Lacunar infract
Reading File
Finding Sources
Searching PubMed
"lacunar infarct"[MeSH Terms] AND stroke
Finding Sources
Searching PubMed
"lacunar stroke" AND pathophysiology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full, detailed answer.
Lacunar Infarct
Definition
A lacunar infarct (lacune) is a small ischemic infarction in the deep regions of the brain or brainstem, less than 15 mm in diameter, resulting from occlusion of a single penetrating artery. The term "lacuna" (Latin: small pit/lake) is a pathologic term referring to the small necrotic or cystic lesion left behind after infarction. A "lacunar syndrome" is the clinical picture resulting from such a lesion, though it can occasionally result from non-lacunar mechanisms (e.g., small subcortical hemorrhage).
Lacunar infarcts account for 15-26% of all ischemic strokes.
- Localization in Clinical Neurology, 8e, p. 1380
- Symptom to Diagnosis: An Evidence Based Guide, 4th Ed.
Pathophysiology
There are three main mechanisms:
1. Lipohyalinosis (most characteristic)
Long-standing arterial hypertension induces segmental arteriolar disorganization, hypertrophy of the media, and fibrinoid deposition on the vessel wall. This "lipohyalinosis" was originally described by CM Fisher on postmortem examination - he found eosinophilic degeneration of the wall of small penetrating arteries in the region of the infarct. This eventually leads to narrowing or occlusion of the vessel.
2. Microatheroma
Atherosclerosis at the origin of penetrating arteries from a parent major cerebral artery (e.g., MCA, PCA, basilar artery).
3. Microembolism
Less common - from arterial or cardiac sources, or arteriolar/capillary endothelial dysfunction.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, p. 278
- Adams and Victor's Principles of Neurology, 12th Ed.
- Localization in Clinical Neurology, 8e, p. 1380
Risk Factors
- Arterial hypertension (primary risk factor - ~80-90% of patients with lacunar stroke have hypertension)
- Diabetes mellitus
- Smoking
- Dyslipidemia
- African-American race (incidence approximately twice that in white population)
- Rarely: CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) - the most common monogenic cause of small vessel disease
Sites of Predilection
In order of frequency:
- Putamen (most common)
- Basis pontis
- Thalamus
- Posterior limb of the internal capsule
- Caudate nucleus
Less commonly: anterior limb of internal capsule, subcortical cerebral white matter, cerebellar white matter, corona radiata, corpus callosum.
- Localization in Clinical Neurology, 8e, p. 1380
- Rosen's Emergency Medicine, 9th Ed.
