considered within 4.5 hours; large trial of local intra-arterial rtPA showed no benefit; IV route remains investigational but increasingly used per stroke protocols
Key: Consult ophthalmology AND neurology immediately. Treat as a "stroke of the eye."
Systemic Workup (Mandatory)
- 30% of CRAO patients have severe carotid disease, coincidental stroke, or extreme hypertension
- 20% have simultaneous MI or critical heart disease
- 95% will need a change in systemic medication; 25% require urgent surgical intervention
- Urgent referral to stroke clinic; antiplatelet therapy (aspirin 600 mg loading), carotid Doppler, echocardiogram, ESR/CRP (for GCA)
2. Branch Retinal Artery Occlusion (BRAO)
- Symptoms: Sudden, profound, painless altitudinal or sectoral visual field loss; may go unnoticed if central vision is spared
- RAPD often present
- Fundus: Cloudy, white, edematous ("ground-glass") retina in the affected sector; one or more emboli often visible at arterial bifurcation points; "cattle-trucking" limited to affected vessel
- FA: Delayed arterial filling and hypofluorescence in the involved segment
- Management: Same approach as CRAO; systemic workup for embolic source is mandatory
- Prognosis: Visual field defect rarely recovers completely
3. Central Retinal Vein Occlusion (CRVO)
Pathophysiology
Venous thrombosis at the level of the lamina cribrosa causes venous stasis, retinal edema, and hemorrhage throughout all quadrants.
Risk Factors
Diabetes, hypertension, cardiovascular disease, dyslipidemia, hypercoagulable states, vasculitis, glaucoma (most important ocular risk factor), thyroid disease (compressing the vein), orbital tumors.
Types
Non-ischaemic CRVO ("venous stasis retinopathy"):
- More common; about one-third progress to ischaemic CRVO within months
- Sudden painless monocular fall in vision (variable severity)
- RAPD absent or mild
- Diffuse dot, blot, and flame hemorrhages (mild-moderate); disc edema; macular edema
- VA of 6/60 or better suggests non-ischaemic
Ischaemic CRVO:
- More severe vision loss; dense central scotoma with sparing of peripheral vision
- Significant RAPD
- More extensive retinal hemorrhages, more cotton-wool spots
- High risk of rubeosis iridis (neovascularization) and neovascular glaucoma within 3 months
Classic Fundoscopic Appearance
"Blood and thunder fundus" - optic disc edema + dilated, tortuous retinal veins + diffuse retinal hemorrhages in all four quadrants. The contralateral eye is normal (distinguishing it from papilledema).

Treatment
- Anti-VEGF injections (ranibizumab, bevacizumab) - first-line for macular edema
- Laser-induced chorioretinal anastomosis
- No universally beneficial single treatment; consult ophthalmology + neurology
- Pan-retinal photocoagulation for ischaemic CRVO to prevent neovascular glaucoma
4. Amaurosis Fugax (Transient Monocular Vision Loss)
- Transient painless monocular visual loss, classically described as "a curtain coming down over the eye"
- Usually lasts a few minutes, then fully recovers (in the reverse order of loss, but more gradually)
- Frequency: several times daily to once every few months
- Causes: embolic (most common), hemodynamic (carotid stenosis, hypotension), ocular (raised IOP, vasospasm), neurologic, idiopathic
- Can be accompanied by ipsilateral cerebral TIA (contralateral neurological features)
Important: Patients often cannot tell whether loss is monocular or involves the ipsilateral hemifield of both eyes (the latter indicates cerebral ischemia, not retinal).
Management is identical to CRAO - urgent stroke workup - because the 90-day stroke risk after amaurosis fugax is 10-15%.
