12 year old boy with CSOM planned for tympanomastoidectomy(middle ear surgery ) -write me a long case presentation for MD anaesthesia final practical exam - include structured case presentation - pre op ,intra op, post op anesthesia management - include viva questions - act like a professor in anesthesia & teach me how to present case, and answer questions at every point needed in the above long case presentation
LONG CASE PRESENTATION
MD Anaesthesia Final Practical Examination
Case: 12-Year-Old Boy with CSOM Planned for Tympanomastoidectomy
Professor's Opening Note to the Candidate: "When you walk into your final practical, remember - the examiner is not testing whether you memorize drug doses. They want to see a thinking anaesthesiologist. Present systematically. Every clinical finding you mention must lead to an anaesthetic implication. If you say 'the child has CSOM,' the very next thought must be: 'and this affects my anaesthetic plan in the following three ways...' That is how you pass. That is how you practice."
PART 1: STRUCTURED CASE PRESENTATION
HOW TO OPEN YOUR PRESENTATION
"Good morning sir/madam. I would like to present a long case of a 12-year-old male child, Master [Name], weighing approximately 32 kg, admitted for elective tympanomastoidectomy under general anaesthesia for chronic suppurative otitis media of the right/left ear."
SECTION 1: HISTORY
Chief Complaint
- Persistent ear discharge from the right/left ear for [X] years
- Decreased hearing in the affected ear
- Occasional earache and headache
History of Present Illness
- CSOM diagnosed [X] years ago
- Character of discharge: mucopurulent, non-bloody, intermittent/persistent, offensive or non-offensive odour
- Associated symptoms: conductive hearing loss (gradual), tinnitus, occasional vertigo
- No facial palsy (important - rules out cholesteatoma eroding facial canal)
- No headache, neck stiffness, or altered sensorium (rules out intracranial extension - meningitis, brain abscess)
- Conservative treatment tried: topical ear drops, systemic antibiotics - failed to control infection
- Surgery advised: tympanomastoidectomy (combined approach tympanoplasty with cortical mastoidectomy)
Past Medical History
- No known systemic illness (diabetes, asthma, epilepsy, cardiac disease)
- No previous surgeries or anaesthesia (important - no h/o adverse events, malignant hyperthermia, difficult airway)
- No h/o bleeding tendency or clotting disorders
Drug History
- Current medications: topical ciprofloxacin/gentamicin ear drops
- Any systemic antibiotics in recent weeks
- No known drug allergies (NKDA) - always state this explicitly
Family History
- No family h/o anaesthesia-related complications (malignant hyperthermia is autosomal dominant - always ask)
- No family h/o bleeding disorders
Nutritional & Developmental History
- Normal growth and development for age
- Regular school attendance, no cognitive impairment
"Why is family history of anaesthesia complications relevant here?"
SECTION 2: REVIEW OF SYSTEMS (RELEVANT)
| System | Findings | Anaesthetic Relevance |
|---|---|---|
| ENT | CSOM with perforation | Eustachian tube dysfunction - N₂O contraindicated |
| Respiratory | No URTI, no asthma | Proceed with elective surgery |
| Cardiovascular | No murmur, no exertional dyspnoea | ASA I |
| Neurological | No headache, no cranial nerve deficits | No intracranial complication |
| GI | No reflux, last meal [X] hours ago | Fasting status confirmed |
| Haematological | No bruising, no prolonged bleeding | No coagulopathy |
SECTION 3: PHYSICAL EXAMINATION
- Well-nourished, well-developed 12-year-old male
- Weight: ~32 kg, Height: ~145 cm
- Afebrile (if febrile - surgery to be deferred; active infection increases anaesthetic risk)
- No pallor, icterus, cyanosis, clubbing, lymphadenopathy, or oedema (PICLE)
- Vitals: HR 88/min, RR 18/min, SpO₂ 99% RA, BP 100/65 mmHg
| Parameter | Finding | Significance |
|---|---|---|
| Mouth opening | >3 finger-breadths (inter-incisor distance >4 cm) | Adequate |
| Mallampati Class | Class I or II | Easy intubation predicted |
| Thyromental distance | >3 finger-breadths (>6.5 cm) | Adequate |
| Neck mobility | Full range of motion | No restriction |
| Jaw protrusion (ULBT) | Class A | Favourable |
| Teeth | All permanent teeth erupting; note any loose teeth | Document - may dislodge during laryngoscopy |
| Tonsils | Grade I/II | Note if enlarged - may affect view |
| Nasal cavity | Patent bilaterally | Relevant for nasal intubation if needed |
"What is the Mallampati classification? Which class does this child belong to?"
- Class I: Soft palate, fauces, uvula, tonsillar pillars visible
- Class II: Soft palate, fauces, uvula visible
- Class III: Soft palate, base of uvula visible
- Class IV: Only hard palate visible
- Cardiovascular: S1 S2 heard, no murmurs. HR regular.
- Respiratory: Air entry equal bilaterally, no adventitious sounds, no signs of URTI (critical - see below)
- Abdomen: Soft, non-tender
- ENT Examination: Perforated tympanic membrane (central/marginal), mucopurulent discharge, mastoid tenderness on palpation (if present = active mastoiditis)
- Neurological: Cranial nerves intact, no facial palsy, no signs of raised ICP
"This child has active ear discharge today. Would you proceed with anaesthesia?"
- If the child has FEVER (>38°C), active systemic infection, signs of intracranial complication (meningitis, brain abscess), or a coexisting URTI - surgery should be deferred.
- Active URTI is a significant concern because it increases perioperative respiratory adverse events (PRAE): laryngospasm, bronchospasm, oxygen desaturation. Miller's Anesthesia recommends postponing elective surgery for 4-6 weeks after resolution of URTI symptoms (though this is nuanced by symptom severity).
- Source: Miller's Anesthesia, 10e - URI increases risk of laryngospasm, bronchospasm, breath-holding, atelectasis, and unplanned hospital admission.
PART 2: PREOPERATIVE ANAESTHESIA MANAGEMENT
SECTION 4: PREOPERATIVE INVESTIGATIONS
| Investigation | Finding | Anaesthetic Relevance |
|---|---|---|
| Haemoglobin | >10 g/dL (target) | Blood loss in mastoidectomy can be moderate; anaemia increases risk |
| Haematocrit/PCV | Normal | - |
| Blood group & Cross-match | Done | Mastoidectomy near sigmoid sinus - risk of venous sinus injury |
| Bleeding time, Clotting time | Normal | No coagulopathy |
| PT/INR | Normal | - |
| RBS | Normal | Perioperative glucose monitoring in paediatrics |
| Serum electrolytes | Normal | - |
| Urine routine | Normal | - |
| ECG | Normal sinus rhythm | Not mandatory for ASA I <40 years, but done |
| Chest X-ray | Clear lung fields | Not mandatory, but done if clinically indicated |
| Pure tone audiometry | Conductive hearing loss | Surgical documentation |
| CT temporal bone | Extent of disease, ossicular erosion, facial canal involvement | Guides surgical and anaesthetic planning |
"Why did you request blood grouping and cross-matching for what seems like a routine ear surgery?"
SECTION 5: PREOPERATIVE OPTIMISATION
- Ear discharge: Topical antibiotic ear drops for at least 2-4 weeks pre-operatively to reduce bacterial load (decreases intraoperative contamination)
- Nutritional status: Optimise nutrition if malnourished (poor wound healing)
- Haemoglobin: If Hb <10 g/dL - correct anaemia before elective surgery with iron supplementation or blood transfusion
- Informed consent: From parent/guardian. Explain: general anaesthesia, risks (nausea, vomiting, sore throat, rare risks of aspiration, awareness under anaesthesia, anaphylaxis, difficult airway)
- Anxiolysis: Reassure child; child life specialist or play therapy pre-operatively
- Consent for TIVA: Preferred over volatile-based technique (see intraoperative section)
SECTION 6: PREOPERATIVE FASTING (NPO GUIDELINES)
| Substance | Minimum Fasting Duration |
|---|---|
| Clear liquids (water, juice without pulp, tea/coffee without milk) | 2 hours |
| Breast milk | 4 hours |
| Infant formula | 6 hours |
| Light meal (toast + clear liquid) | 6 hours |
| Heavy/fatty meal | 8 hours |
Professor's Note: Prolonged fasting in children causes hypoglycaemia and dehydration. Always check the last meal time, calculate deficit, and replace intraoperative fluid accordingly.
"The child is scheduled for 10 AM. When do you allow the last clear fluids?"
SECTION 7: PREMEDICATION
| Drug | Dose | Route | Timing | Purpose |
|---|---|---|---|---|
| Midazolam | 0.5 mg/kg oral (max 15 mg) | Oral | 30-45 min before induction | Anxiolysis, anterograde amnesia |
| Paracetamol | 15 mg/kg | Oral or rectal | 45-60 min before | Pre-emptive analgesia |
| Ondansetron | 0.1 mg/kg IV (max 4 mg) | IV | At induction | PONV prophylaxis |
| Dexamethasone | 0.1-0.15 mg/kg IV (max 8 mg) | IV | At induction | PONV prophylaxis + anti-inflammatory |
| Atropine | 0.02 mg/kg IV (min 0.1 mg, max 0.5 mg) | IV | Induction | Antisialagogue, prevent bradycardia |
"Why is PONV prophylaxis so important in this case?"