Classic Lacunar Syndromes (Five Classical)
At least 20 lacunar syndromes have been described; the five classical ones are:
1. Pure Motor Hemiplegia (PMH) - Most Common
- Frequency: 50-67% of lacunar strokes
- Location: Posterior limb of internal capsule, corona radiata, or basis pontis
- Features: Hemiparesis/hemiplegia of face, arm, AND leg. Mild dysarthria may be present at onset
- Absent features: No aphasia, apraxia, agnosia, sensory loss, visual, or higher cortical disturbances
- Capsular warning syndrome (crescendo TIAs) may precede it
2. Pure Sensory Stroke (PSS)
- Location: Ventroposterolateral nucleus of the thalamus (most common); also internal capsule/corona radiata, subthalamus, midbrain, parietal cortex
- Features: Numbness, paresthesias, and hemisensory deficit involving face, arm, trunk, and leg. Often cheiro-oral, cheiro-pedal, or cheiro-oral-pedal pattern
- In thalamic PSS: both spinothalamic AND medial lemniscal modalities affected
- In pontine PSS: vibration/position sense impaired, but pinprick/temperature preserved (selective medial lemniscal involvement)
3. Ataxic Hemiparesis (AH) - Second Most Common
- Location: Posterior limb of internal capsule, basis pontis, corona radiata
- Features: Combination of ipsilateral cerebellar ataxia AND contralateral hemiparesis (leg > arm), often with dysarthria ("dysarthria-clumsy hand syndrome" is a variant)
4. Sensorimotor Stroke
- Location: Posterolateral thalamus and adjacent internal capsule
- Features: Both hemiparesis and hemisensory loss
5. Dysarthria-Clumsy Hand Syndrome
-
Location: Basis pontis or genu of internal capsule
-
Features: Dysarthria + ipsilateral hand clumsiness/weakness, facial weakness, dysphagia
-
Localization in Clinical Neurology, 8e, pp. 1380-1382
Key Clinical Features
- Onset: Typically abrupt or stuttering (can evolve over hours)
- Cortical signs are ABSENT: No aphasia, agnosia, apraxia, hemianopsia, or neglect
- Consciousness preserved (unless bilateral or strategically located)
- Size: Infarcts range from a few millimeters to 2 cm
- Preceding TIAs are common, especially the capsular warning syndrome
Neuroimaging
CT:
- Acute: small hypodensity in deep brain structures
- Chronic: hypodense cystic lesion
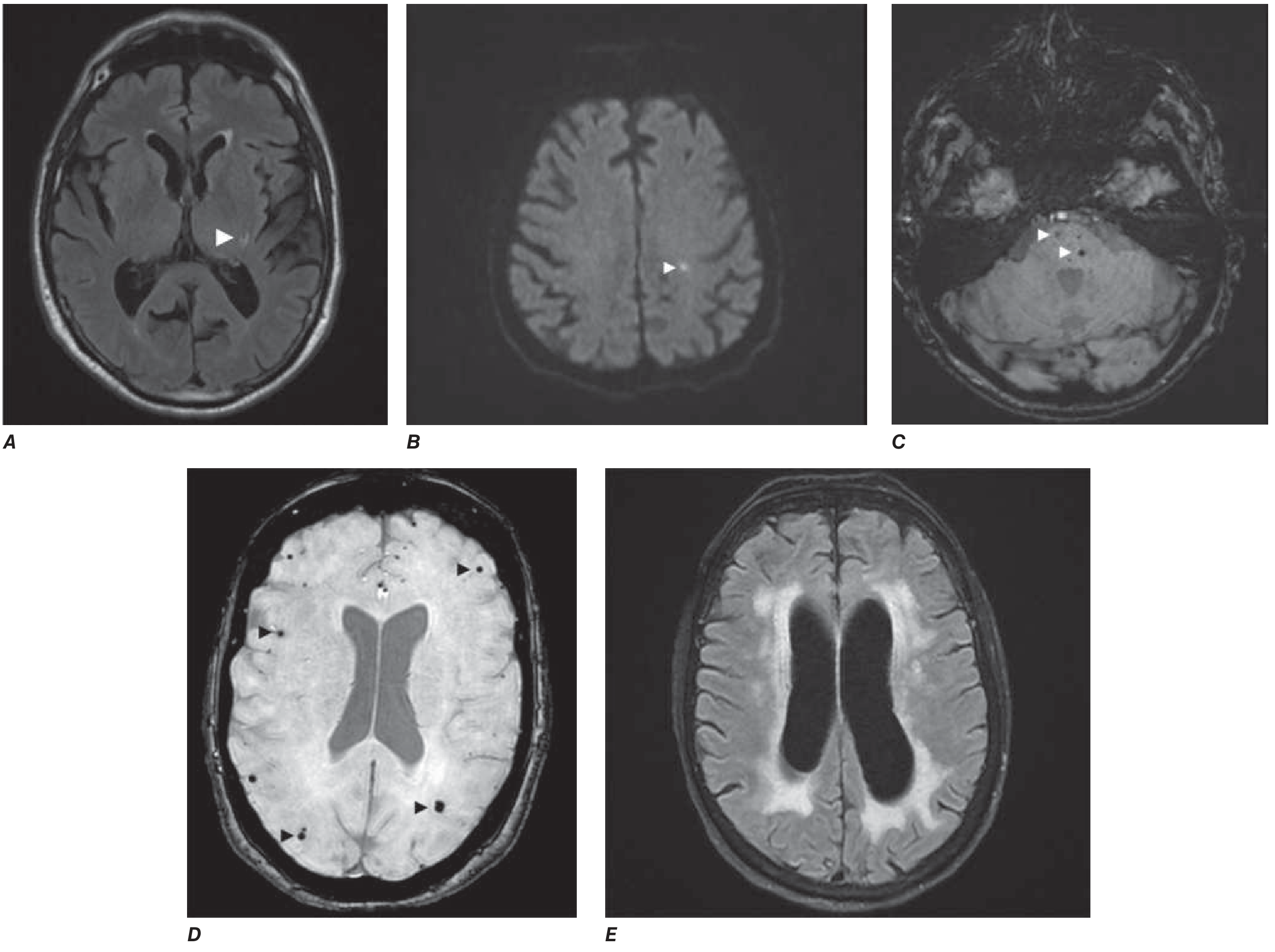
MRI (gold standard):
- Acute: DWI (diffusion-weighted imaging) shows restricted diffusion (bright signal)
- Chronic (FLAIR): Hyperintense rim surrounding a hypointense cavitated core, typically 3-15 mm diameter (Fig. 444-1A from Harrison's)
- Associated findings: white matter hyperintensities (periventricular leukoaraiosis), cerebral microbleeds on T2*/SWI sequences