5. Anterior Ischemic Optic Neuropathy (AION)
Pathophysiology
Loss of blood supply to the optic nerve head from the posterior ciliary arteries and peripapillary choroidal circulation. Comes in two forms:
Non-arteritic AION (NAION) - more common
- Onset typically abrupt and painless (occasionally progressive over days)
- Age >50, usually on a background of hypertensive vascular disease and diabetes
- No premonitory TIA-like episodes (unlike CRAO)
- Crowded "disc at risk" with a small cup-to-disc ratio is a key anatomic predisposing factor
- Episodes of nocturnal hypotension thought to precipitate ischemia
- Field defect: characteristically altitudinal (inferior > superior)
- Fundus: Sectoral or diffuse optic disc swelling with small flame-shaped hemorrhages; retina and retinal vessels are normal (unlike CRAO)
- Prognosis: Generally poor - optic atrophy develops as disc edema subsides; lifetime risk of fellow eye involvement ~25%
- Association: Sildenafil (PDE5 inhibitors) can precipitate NAION in patients with vascular risk factors; sleep apnea is an important risk factor
Arteritic AION (GCA-AION) - more severe
- Caused by giant cell arteritis (temporal arteritis)
- Typically age >60; women > men
- May be preceded by headache, jaw claudication, temporal artery tenderness, polymyalgia rheumatica symptoms, fever, anorexia
- Vision loss is more severe and bilateral involvement within days is a major risk if untreated
- ESR markedly elevated (typically 70-110 mm/h); CRP also elevated
- CT angiography (71% sensitive, 85.7% specific); MRI (94% sensitive, 78% specific)
- Treatment: HIGH-DOSE CORTICOSTEROIDS IMMEDIATELY - do not wait for temporal artery biopsy
- If no visual symptoms: prednisone 60 mg/day orally
- If visual loss present: IV methylprednisolone 500-1000 mg/day for 3 days
- Biopsy should be performed within 1 week of starting steroids (granulomatous changes persist for 2-4 weeks)
- Tocilizumab for steroid-resistant or intolerant cases
6. Retinal Detachment
- Symptoms: Flashes of light (photopsia), floaters, a dark veil or curtain in the visual field, decreased peripheral and/or central acuity
- Mechanism: Vitreous gel contraction with age causes posterior vitreous detachment (PVD); if it tears a retinal hole, fluid enters the subretinal space and peels the retina away
- Monocular; average age of onset 55 (but can occur in the 20s in highly myopic individuals)
- Examination: Requires dilated indirect ophthalmoscopic examination; ultrasound if media opacity
- Treatment: Ophthalmic emergency - surgical repair (pneumatic retinopexy, scleral buckle, or vitrectomy) required urgently before macular involvement
7. Vitreous Hemorrhage
- Symptoms: Sudden onset of floaters, haze, "cobwebs," or complete vision loss; painless
- Causes: Proliferative diabetic retinopathy (most common cause), posterior vitreous detachment with retinal tear, trauma, subarachnoid hemorrhage (Terson syndrome), retinal vein occlusion, sickle cell retinopathy
- Examination: Red reflex lost; fundus view obscured; ocular ultrasound can identify associated retinal detachment
- Management: If the retina cannot be visualized, urgent B-scan ultrasound. If retinal detachment present, urgent vitreoretinal surgery
8. Posterior Cortical (Binocular) Causes
Occipital lobe stroke (PCA territory):
- Sudden binocular vision loss, often hemianopic
- Contralateral homonymous hemianopia or cortical blindness
- Fundus is normal (key distinguishing feature)
- May be accompanied by other posterior circulation symptoms (vertigo, ataxia, diplopia)
Idiopathic Central Serous Retinopathy:
- Positive central scotoma of sudden onset, often with metamorphopsia (distorted straight lines) or micropsia
- Fluid leakage into the subretinal space
- Typically young adult men with type-A personality
- Diagnosis confirmed by FA or OCT
- Usually resolves spontaneously in weeks to months
Diagnostic Approach Summary
Step 1: Monocular or Binocular?
Monocular → retinal vascular, optic nerve, or vitreoretinal cause
Binocular → intracranial / retrochiasmal; check for other neurological signs
Step 2: Key Examination Findings
| Finding | Suggests |
|---|---|
| RAPD (afferent pupillary defect) | Optic nerve or severe retinal ischemia |
| Cherry-red spot | CRAO |
| "Blood and thunder" fundus | CRVO |
| Disc edema + altitudinal field defect | AION |
| Pale disc, no RAPD | Old optic atrophy |
| Dark veil/curtain + floaters/flashes | Retinal detachment |
| Normal fundus + monocular | Optic neuritis (painful), NAION, amaurosis |
| Normal fundus + binocular | Occipital cortex stroke |
Step 3: Urgency Stratification
| Condition | Urgency | Action |
|---|---|---|
| CRAO | Minutes | Immediate ophtho + neurology, tPA consideration |
| Arteritic AION (GCA) | Hours | IV steroids NOW, do not delay for biopsy |
| CRVO (ischaemic) | Hours | Urgent ophthalmology |
| Retinal detachment | Same day | Urgent vitreoretinal surgeon |
| Amaurosis fugax | Same day | Stroke workup |
| NAION | Same day | Ophthalmology, rule out GCA |
| Vitreous hemorrhage | Same day | Ophthalmology, B-scan US |
Key Differentiating Features at a Glance
| Condition | Pain | Laterality | Onset | RAPD | Fundus |
|---|---|---|---|---|---|
| CRAO | No (yes in GCA) | Monocular | Seconds | Profound | Cherry-red spot, pale retina |
| BRAO | No | Monocular | Seconds | Often present | Sectoral white retina, embolus |
| CRVO | No | Monocular | Hours-days | Mild-absent | Blood-and-thunder |
| AION | No | Monocular | Abrupt | Yes | Disc edema ± flame hemorrhages |
| Amaurosis fugax | No | Monocular | Minutes, resolves | Absent (transient) | Normal or embolus |
| Retinal detachment | No | Monocular | Minutes-hours | Absent | Detached retina |
| Vitreous hemorrhage | No | Monocular | Seconds | Absent | Absent red reflex |
| Occipital stroke | No | Binocular | Seconds | Absent | Normal |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., Chapters 13 (Retinal Vascular Disease) and Treatment sections
- Tintinalli's Emergency Medicine: A Comprehensive Study, Chapter 241 (Ocular Emergencies)
- Adams and Victor's Principles of Neurology, 12th Ed., Chapter 12
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 16
This is a shared conversation. Sign in to Orris to start your own chat.