- Female sex would score 1 - here male, so 0
- Non-smoker - this 12-year-old is a non-smoker = 1 point
- History of PONV or motion sickness - if present = 1 point
- Postoperative opioid use - if planned = 1 point
- Middle ear/inner ear surgery - independent risk factor beyond the Apfel score
- Increase intracranial pressure
- Displace the tympanic membrane graft
- Cause aspiration
- Increase post-operative pain
PART 3: INTRAOPERATIVE ANAESTHESIA MANAGEMENT
SECTION 8: OPERATING ROOM SETUP
- Anaesthesia machine checked (O₂, circuit, CO₂ absorber)
- Suction working
- Difficult airway cart available (videolaryngoscope, supraglottic airways, bougie)
- Drugs drawn: propofol, fentanyl, atracurium, atropine, adrenaline, vasopressors
- Paediatric ETT sizes ready: 5.0, 5.5, 6.0 cuffed (for 12-year-old = age/4 + 4 = 7, but actual size based on weight/clinical assessment; cuffed tube preferred)
- Temperature monitoring (paediatrics are prone to hypothermia; maintain warm OR, use warm IV fluids, warming blanket)
- Nerve integrity monitor (NIM) if facial nerve monitoring planned by surgeon
"What size ETT will you use for this 12-year-old boy?"
- Formula: ETT internal diameter (mm) = (Age/4) + 4 = (12/4) + 4 = 7.0 mm for uncuffed tube
- For cuffed tube: subtract 0.5 = 6.5 mm cuffed
- In practice, always have one size above and one size below (6.0, 6.5, 7.0) ready
- For ear surgery, a south-facing (RAE oral preformed) tube or armoured (reinforced) tube is preferred because the surgical field is the head/neck and the surgeon needs unobstructed access
- Confirm position by auscultation bilaterally and end-tidal CO₂
SECTION 9: INDUCTION OF ANAESTHESIA
- Avoids nitrous oxide (mandatory in ear surgery)
- Propofol-based TIVA significantly reduces PONV compared to volatile agents
- Provides smoother emergence, less airway reactivity
- Allows rapid recovery
- Source: Scott-Brown's Otolaryngology - "TIVA is commonly used. Advantages include improved cardiovascular stability, decreased PONV and a short recovery time."
| Step | Drug | Dose (for 32 kg child) |
|---|---|---|
| Pre-oxygenation | 100% O₂ for 3-5 minutes | Via face mask |
| Analgesia | Fentanyl 2 mcg/kg IV | = 64 mcg (round to 60 mcg) |
| Induction | Propofol 2-2.5 mg/kg IV slowly | = 64-80 mg (give over 60-90 sec) |
| Muscle relaxant | Atracurium 0.5 mg/kg IV | = 16 mg |
| OR: if shorter relaxation needed | Rocuronium 0.6 mg/kg IV | = 19.2 mg |
| Antisialagogue | Glycopyrrolate 5 mcg/kg IV OR Atropine 0.02 mg/kg | To dry secretions |
| Anticholinergic | Atropine 0.02 mg/kg | = 0.64 mg (if not given above) |
- Direct laryngoscopy with Macintosh blade size 3
- Insert 6.5 cuffed oral RAE tube (or standard ETT)
- Confirm: bilateral breath sounds, EtCO₂ capnography waveform present
- Inflate cuff to minimum occlusive pressure
- Secure tube firmly with tape
- Eyes taped/padded (corneal abrasion risk with head-turning)
"Why is succinylcholine avoided in this case?"
- Risk of malignant hyperthermia - succinylcholine is a known trigger
- Muscle fasciculations - can increase intraocular pressure, intragastric pressure, and cause myalgias in older children
- Hyperkalaemia risk in burns, crush injuries, denervation (not applicable here, but principle)
- Rocuronium with sugammadex reversal is now the preferred alternative for rapid airway control
- For elective surgery with predicted easy airway, a non-depolarising agent (atracurium, rocuronium) with adequate time for onset is safer and preferred
SECTION 10: POSITIONING
- Head ring to stabilise head
- 15-degree reverse Trendelenburg (head-up tilt) to:
- Reduce venous congestion in the head and neck
- Decrease bleeding in the surgical field
- Source: Morgan and Mikhail (7e) - "Techniques to minimize blood loss during ear surgery include mild (15°) head elevation"
- Armboard tucked so surgeon can stand freely at the head
- Eyes padded bilaterally - extreme head-turning can cause direct pressure on the dependent eye and corneal abrasion from drapes
- ETT secured on the side AWAY from surgery - double check after final positioning
- Avoid neck flexion/extension - may kink ETT, especially if armoured tube not used
"What is the danger of extreme head-turning in this position?"
- Occlusion/kinking of the endotracheal tube - check EtCO₂ and airway pressures after final positioning
- Venous obstruction - rotation can compress jugular veins on the dependent side, increasing intracranial venous pressure and bleeding at the surgical field
- Brachial plexus stretch - if shoulder is not adequately padded
- Vertebral artery compression - in patients with cervical spondylosis (not relevant in this 12-year-old, but important in adults)
- Pressure on the dependent eye - corneal abrasion or even central retinal artery occlusion
SECTION 11: MAINTENANCE OF ANAESTHESIA
Option A: TIVA (Preferred)
| Drug | Infusion Rate |
|---|---|
| Propofol | 4-12 mg/kg/hr (target-controlled infusion TCI or manual infusion) |
| Remifentanil | 0.05-0.25 mcg/kg/min |
- No nitrous oxide
- Oxygen in air (FiO₂ 0.3-0.4)
- Maintain BIS (Bispectral Index) 40-60 for adequate depth of anaesthesia
- Short-acting opioids such as remifentanil allow greater control of cardiovascular stability and facilitate controlled/deliberate hypotension
Option B: Volatile-based (if TIVA not available)
- Sevoflurane in oxygen + air (NO N₂O)
- Minimum Alveolar Concentration (MAC) 1.0-1.5 MAC
- Maintain with fentanyl top-ups (1-2 mcg/kg PRN)
"Explain exactly why nitrous oxide is contraindicated in this case. What happens physiologically?"
- Displace the tympanic membrane graft - causing surgical failure
- Rupture the ossicular chain reconstruction
- Pre-graft placement: even with the ear open, N₂O expands the air, and when the surgeon closes the cavity, a pressure gradient develops
- If N₂O is stopped AFTER graft placement, the rapid washout of N₂O creates negative middle ear pressure which can also displace the graft
- Solution: Either avoid N₂O entirely throughout the case (preferred), OR discontinue N₂O at least 15-30 minutes before graft placement and ensure complete washout
- Additionally, patients with CSOM have obstructed Eustachian tubes - they cannot passively vent middle ear pressure fluctuations, making them particularly vulnerable
SECTION 12: CONTROLLED/DELIBERATE HYPOTENSION
| Agent | Mechanism | Notes |
|---|---|---|
| Remifentanil infusion | Opioid-mediated decrease in SVR and HR | Preferred - ultra-short acting, titratable |
| Propofol TIVA | Vasodilation, ↓ cardiac output | Synergistic with remifentanil |
| Esmolol infusion | Beta-1 blockade → ↓ HR, ↓ CO | Used to control reflex tachycardia |
| Labetalol (alpha+beta) | ↓ SVR + ↓ HR | Less titratable |
| Dexmedetomidine | Alpha-2 agonist, ↓ sympathetic tone | Has analgesic-sparing effect |
| Head-up tilt 15° | Reduces venous pooling in head | Simple, non-pharmacological |
| Infiltration by surgeon | Epinephrine 1:200,000 in local anaesthetic | Local vasoconstriction; watch for arrhythmias |
- Uncontrolled hypertension
- Cerebrovascular disease, carotid stenosis
- Severe anaemia (Hb <8 g/dL)
- Renal insufficiency
- Scott-Brown's notes: "Hypotension should be limited in patients with uncontrolled hypertension, cerebrovascular or ischaemic disease"
"The surgeon has injected epinephrine 1:50,000 around the ear. You notice sudden hypertension and bradycardia (or tachycardia + tachyarrhythmia). What do you do?"
- Epinephrine 1:50,000 is a higher concentration (compared to 1:200,000) and systemic absorption can cause:
- Tachycardia and hypertension (beta-1 and alpha-1 effects)
- Ventricular ectopics or VT (especially with volatile anaesthetics - halothane sensitises most, sevoflurane less so)
- Management:
- Alert surgeon to stop further injection
- Increase anaesthetic depth (propofol bolus/increase infusion)
- If arrhythmia: ensure adequate ventilation (hypocapnia or hypercapnia worsen arrhythmias), correct hypokalaemia
- For VT: lidocaine 1 mg/kg IV, esmolol 0.5 mg/kg IV
- For refractory hypertension: labetalol, esmolol
- Avoid treating bradycardia with atropine if BP is already high - this may worsen hypertension
- Document and communicate with surgical team
SECTION 13: FACIAL NERVE MONITORING
- The facial nerve runs through the mastoid and is at risk of injury during drilling
- Surgeons may request intraoperative facial nerve monitoring (NIM - nerve integrity monitoring)
- If NIM is planned: muscle relaxants must NOT be used in the post-intubation period
- Use a NIM endotracheal tube (electrodes contact the vocal cords to also detect recurrent laryngeal nerve injury in some cases)
- Anaesthesiologist must communicate with the surgeon before case begins about relaxant plan
- Source: Morgan and Mikhail (7e) and Miller's Anesthesia (10e) both emphasise this point
"The surgeon asks you to give a muscle relaxant mid-surgery because the patient moved. What is your response?"