The FLAIR appearance evolves in only a subset of small infarctions - many cannot be identified in the chronic stage.
- Harrison's Principles of Internal Medicine, 22E, p. 3533
- Neuroanatomy through Clinical Cases, 3rd Ed.
Diagnosis
- Diagnosis requires correlation of clinical lacunar syndrome + imaging
- The mere association of a lacunar syndrome with hypertension and DM is insufficient - other stroke causes (especially cardioembolic) must be excluded
- Embolic workup (echocardiography, cardiac monitoring for AF) should be performed even when lacunar mechanism is suspected
- TOAST classification categorizes this as "small vessel occlusion"
Management
Acute:
- IV tPA (alteplase) if within 4.5 hours of onset and eligible (same criteria as other ischemic strokes)
- Aspirin is favored over warfarin for secondary prevention in cryptogenic/lacunar stroke (clinical trial evidence supports no difference between aspirin and warfarin)
Secondary Prevention:
-
Aggressive hypertension control (primary target - SPRINT-MIND trial supports SBP <120 mmHg)
-
Antiplatelet therapy (aspirin, clopidogrel, or aspirin + dipyridamole)
-
Statin therapy (for associated dyslipidemia/atherosclerosis)
-
Diabetes control
-
Smoking cessation
-
Neuroanatomy through Clinical Cases, 3rd Ed., p. 302
-
Harrison's Principles of Internal Medicine, 22E, p. 3533
Prognosis and Complications
- Good short-term prognosis for individual lacunar strokes - deficits often improve significantly (as in the case from Neuroanatomy through Clinical Cases: numbness completely resolved in 5 days)
- Risk of recurrence (stroke recurrence rate ~1% per year for pure lacunar disease)
- Multiple lacunar infarcts over time can lead to vascular dementia - a multi-infarct dementia syndrome with dementia, gait abnormalities, and pseudobulbar signs (Binswanger disease in severe white-matter predominant form)
- Associated microbleeds and white matter hyperintensities indicate ongoing small vessel disease
Summary Table
| Feature | Lacunar Infarct |
|---|---|
| Size | < 15 mm |
| Mechanism | Lipohyalinosis, microatheroma, embolism |
| Key risk factor | Hypertension |
| Common sites | Putamen, pons, thalamus, internal capsule |
| Cortical signs | Absent |
| Classic syndromes | PMH, PSS, AH, sensorimotor, dysarthria-clumsy hand |
| MRI (chronic) | FLAIR: hyperintense rim + hypointense core |
| Secondary prevention | BP control + antiplatelet |
Tq
You're welcome! Feel free to ask anytime you need help with lacunar infarcts or any other topic. 😊
Ok
Whenever you're ready with your next question, I'm here! 👍
This is a shared conversation. Sign in to Orris to start your own chat.