- Immediately ask the surgeon - is facial nerve monitoring in use? If yes, NMBs are absolutely contraindicated intraoperatively as they will abolish the EMG signal and make nerve identification impossible.
- If NIM is NOT in use and patient moved due to inadequate depth - first increase anaesthetic depth (propofol bolus, increase infusion/volatile)
- If movement persists despite adequate depth - check TOF ratio. If there is residual block, additional relaxant can be given. If TOF ratio is 1.0 (fully recovered), movement suggests light anaesthesia.
- In TIVA, if the patient is waking up: remifentanil bolus + propofol bolus are first-line
- Never give a relaxant reflexively without understanding why the patient moved
SECTION 14: MONITORING
| Monitor | What it tells you |
|---|---|
| ECG (5-lead) | HR, rhythm, ST changes |
| Pulse oximetry (SpO₂) | Oxygenation |
| Non-invasive BP (NIBP) q3-5 min | Haemodynamic status |
| Capnography (EtCO₂) | Ventilation adequacy, ETT position, air embolism detection |
| Temperature | Hypothermia prevention in paediatrics |
| Neuromuscular monitoring (TOF) | NMB depth, reversal adequacy |
| BIS monitor | Depth of anaesthesia, prevent awareness |
| Urine output (if >3 hr surgery) | Hydration, renal perfusion (target 0.5-1 mL/kg/hr) |
| Intra-arterial line | If deliberate hypotension planned - real-time BP + ABG sampling |
SECTION 15: FLUID MANAGEMENT
- First 10 kg: 4 mL/kg/hr = 40 mL/hr
- Next 10 kg: 2 mL/kg/hr = 20 mL/hr
- Next 12 kg: 1 mL/kg/hr = 12 mL/hr
- Total maintenance = 72 mL/hr
- If NPO for 8 hours: deficit = 8 × 72 = 576 mL
- Replace: 50% in first hour, 25% in second, 25% in third
- Ear surgery blood loss is typically small (<100-150 mL)
- Calculate MABL = TBV × (Hct_start - Hct_min) / Hct_avg
- TBV in child = 70-80 mL/kg = 2240-2560 mL
- For Hb 12 g/dL (Hct 36%), target minimum Hct 25% (Hb 8 g/dL)
- Replace with crystalloid (3:1) up to MABL; packed red cells if MABL exceeded
SECTION 16: VENTILATION
- Mode: Volume control or pressure control ventilation
- Tidal volume: 6-8 mL/kg = 190-255 mL
- Rate: 14-18 breaths/min
- EtCO₂ target: 35-40 mmHg (normocapnia)
- Mild hypocapnia (EtCO₂ 32-35 mmHg): May be used to reduce cerebral blood volume and venous ooze
- Avoid hypercapnia - causes vasodilation, increases venous bleeding at surgical site
- PEEP: 3-5 cmH₂O to prevent atelectasis
PART 4: EMERGENCE AND EXTUBATION
SECTION 17: EMERGENCE FROM ANAESTHESIA
- Coughing, straining → raises venous pressure → bleeding → graft displacement
- PONV → graft displacement, aspiration
- Pain and agitation → uncontrolled head movement
- Preferred in ear surgery to avoid coughing on the tube
- Pre-requisites: full stomach NOT suspected, no difficult airway, haemodynamically stable, adequate reversal
- Turn patient to lateral position (or semi-lateral) before extubation
- Remove ETT while patient is still in deep plane of anaesthesia (before airway reflexes return)
- Transition to spontaneous ventilation on face mask
- Source: Morgan and Mikhail (7e) - "deep extubation is often utilised" in ear surgery
- Ensure full reversal: neostigmine 50 mcg/kg + glycopyrrolate 10 mcg/kg IV
- Wait for TOF ratio >0.9 (preferred >1.0 with quantitative monitoring)
- Wait for spontaneous breathing, eye opening, purposeful movements
- Give lidocaine 1 mg/kg IV 1-2 min before extubation to blunt cough reflex
- Alternatively: remifentanil infusion continued at low dose (0.01-0.05 mcg/kg/min) during emergence to suppress coughing without causing apnoea
"You have extubated the child (deep extubation). He suddenly develops stridor and SpO₂ begins to fall. What is your diagnosis and management?"
- Diagnosis: Inspiratory stridor, paradoxical chest movement, SpO₂ falling, no air entry on auscultation
- Immediate management (ladder approach):
- Call for help immediately
- Jaw thrust + CPAP with 100% O₂ at 20-30 cmH₂O via tight mask - may break incomplete laryngospasm
- Larson's manoeuvre: Apply firm pressure in the notch posterior to the mandibular condyle (Larson's point) bilaterally
- If SpO₂ < 90% and not responding: Propofol 0.5-1 mg/kg IV (small dose often breaks laryngospasm)
- If complete laryngospasm/hypoxia not resolving: Succinylcholine 1-2 mg/kg IV (or 4 mg/kg IM if no IV access) to achieve complete relaxation → bag-mask ventilate → re-intubate
- Atropine if bradycardia accompanies (suxamethonium + hypoxia = bradycardia in children)
PART 5: POSTOPERATIVE ANAESTHESIA MANAGEMENT
SECTION 18: RECOVERY ROOM (PACU) MANAGEMENT
- Procedure performed, duration, any intraoperative events
- Drugs given (opioids, antiemetics, antibiotics)
- Blood loss and fluids administered
- Type of reversal
- Specific instructions: keep head elevated 30°, avoid vomiting, watch for facial nerve palsy
- SpO₂, HR, BP, RR, EtCO₂ (if still intubated)
- Temperature
- Pain score (Wong-Baker FACES scale or NRS for 12-year-old)
- Level of consciousness (Aldrete score → target ≥9 before discharge)
| Parameter | Score 2 | Score 1 | Score 0 |
|---|---|---|---|
| Activity | Moves 4 limbs | Moves 2 limbs | No movement |
| Respiration | Breathes deeply, coughs | Dyspnoea/limited | Apnoeic |
| Circulation | BP ±20% pre-op | BP ±20-50% pre-op | BP ±50% pre-op |
| Consciousness | Fully awake | Arousable | Not responsive |
| SpO₂ | >92% room air | >90% with O₂ | <90% with O₂ |
SECTION 19: POSTOPERATIVE ANALGESIA
| Drug | Dose | Route | Frequency |
|---|---|---|---|
| Paracetamol | 15 mg/kg | IV/oral | q6h (max 60 mg/kg/day) |
| Ibuprofen (NSAID) | 10 mg/kg | Oral | q8h (if no contraindications) |
| Tramadol | 1-2 mg/kg | IV/oral | q6h PRN (for moderate pain) |
| Morphine | 0.05-0.1 mg/kg | IV | PRN for severe pain |
- Source: Scott-Brown's - "Post-operative pain is relatively low and is well managed with paracetamol and NSAIDs except in the mastoidectomy group when opioid analgesia is required."
- Mastoidectomy with significant bone drilling can cause moderate-to-severe pain - anticipate opioid requirements
- Avoid NSAIDS if there is concern about bleeding or renal function
SECTION 20: PONV MANAGEMENT IN THE POSTOPERATIVE PERIOD
- Non-smoker: +1
- Middle ear surgery: independent risk factor
- Post-op opioid use: +1
- Ondansetron 0.1 mg/kg IV at end of surgery
- Dexamethasone 0.1 mg/kg IV at induction
- Repeat ondansetron 0.1 mg/kg IV (if >6 hours since last dose)
- Metoclopramide 0.15 mg/kg IV (dopamine antagonist - avoid in children <1 year, risk of extrapyramidal effects)
- Promethazine 0.25-0.5 mg/kg IM (antihistamine - sedating, avoid in young children, use cautiously)
- Droperidol 0.01-0.015 mg/kg IV (butyrophenone - effective but watch QT prolongation)
"The child is vomiting repeatedly in the PACU. You have already given ondansetron. What next?"
- Rule out surgical causes: haematoma, cerebrospinal fluid leak (rare but can cause vomiting)
- Rule out pain as a driver of PONV (pain stimulates vomiting)
- Ensure adequate hydration - IV fluids
- Switch antiemetic class - if ondansetron (5-HT3 antagonist) has failed, use a different class:
- Dexamethasone (if not already given maximum dose)
- Droperidol 0.01 mg/kg IV
- Scopolamine transdermal patch (limited in paediatrics)
- TIVA was intended to prevent this - if volatile was used, consider this factor
- Keep the child in lateral position to reduce aspiration risk
- Head elevated 30°
- Inform the surgeon - repeated vomiting risks graft displacement and wound haematoma
SECTION 21: SPECIFIC POSTOPERATIVE CONCERNS
1. Postoperative Vertigo
- Common after inner ear manipulation
- Reassure patient and parents
- Ambulate slowly and only when stable
- Source: Morgan and Mikhail - "Patients undergoing ear surgery should be carefully assessed for vertigo postoperatively, and their ambulation should be closely monitored to minimise the risk of falling."
2. Facial Nerve Palsy
- Document facial nerve function BEFORE surgery (preoperative baseline)
- Compare postoperatively - if new facial palsy present, inform surgeon immediately
- May be due to surgical trauma, oedema, or infiltration of local anaesthetic
- If immediate and complete: suggests surgical injury → return to OT
- If delayed and partial: post-operative oedema → expectant management, steroids
3. Bleeding and Haematoma
- Monitor wound dressings
- Ear dressing/mastoid pressure bandage assessed every hour
- Blood on pillow or saturated dressing → call surgeon
- Significant haematoma → return to OT for evacuation
4. Hearing Assessment
- Audiometry at 6-8 weeks post-operatively to document hearing improvement
"What are the indications to return to the operating theatre (re-exploration) in the post-operative period?"
- Haematoma causing wound expansion, airway compromise, or significant blood loss
- Facial nerve palsy that is immediate and complete (suggests direct injury - surgical emergency)
- CSF leak detected (otorrhoea of clear fluid) not resolving
- Acute hearing loss suggesting ossicular displacement
- Wound dehiscence with exposure of underlying structures
- Signs of intracranial complication - new neurological deficit, signs of raised ICP (though rare)
- From anaesthetic standpoint: this is now a semi-urgent/urgent return to OT on a child who has already received anaesthesia - full stomach precautions must be considered if return is within 6-8 hours of last operation (impaired gastric motility, opioid effect, pain/fear slows gastric emptying). RSI (Rapid Sequence Induction) would be warranted.
PART 6: SPECIAL TOPICS AND ADDITIONAL VIVA QUESTIONS
"What is the significance of a cholesteatoma in this patient from an anaesthetic standpoint?"
- Intracranial extension: can erode into posterior fossa → meningitis, brain abscess, sigmoid sinus thrombosis → preoperatively assess for intracranial complications
- Dural plate erosion: risk of CSF leak or pneumocephalus intraoperatively
- Facial nerve canal erosion: mandatory facial nerve monitoring
- Tegmen erosion: risk of meningoencephalocele
- Sigmoid sinus erosion: catastrophic venous haemorrhage risk
- CT temporal bone is mandatory to map extent before surgery
- These complications change the ASA status and surgical risk significantly
"Briefly outline the anaesthetic considerations specific to a 12-year-old vs an adult for the same surgery."
| Aspect | Paediatric (12-year-old) | Adult |
|---|---|---|
| Airway anatomy | More anterior larynx, larger head, shorter neck | More predictable airway anatomy |
| ETT | Cuffed 6.5 mm; uncuffed 7.0 mm | Standard cuffed 7.5-8.0 mm |
| Drug doses | All weight-based | Fixed adult doses with ranges |
| Fluids | Holliday-Segar maintenance; careful to avoid overload | Standard formulas |
| Temperature regulation | More prone to hypothermia (larger BSA:weight ratio) | Less susceptible |
| Fasting | More risky if prolonged (hypoglycaemia) | Better tolerated |
| Blood volume | 70-80 mL/kg | 65-75 mL/kg |
| NPO | Clear fluids allowed up to 2h | Same (2h clear, 6h solids) |
| PONV | Higher incidence than adults; middle ear surgery compound risk | Apfel score guides prophylaxis |
| Consent | Parent/guardian; assent from child if old enough | Patient consent directly |
| Psychological prep | Child life specialist, play therapy, parental presence at induction | Standard consent/anxiolysis |
| MAC of volatiles | Higher in children (sevoflurane MAC 2.6 at age 12 vs 2.0 in adults) | Lower |
"What is your plan if the child refuses IV cannulation and is in tears preoperatively?"
- EMLA cream (eutectic mixture of lidocaine 2.5% + prilocaine 2.5%) applied under occlusive dressing to dorsum of hand/antecubital fossa 60-90 minutes before induction → numbs the skin
- Oral midazolam 0.5 mg/kg (max 15 mg) as premedication → excellent anxiolysis and compliance
- Inhalational induction with sevoflurane (up to 8%) in oxygen via face mask is the traditional paediatric technique - child breathes down to Stage 3 anaesthesia, then IV cannula placed
- Parental presence at induction - reduces anxiety significantly in children
- Distraction techniques - tablet/video games in the anaesthetic room
- Important caveat: For ear surgery specifically, once cannula is in and IV induction done, we transition to TIVA + avoid volatile maintenance to avoid PONV and avoid N₂O
"Describe your pain assessment tool for this 12-year-old in the PACU."
- NRS (Numerical Rating Scale) 0-10: "Tell me your pain on a scale of 0 to 10." Reliable from age 8+. Most commonly used.
- Wong-Baker FACES Pain Scale: 6 faces from 0 (no pain) to 10 (worst pain). Useful for ages 3-18. Visual, does not require numeracy.
- VAS (Visual Analogue Scale): 10 cm line - reliable from age 8+
- FLACC scale (Face, Legs, Activity, Cry, Consolability): for non-verbal or sedated children; not needed here as child is 12 and verbal
- Target: NRS ≤3 before PACU discharge
- Important: Always use the same scale for serial assessments to track trends reliably
"Sum up the five key anaesthetic take-home points for this case."
-
No Nitrous Oxide - middle ear surgery with tympanic membrane graft is an absolute contraindication to N₂O due to middle ear pressure dynamics and risk of graft displacement
-
TIVA is preferred - propofol-remifentanil TIVA reduces PONV, provides titratable controlled hypotension, avoids N₂O, and allows rapid, smooth recovery - critical for protecting the surgical repair
-
PONV prophylaxis is mandatory - dual antiemetic prophylaxis (dexamethasone + ondansetron) at induction; PONV threatens graft integrity and risks aspiration in a sedated, head-bandaged child
-
Facial nerve monitoring - confirm with surgeon before using NMBs; if NIM in use, neuromuscular blockade is contraindicated intraoperatively; this must be communicated before the first knife cut
-
Smooth emergence = protected graft - coughing, straining, and bucking on the ETT raises venous pressure and risks bleeding and graft displacement; deep extubation, lidocaine, or low-dose remifentanil at emergence protects the surgical result
PART 7: CASE SUMMARY TABLE
| Phase | Key Points |
|---|---|
| Preop | ASA I, 32 kg; TIVA consent; crossmatch blood; NPO 6h solids/2h clear; Hb >10; CT temporal bone; premedicate with oral midazolam + paracetamol |
| Induction | Pre-oxygenate; fentanyl + propofol + atracurium/rocuronium; cuffed 6.5 mm RAE tube; confirm bilateral BS + EtCO₂; eyes padded |
| Maintenance | TIVA (propofol + remifentanil); NO N₂O; oxygen in air; BIS 40-60; controlled hypotension MAP 50-65; 15° head-up; confirm facial nerve monitoring plan |
| Emergence | Deep extubation preferred; lidocaine 1 mg/kg or low-dose remifentanil infusion; lateral positioning; ondansetron at end |
| Postop | Multimodal analgesia (paracetamol + NSAID ± tramadol); dual antiemetic prophylaxis; head 30° elevation; watch for: PONV, haematoma, facial palsy, vertigo; Aldrete ≥9 before discharge |
Professor's Final Words to the Candidate:"You have now presented a complete anaesthetic long case. Remember - in the exam, precision and safety thinking matter more than textbook recitation. When the examiner asks 'what would you do?', the answer must always protect your patient first. The moment you anchor your management to patient safety, the examiner knows you are a clinician, not just a student.One more thing: always close your case presentation by saying - 'I would like to re-examine the child in the anaesthetic room immediately before induction to confirm no interval changes, re-check fasting status, and obtain a final verbal assent from the child.' That statement alone tells the examiner you understand that anaesthesia begins before the first drug is given."
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Chapter on Ear Surgery, N₂O and ear surgery
- Miller's Anesthesia, 10e - Ear Surgery, Paediatric Anaesthesia
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Ear Surgery, TIVA, PONV
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Paediatric assessment
- Cummings Otolaryngology - Middle ear surgery anaesthesia considerations
Generate a PPTX presentation with this case for class teaching
mkdir -p /home/daytona/workspace/csom-anaesthesia-pptx && ls /home/daytona/workspace/
~/csom-anaesthesia-pptx/generate.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.author = "Department of Anaesthesiology";
pres.title = "Anaesthesia for Tympanomastoidectomy in a Child";
// ── COLOR PALETTE ─────────────────────────────────────────────────────────────
// Deep navy dominates, teal accent, white text, warm amber highlights
const C = {
navy: "0A1628", // dominant dark bg
navyMid: "0E2040", // mid tone
teal: "1A9B8A", // accent
tealDark: "127A6D",
tealPale: "D0F0EB",
amber: "F0A500",
white: "FFFFFF",
offWhite: "EEF4F7",
gray: "8FA3B1",
grayLight:"C8D8E0",
red: "E84040",
green: "27AE60",
};
// ── HELPERS ───────────────────────────────────────────────────────────────────
function addSlideNumber(slide, num, total) {
slide.addText(`${num} / ${total}`, {
x: 9.3, y: 5.3, w: 0.6, h: 0.2,
fontSize: 9, color: C.gray, align: "right",
});
}
function sectionHeader(slide, title, subtitle) {
// Full-bleed dark bg
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
// Teal accent bar left
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.08, h: 5.625, fill: { color: C.teal } });
// Decorative circle
slide.addShape(pres.shapes.OVAL, { x: 7.8, y: -1.2, w: 3.5, h: 3.5, fill: { color: C.navyMid }, line: { color: C.teal, width: 1.5 } });
slide.addText(title, {
x: 0.55, y: 1.9, w: 7, h: 1.0,
fontSize: 34, bold: true, color: C.white, fontFace: "Calibri Light",
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.55, y: 2.95, w: 7, h: 0.55,
fontSize: 16, color: C.teal, fontFace: "Calibri",
});
}
}
function contentSlide(slide) {
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.07, fill: { color: C.teal } });
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.55, w: 10, h: 0.075, fill: { color: C.navy } });
}
function slideTitle(slide, title) {
slide.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.07, w: 10, h: 0.7, fill: { color: C.navy } });
slide.addText(title, {
x: 0.3, y: 0.1, w: 9.4, h: 0.62,
fontSize: 18, bold: true, color: C.white, fontFace: "Calibri", valign: "middle",
});
}
function tealBadge(slide, label, x, y, w) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w, h: 0.32, fill: { color: C.teal }, rectRadius: 0.05,
});
slide.addText(label, {
x, y, w, h: 0.32, fontSize: 10, bold: true, color: C.white,
align: "center", valign: "middle",
});
}
function amberBadge(slide, label, x, y, w) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w, h: 0.32, fill: { color: C.amber }, rectRadius: 0.05,
});
slide.addText(label, {
x, y, w, h: 0.32, fontSize: 10, bold: true, color: C.navy,
align: "center", valign: "middle",
});
}
function vivaBox(slide, question, answer, x, y, w, h) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y, w, h, fill: { color: C.navyMid }, rectRadius: 0.1,
shadow: { type: "outer", color: "000000", blur: 8, offset: 2, angle: 135, opacity: 0.2 },
});
slide.addText("Q: " + question, {
x: x + 0.15, y: y + 0.1, w: w - 0.3, h: 0.35,
fontSize: 10, bold: true, color: C.amber, fontFace: "Calibri",
});
slide.addShape(pres.shapes.RECTANGLE, { x: x + 0.15, y: y + 0.46, w: w - 0.3, h: 0.02, fill: { color: C.teal } });
slide.addText(answer, {
x: x + 0.15, y: y + 0.5, w: w - 0.3, h: h - 0.65,
fontSize: 9, color: C.white, fontFace: "Calibri",
});
}
function bullets(items) {
return items.map((t, i) => ({
text: t,
options: { bullet: { code: "2022" }, breakLine: i < items.length - 1, fontSize: 12, color: C.navy },
}));
}
function bulletsTeal(items) {
return items.map((t, i) => ({
text: t,
options: { bullet: { code: "25B6" }, breakLine: i < items.length - 1, fontSize: 11, color: C.navyMid },
}));
}
// ═══════════════════════════════════════════════════════════════════
// TOTAL SLIDES: 28
// ═══════════════════════════════════════════════════════════════════
const TOTAL = 28;
// ── SLIDE 1: TITLE ───────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
// Large decorative circle top-right
s.addShape(pres.shapes.OVAL, { x: 6.5, y: -1.5, w: 5, h: 5, fill: { color: C.navyMid }, line: { color: C.teal, width: 2 } });
// Small circle accent
s.addShape(pres.shapes.OVAL, { x: 8.6, y: 3.8, w: 1.8, h: 1.8, fill: { color: C.tealDark } });
// Bottom teal bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.15, w: 10, h: 0.475, fill: { color: C.teal } });
// Left accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.1, h: 5.625, fill: { color: C.teal } });
s.addText("ANAESTHESIA FOR", {
x: 0.4, y: 0.7, w: 7, h: 0.5,
fontSize: 14, color: C.teal, bold: true, charSpacing: 4, fontFace: "Calibri",
});
s.addText("Tympanomastoidectomy", {
x: 0.4, y: 1.2, w: 8, h: 1.0,
fontSize: 36, bold: true, color: C.white, fontFace: "Calibri Light",
});
s.addText("in a Paediatric Patient", {
x: 0.4, y: 2.2, w: 7, h: 0.6,
fontSize: 22, color: C.grayLight, fontFace: "Calibri Light",
});
s.addText([
{ text: "Case: ", options: { bold: true, color: C.amber } },
{ text: "12-year-old boy | CSOM | Elective Surgery", options: { color: C.white } },
], { x: 0.4, y: 3.0, w: 8, h: 0.4, fontSize: 13 });
s.addText([
{ text: "Long Case Presentation ", options: { bold: true, color: C.white } },
{ text: "MD Anaesthesia Final Practical Exam", options: { color: C.grayLight } },
], { x: 0.4, y: 5.18, w: 9, h: 0.38, fontSize: 12, valign: "middle" });
}
// ── SLIDE 2: LEARNING OBJECTIVES ─────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Learning Objectives");
const objs = [
"Present a structured long case of a child with CSOM planned for tympanomastoidectomy",
"Discuss preoperative assessment and optimisation specific to this case",
"Outline a safe intraoperative anaesthesia plan — with rationale for every key decision",
"Explain why TIVA and NO nitrous oxide are the cornerstones of anaesthetic management",
"Manage PONV, controlled hypotension, and facial nerve monitoring considerations",
"Handle postoperative analgesia, recovery, and potential complications",
"Answer high-yield viva questions at every stage of management",
];
objs.forEach((obj, i) => {
const yPos = 0.95 + i * 0.63;
s.addShape(pres.shapes.OVAL, { x: 0.22, y: yPos + 0.05, w: 0.28, h: 0.28, fill: { color: C.teal } });
s.addText(`${i + 1}`, {
x: 0.22, y: yPos + 0.05, w: 0.28, h: 0.28,
fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle",
});
s.addText(obj, {
x: 0.65, y: yPos, w: 9.0, h: 0.42,
fontSize: 11.5, color: C.navyMid, fontFace: "Calibri", valign: "middle",
});
});
addSlideNumber(s, 2, TOTAL);
}
// ── SLIDE 3: CASE AT A GLANCE ─────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Case at a Glance");
// Patient info card
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.3, y: 0.9, w: 4.2, h: 4.4, fill: { color: C.navyMid }, rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 8, offset: 2, angle: 135, opacity: 0.2 },
});
s.addText("PATIENT PROFILE", {
x: 0.5, y: 1.0, w: 3.8, h: 0.35,
fontSize: 11, bold: true, color: C.teal, charSpacing: 3, align: "center",
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.5, y: 1.35, w: 3.8, h: 0.03, fill: { color: C.teal } });
const patientDetails = [
["Age", "12 years"],
["Sex", "Male"],
["Weight", "~32 kg"],
["Diagnosis", "CSOM (Right ear)"],
["Procedure", "Tympanomastoidectomy"],
["ASA Status", "ASA I"],
["Surgery Type", "Elective"],
];
patientDetails.forEach(([label, val], i) => {
const y = 1.5 + i * 0.48;
s.addText(label + ":", { x: 0.55, y, w: 1.4, h: 0.38, fontSize: 10.5, color: C.grayLight, bold: true, valign: "middle" });
s.addText(val, { x: 2.0, y, w: 2.3, h: 0.38, fontSize: 10.5, color: C.white, valign: "middle" });
});
// Right side: key anaesthetic flags
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 4.8, y: 0.9, w: 4.9, h: 4.4, fill: { color: C.offWhite }, rectRadius: 0.12,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.1 },
});
s.addText("KEY ANAESTHETIC FLAGS", {
x: 5.0, y: 1.0, w: 4.5, h: 0.35,
fontSize: 11, bold: true, color: C.navy, charSpacing: 3, align: "center",
});
s.addShape(pres.shapes.RECTANGLE, { x: 5.0, y: 1.35, w: 4.5, h: 0.03, fill: { color: C.amber } });
const flags = [
["NO Nitrous Oxide", "red", "Middle ear graft — pressure risk"],
["TIVA Preferred", "teal", "Propofol + Remifentanil"],
["PONV High Risk", "red", "Dual prophylaxis mandatory"],
["Facial Nerve Monitor", "amber", "No relaxants if NIM in use"],
["Deep Extubation", "teal", "Prevent cough on ETT"],
["Paediatric Dosing", "amber", "All drugs are weight-based"],
];
const flagColors = { red: C.red, teal: C.teal, amber: C.amber };
flags.forEach(([title, col, sub], i) => {
const y = 1.5 + i * 0.63;
s.addShape(pres.shapes.RECTANGLE, { x: 5.0, y: y + 0.08, w: 0.06, h: 0.32, fill: { color: flagColors[col] } });
s.addText(title, { x: 5.2, y, w: 2.5, h: 0.28, fontSize: 11, bold: true, color: C.navy, valign: "bottom" });
s.addText(sub, { x: 5.2, y: y + 0.28, w: 4.2, h: 0.25, fontSize: 9.5, color: C.gray, valign: "top" });
});
addSlideNumber(s, 3, TOTAL);
}
// ── SLIDE 4: SECTION HEADER — PREOPERATIVE ────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "SECTION 1\nPreoperative Assessment", "History · Examination · Investigations · Optimisation");
s.addShape(pres.shapes.RECTANGLE, { x: 0.55, y: 1.85, w: 2.5, h: 0.07, fill: { color: C.teal } });
}
// ── SLIDE 5: HISTORY ──────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "History — Chief Complaint & HPI");
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 4.6, h: 4.45, fill: { color: C.navyMid }, rectRadius: 0.1 });
tealBadge(s, "CHIEF COMPLAINTS", 0.45, 0.98, 2.5);
s.addText([
...bullets([
"Persistent ear discharge — years duration",
"Decreased hearing (affected ear)",
"Occasional earache & headache",
"No facial palsy",
"No vertigo",
])
], { x: 0.45, y: 1.38, w: 4.2, h: 3.7, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 0.9, w: 4.6, h: 4.45, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "ANAESTHETIC RELEVANCE", 5.35, 0.98, 3.0);
s.addText([
...bulletsTeal([
"No facial palsy → no facial canal erosion",
"No headache/neck stiffness → no intracranial extension",
"No previous anaesthesia → no known reactions",
"No family h/o adverse reactions (MH screen)",
"No NKDA — note clearly in chart",
"CSOM = obstructed Eustachian tube",
"→ N₂O will NOT vent → CONTRAINDICATED",
])
], { x: 5.35, y: 1.38, w: 4.2, h: 3.7, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
addSlideNumber(s, 5, TOTAL);
}
// ── SLIDE 6: AIRWAY ASSESSMENT ────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Airway Assessment — The Anaesthetist's Priority");
const rows = [
["Parameter", "Finding", "Grade"],
["Mouth opening", ">4 cm (>3 finger-breadths)", "✓ Adequate"],
["Mallampati class", "Class I–II", "✓ Easy intubation"],
["Thyromental distance", ">6.5 cm (>3 FB)", "✓ Adequate"],
["Neck mobility", "Full range", "✓ Unrestricted"],
["ULBT (jaw protrusion)", "Class A", "✓ Favourable"],
["Loose teeth", "Check permanent dentition", "Document"],
["Tonsil size", "Grade I–II", "Note if enlarged"],
["Predicted CL grade", "Grade I–II", "Easy laryngoscopy"],
];
const colW = [2.9, 3.4, 2.5];
const colX = [0.25, 3.2, 6.65];
const rowH = 0.46;
rows.forEach((row, ri) => {
const y = 0.9 + ri * rowH;
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const bg = isHeader ? C.navy : (ri % 2 === 0 ? C.white : C.offWhite);
s.addShape(pres.shapes.RECTANGLE, { x: colX[ci], y, w: colW[ci], h: rowH, fill: { color: bg }, line: { color: C.grayLight, width: 0.5 } });
const textColor = isHeader ? C.white : (ci === 2 ? (cell.includes("✓") ? C.tealDark : C.amber) : C.navyMid);
s.addText(cell, {
x: colX[ci] + 0.1, y, w: colW[ci] - 0.2, h: rowH,
fontSize: isHeader ? 11 : 10.5, bold: isHeader, color: textColor, valign: "middle",
});
});
});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y: 5.1, w: 9.5, h: 0.37, fill: { color: C.teal }, rectRadius: 0.05,
});
s.addText("Predicted: NOT DIFFICULT AIRWAY — Proceed with standard oral RAE tube (cuffed 6.5 mm) + video laryngoscope on standby", {
x: 0.35, y: 5.1, w: 9.3, h: 0.37,
fontSize: 10.5, color: C.white, bold: true, valign: "middle",
});
addSlideNumber(s, 6, TOTAL);
}
// ── SLIDE 7: INVESTIGATIONS ───────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Preoperative Investigations");
const inv = [
["Haemoglobin", "Target >10 g/dL", "Blood loss risk during mastoid drilling"],
["Blood group & X-match", "1–2 units RBC reserved", "Sigmoid sinus injury risk"],
["BT / CT / PT-INR", "Within normal limits", "Microsurgery — no coagulopathy"],
["RBS", "Normal", "Paediatric glucose monitoring"],
["Electrolytes", "Normal", "Fluid management reference"],
["ECG", "NSR — not mandatory ASA I", "Done if clinically indicated"],
["CT Temporal Bone", "Extent of CSOM, facial canal", "Guides surgical + anaes planning"],
["Pure Tone Audiogram", "Conductive hearing loss", "Surgical documentation"],
];
const colW2 = [2.0, 2.5, 5.2];
const colX2 = [0.25, 2.3, 4.85];
const headers2 = ["Investigation", "Expected Finding", "Anaesthetic Relevance"];
headers2.forEach((h, ci) => {
s.addShape(pres.shapes.RECTANGLE, { x: colX2[ci], y: 0.9, w: colW2[ci], h: 0.42, fill: { color: C.teal }, line: { color: C.tealDark, width: 0.5 } });
s.addText(h, { x: colX2[ci] + 0.1, y: 0.9, w: colW2[ci] - 0.2, h: 0.42, fontSize: 11, bold: true, color: C.white, valign: "middle" });
});
inv.forEach((row, ri) => {
const y = 1.32 + ri * 0.5;
row.forEach((cell, ci) => {
const bg = ri % 2 === 0 ? C.white : C.offWhite;
s.addShape(pres.shapes.RECTANGLE, { x: colX2[ci], y, w: colW2[ci], h: 0.5, fill: { color: bg }, line: { color: C.grayLight, width: 0.5 } });
s.addText(cell, { x: colX2[ci] + 0.1, y, w: colW2[ci] - 0.2, h: 0.5, fontSize: 10, color: C.navyMid, valign: "middle" });
});
});
addSlideNumber(s, 7, TOTAL);
}
// ── SLIDE 8: NPO & PREMEDICATION ─────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Fasting Guidelines & Premedication");
// NPO left
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 4.6, h: 4.45, fill: { color: C.navyMid }, rectRadius: 0.1 });
tealBadge(s, "ASA NPO GUIDELINES (2023)", 0.45, 0.98, 3.8);
const npoItems = [
["Clear liquids (water, juice)", "2 hours"],
["Breast milk", "4 hours"],
["Formula / light meal", "6 hours"],
["Full / fatty meal", "8 hours"],
];
npoItems.forEach(([item, time], i) => {
const y = 1.5 + i * 0.7;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.45, y, w: 3.7, h: 0.58, fill: { color: C.navy }, rectRadius: 0.06 });
s.addText(item, { x: 0.6, y: y + 0.02, w: 2.5, h: 0.3, fontSize: 10, color: C.white, valign: "bottom" });
s.addText(time, { x: 3.1, y: y + 0.02, w: 0.9, h: 0.54, fontSize: 14, bold: true, color: C.amber, align: "center", valign: "middle" });
});
s.addText("⚠ Prolonged fasting → hypoglycaemia in children\nAllow clear fluids up to 2h before induction", {
x: 0.45, y: 4.38, w: 4.1, h: 0.65, fontSize: 9.5, color: C.amber, fontFace: "Calibri",
});
// Premedication right
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 0.9, w: 4.6, h: 4.45, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "PREMEDICATION (32 kg child)", 5.35, 0.98, 3.4);
const premed = [
["Midazolam", "0.5 mg/kg oral (max 15 mg)", "Anxiolysis / amnesia"],
["Paracetamol", "15 mg/kg oral/rectal", "Pre-emptive analgesia"],
["Ondansetron", "0.1 mg/kg IV at induction", "PONV prophylaxis"],
["Dexamethasone", "0.1 mg/kg IV at induction", "PONV + anti-inflam"],
["Atropine", "0.02 mg/kg IV at induction", "Antisialagogue"],
];
premed.forEach(([drug, dose, purpose], i) => {
const y = 1.5 + i * 0.72;
s.addShape(pres.shapes.RECTANGLE, { x: 5.25, y: y + 0.1, w: 0.05, h: 0.3, fill: { color: C.teal } });
s.addText(drug, { x: 5.45, y, w: 1.5, h: 0.3, fontSize: 11, bold: true, color: C.navy, valign: "bottom" });
s.addText(dose, { x: 5.45, y: y + 0.3, w: 2.8, h: 0.25, fontSize: 9.5, color: C.navyMid });
s.addText(purpose, { x: 5.45, y: y + 0.48, w: 4.1, h: 0.22, fontSize: 9, color: C.gray });
});
addSlideNumber(s, 8, TOTAL);
}
// ── SLIDE 9: VIVA — NPO & N2O ────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.08, h: 5.625, fill: { color: C.amber } });
s.addText("VIVA QUESTIONS — Preoperative", {
x: 0.3, y: 0.18, w: 9, h: 0.45,
fontSize: 16, bold: true, color: C.amber, charSpacing: 2,
});
vivaBox(s,
"Clear fluids last given at what time if surgery is at 10 AM?",
"8 AM — clear fluids are permitted up to 2 hours before induction per ASA 2023 NPO guidelines. Solids stopped at midnight (10 h prior). Gastric ultrasound may confirm emptying if in doubt.",
0.25, 0.75, 9.5, 1.4);
vivaBox(s,
"Why is N₂O contraindicated in tympanomastoidectomy?",
"N₂O is 20× more soluble in blood than nitrogen. It diffuses into the closed middle ear cavity faster than N₂ escapes, raising pressure. This displaces the TM graft. CSOM patients have obstructed Eustachian tubes — cannot passively vent pressure. Even stopping N₂O after graft placement creates negative pressure → graft dislodgement. Avoid entirely or wash out 15–30 min before graft.",
0.25, 2.3, 9.5, 1.65);
vivaBox(s,
"Why is family history of anaesthesia complications relevant?",
"Malignant hyperthermia (MH) is autosomal dominant, triggered by volatile agents and succinylcholine. Positive family history mandates TIVA — avoiding all volatile agents and succinylcholine. Incidence ~1:10,000–50,000 anaesthetics. A TIVA plan already being considered for this case eliminates MH trigger risk.",
0.25, 4.1, 9.5, 1.35);
addSlideNumber(s, 9, TOTAL);
}
// ── SLIDE 10: SECTION HEADER — INTRAOPERATIVE ────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "SECTION 2\nIntraoperative Management", "Induction · Maintenance · Monitoring · Controlled Hypotension");
s.addShape(pres.shapes.RECTANGLE, { x: 0.55, y: 1.8, w: 2.5, h: 0.07, fill: { color: C.teal } });
}
// ── SLIDE 11: INDUCTION ───────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Induction of Anaesthesia — TIVA Protocol");
// Left: steps
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 5.1, h: 4.45, fill: { color: C.navyMid }, rectRadius: 0.1 });
tealBadge(s, "INDUCTION SEQUENCE (32 kg)", 0.4, 0.98, 3.8);
const steps = [
["1", "Pre-oxygenate", "100% O₂ × 3–5 min via tight-fitting mask"],
["2", "Fentanyl 2 mcg/kg IV", "= 64 mcg (give slowly over 60 sec)"],
["3", "Propofol 2–2.5 mg/kg IV", "= 64–80 mg (over 60–90 sec)"],
["4", "Atracurium 0.5 mg/kg IV", "= 16 mg | OR Rocuronium 0.6 mg/kg"],
["5", "Wait full relaxation 3 min", "Confirm with nerve stimulator / TOF"],
["6", "Laryngoscopy + intubation", "Cuffed oral RAE 6.5 mm, Macintosh 3"],
["7", "Confirm position", "Bilateral BS + capnograph waveform"],
];
steps.forEach(([num, action, detail], i) => {
const y = 1.5 + i * 0.54;
s.addShape(pres.shapes.OVAL, { x: 0.4, y: y + 0.04, w: 0.3, h: 0.3, fill: { color: C.teal } });
s.addText(num, { x: 0.4, y: y + 0.04, w: 0.3, h: 0.3, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle" });
s.addText(action, { x: 0.82, y, w: 2.0, h: 0.3, fontSize: 10, bold: true, color: C.white, valign: "bottom" });
s.addText(detail, { x: 0.82, y: y + 0.28, w: 4.3, h: 0.24, fontSize: 9, color: C.grayLight });
});
// Right: ETT choice
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.6, y: 0.9, w: 4.15, h: 2.4, fill: { color: C.teal }, rectRadius: 0.1 });
s.addText("ETT SELECTION", { x: 5.8, y: 0.98, w: 3.8, h: 0.35, fontSize: 12, bold: true, color: C.navy, align: "center" });
s.addText([
{ text: "Formula: ", options: { bold: true, color: C.navy } },
{ text: "Age/4 + 4 = 7.0 mm (uncuffed)\n", options: { color: C.white } },
{ text: "Cuffed tube: ", options: { bold: true, color: C.navy } },
{ text: "6.5 mm (preferred)\n", options: { color: C.white } },
{ text: "Tube type: ", options: { bold: true, color: C.navy } },
{ text: "Oral RAE (south-facing preformed)\n", options: { color: C.white } },
{ text: "Have ready: ", options: { bold: true, color: C.navy } },
{ text: "6.0, 6.5, 7.0 mm sizes", options: { color: C.white } },
], { x: 5.8, y: 1.38, w: 3.75, h: 1.75, fontSize: 10.5, fontFace: "Calibri", lineSpacingMultiple: 1.5 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.6, y: 3.5, w: 4.15, h: 1.85, fill: { color: C.offWhite }, rectRadius: 0.1 });
s.addText("WHY AVOID SUCCINYLCHOLINE?", { x: 5.8, y: 3.58, w: 3.8, h: 0.3, fontSize: 10, bold: true, color: C.red, align: "center" });
s.addText([
...bulletsTeal([
"MH trigger (autosomal dominant risk)",
"Fasciculations → ↑IOP, ↑intragastric P",
"Rocuronium + sugammadex = safer alternative",
"Elective case with predicted easy airway",
])
], { x: 5.75, y: 3.95, w: 3.85, h: 1.25, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
addSlideNumber(s, 11, TOTAL);
}
// ── SLIDE 12: POSITIONING & EYES ─────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Patient Positioning — Details Matter");
const posItems = [
["Supine + head turned", "Head turned away from surgical ear; secured in head ring"],
["15° reverse Trendelenburg", "Head-up tilt — reduces venous pooling, decreases bleeding"],
["Eyes padded bilaterally", "Corneal abrasion from drapes; pressure on dependent eye"],
["ETT secured away from field", "Confirm no tube kink after final head position; check EtCO₂ + air pressures"],
["Arms tucked by sides", "Surgeon needs unobstructed access from head-end"],
["Temperature maintenance", "Warm OR, warm IV fluids, forced-air warming blanket — paediatrics lose heat rapidly"],
["Nerve integrity monitor", "NIM ETT if facial nerve monitoring planned — confirm with surgeon PRE-INDUCTION"],
];
posItems.forEach(([title, detail], i) => {
const y = 0.92 + i * 0.64;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y, w: 9.5, h: 0.56, fill: { color: i % 2 === 0 ? C.white : C.offWhite }, rectRadius: 0.05, line: { color: C.grayLight, width: 0.5 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.25, y, w: 0.06, h: 0.56, fill: { color: i % 2 === 0 ? C.teal : C.amber } });
s.addText(title, { x: 0.44, y: y + 0.04, w: 2.6, h: 0.26, fontSize: 10.5, bold: true, color: C.navyMid });
s.addText(detail, { x: 0.44, y: y + 0.28, w: 9.1, h: 0.24, fontSize: 10, color: C.gray });
});
addSlideNumber(s, 12, TOTAL);
}
// ── SLIDE 13: MAINTENANCE — TIVA ─────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Maintenance — TIVA (Preferred Technique)");
// Why TIVA box
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 4.6, h: 2.0, fill: { color: C.navy }, rectRadius: 0.1 });
s.addText("WHY TIVA?", { x: 0.45, y: 0.95, w: 4.2, h: 0.35, fontSize: 12, bold: true, color: C.teal });
s.addText([
...bullets([
"Avoids N₂O — mandatory in ear surgery",
"Propofol TIVA ↓ PONV vs volatile agents",
"Remifentanil enables controlled hypotension",
"Smooth, rapid, clear-headed emergence",
"No airway reactivity of volatile agents",
])
], { x: 0.45, y: 1.35, w: 4.2, h: 1.45, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
// Drugs infusion
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 0.9, w: 4.6, h: 2.0, fill: { color: C.teal }, rectRadius: 0.1 });
s.addText("TIVA INFUSION RATES", { x: 5.35, y: 0.95, w: 4.2, h: 0.35, fontSize: 12, bold: true, color: C.navy });
s.addText([
{ text: "Propofol:\n", options: { bold: true, color: C.navy, breakLine: true } },
{ text: "4–12 mg/kg/hr (TCI or manual)\n\n", options: { color: C.white, breakLine: true } },
{ text: "Remifentanil:\n", options: { bold: true, color: C.navy, breakLine: true } },
{ text: "0.05–0.25 mcg/kg/min\n\n", options: { color: C.white, breakLine: true } },
{ text: "Gas: O₂ in Air (FiO₂ 0.3–0.4) — NO N₂O", options: { bold: true, color: C.amber } },
], { x: 5.35, y: 1.35, w: 4.2, h: 1.45, fontSize: 10.5, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
// BIS monitoring
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 3.05, w: 4.6, h: 1.65, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "DEPTH OF ANAESTHESIA — BIS", 0.45, 3.13, 3.5);
s.addText([
...bulletsTeal([
"BIS target: 40–60 (adequate anaesthesia depth)",
"BIS >60 → risk of awareness → increase propofol",
"BIS <40 → too deep → reduce infusion",
])
], { x: 0.45, y: 3.5, w: 4.2, h: 1.1, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
// Ventilation
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 3.05, w: 4.6, h: 1.65, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "VENTILATION TARGETS", 5.35, 3.13, 3.0);
s.addText([
...bulletsTeal([
"TV 6–8 mL/kg = 190–255 mL; Rate 14–18/min",
"EtCO₂ target: 35–40 mmHg (normocapnia)",
"PEEP 3–5 cmH₂O — prevent atelectasis",
])
], { x: 5.35, y: 3.5, w: 4.2, h: 1.1, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
// Volatile alternative note
s.addShape(pres.shapes.RECTANGLE, { x: 0.25, y: 4.8, w: 9.5, h: 0.65, fill: { color: C.navyMid } });
s.addText("Alternative (if TIVA unavailable): Sevoflurane in O₂/Air (1.0–1.5 MAC) — NO N₂O. Increased PONV risk vs TIVA.", {
x: 0.4, y: 4.82, w: 9.2, h: 0.6, fontSize: 10.5, color: C.grayLight, valign: "middle",
});
addSlideNumber(s, 13, TOTAL);
}
// ── SLIDE 14: CONTROLLED HYPOTENSION ─────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Controlled Hypotension — Improving the Surgical Field");
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 9.5, h: 0.65, fill: { color: C.teal }, rectRadius: 0.08 });
s.addText("Target MAP: 50–65 mmHg (20–30% below patient baseline) — microsurgery demands bloodless field", {
x: 0.4, y: 0.9, w: 9.2, h: 0.65, fontSize: 12, bold: true, color: C.white, valign: "middle",
});
const methods = [
["Remifentanil infusion", "Primary agent: ↓SVR + ↓HR; ultra-short t½; most titratable"],
["Propofol TIVA", "Vasodilation + ↓CO; synergistic with remifentanil"],
["Esmolol infusion", "β₁ blockade → ↓HR; controls reflex tachycardia"],
["15° head-up tilt", "Simple non-pharmacological; reduces venous pooling"],
["Epinephrine 1:200,000", "Surgeon's local infiltration; local vasoconstriction"],
["Dexmedetomidine", "α₂ agonist → ↓sympathetic tone + opioid sparing"],
];
methods.forEach(([method, detail], i) => {
const y = 1.68 + i * 0.6;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y, w: 9.5, h: 0.52, fill: { color: i % 2 === 0 ? C.white : C.offWhite }, rectRadius: 0.05, line: { color: C.grayLight, width: 0.5 } });
s.addText(method, { x: 0.4, y, w: 2.5, h: 0.52, fontSize: 10.5, bold: true, color: C.navyMid, valign: "middle" });
s.addText(detail, { x: 3.0, y, w: 6.6, h: 0.52, fontSize: 10, color: C.navy, valign: "middle" });
});
// Contraindications
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 5.18, w: 9.5, h: 0.32, fill: { color: C.red }, rectRadius: 0.05 });
s.addText("Contraindicated in: Uncontrolled hypertension | Cerebrovascular disease | Severe anaemia | Renal insufficiency", {
x: 0.4, y: 5.18, w: 9.2, h: 0.32, fontSize: 10, bold: true, color: C.white, valign: "middle",
});
addSlideNumber(s, 14, TOTAL);
}
// ── SLIDE 15: VIVA — INTRAOPERATIVE ──────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.08, h: 5.625, fill: { color: C.amber } });
s.addText("VIVA QUESTIONS — Intraoperative", {
x: 0.3, y: 0.18, w: 9, h: 0.45, fontSize: 16, bold: true, color: C.amber, charSpacing: 2,
});
vivaBox(s,
"Surgeon injects epinephrine 1:50,000. You see sudden hypertension + VEs. What do you do?",
"Alert surgeon to stop further injection. Increase anaesthetic depth (propofol bolus). For VEs: lignocaine 1 mg/kg IV or esmolol 0.5 mg/kg IV. Correct ventilation (avoid hypercapnia). Note: sevoflurane sensitises myocardium less than halothane. Document and communicate.",
0.25, 0.75, 9.5, 1.5);
vivaBox(s,
"Surgeon asks for a muscle relaxant mid-surgery because patient moved. Your response?",
"First: ask surgeon — is facial nerve NIM monitoring in use? If YES, NMBs are absolutely contraindicated. If NO: increase anaesthetic depth first (propofol + remifentanil bolus). Check TOF — if fully recovered and patient still moves, anaesthesia is too light. Never reflexively give relaxant without understanding why patient moved.",
0.25, 2.4, 9.5, 1.65);
vivaBox(s,
"What is facial nerve monitoring and how does it change your anaesthetic plan?",
"NIM (Nerve Integrity Monitoring) detects facial nerve EMG signals when surgically stimulated. If in use: muscle relaxants must NOT be given post-intubation — paralysis abolishes EMG signal. Communicate with surgeon BEFORE induction. Plan: TIVA depth control replaces relaxants for immobility. TOF monitoring essential to confirm spontaneous recovery.",
0.25, 4.18, 9.5, 1.3);
addSlideNumber(s, 15, TOTAL);
}
// ── SLIDE 16: MONITORING ──────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Intraoperative Monitoring — Standards");
const monitors = [
["ECG (5-lead)", "HR, rhythm, ST changes, arrhythmia from epinephrine injection", C.teal],
["Pulse oximetry", "Oxygenation — continuous SpO₂; desaturation alert <95%", C.teal],
["NIBP (q 3–5 min)", "Haemodynamic monitoring; target MAP during controlled hypotension", C.teal],
["Capnography (EtCO₂)", "Ventilation adequacy; ETT confirmation; air embolism detection (early)", C.teal],
["Temperature probe", "Core temp — paediatric hypothermia is rapid; maintain >36°C", C.amber],
["Neuromuscular (TOF)", "NMB depth monitoring; confirm full recovery before extubation (TOF ratio >0.9)", C.amber],
["BIS monitor", "Depth of anaesthesia 40–60; prevents awareness under TIVA", C.amber],
["Urine output (if >3h)", "Foley catheter — target 0.5–1 mL/kg/hr; guides fluid management", C.amber],
["Arterial line (if deliberate hypotension)", "Beat-to-beat BP; ABG sampling — pH, lactate, glucose, Hb", C.red],
];
monitors.forEach(([monitor, detail, col], i) => {
const y = 0.93 + i * 0.52;
s.addShape(pres.shapes.RECTANGLE, { x: 0.25, y, w: 0.06, h: 0.44, fill: { color: col } });
s.addText(monitor, { x: 0.4, y: y + 0.02, w: 2.7, h: 0.26, fontSize: 10.5, bold: true, color: C.navyMid });
s.addText(detail, { x: 0.4, y: y + 0.26, w: 9.4, h: 0.22, fontSize: 9.5, color: C.gray });
if (i < monitors.length - 1) {
s.addShape(pres.shapes.RECTANGLE, { x: 0.25, y: y + 0.46, w: 9.5, h: 0.01, fill: { color: C.grayLight } });
}
});
addSlideNumber(s, 16, TOTAL);
}
// ── SLIDE 17: FLUID MANAGEMENT ───────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Fluid Management — 32 kg Paediatric Patient");
// Maintenance calculation
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 4.6, h: 2.5, fill: { color: C.navyMid }, rectRadius: 0.1 });
tealBadge(s, "MAINTENANCE — HOLLIDAY-SEGAR", 0.4, 0.97, 3.8);
s.addText([
{ text: "First 10 kg: ", options: { bold: true, color: C.amber } },
{ text: "4 mL/kg/hr = 40 mL/hr\n", options: { color: C.white, breakLine: true } },
{ text: "Next 10 kg: ", options: { bold: true, color: C.amber } },
{ text: "2 mL/kg/hr = 20 mL/hr\n", options: { color: C.white, breakLine: true } },
{ text: "Next 12 kg: ", options: { bold: true, color: C.amber } },
{ text: "1 mL/kg/hr = 12 mL/hr\n\n", options: { color: C.white, breakLine: true } },
{ text: "Total Maintenance = 72 mL/hr", options: { bold: true, color: C.teal } },
], { x: 0.45, y: 1.4, w: 4.2, h: 1.85, fontSize: 11, fontFace: "Calibri", lineSpacingMultiple: 1.5 });
// Deficit
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 0.9, w: 4.6, h: 2.5, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "DEFICIT REPLACEMENT (8h fast)", 5.3, 0.97, 3.5);
s.addText([
{ text: "Deficit = 8 h × 72 mL/hr = 576 mL\n\n", options: { color: C.navyMid, breakLine: true } },
{ text: "1st hour: ", options: { bold: true, color: C.navy } },
{ text: "50% = 288 mL + 72 mL maint.\n", options: { color: C.navyMid, breakLine: true } },
{ text: "2nd hour: ", options: { bold: true, color: C.navy } },
{ text: "25% = 144 mL + 72 mL maint.\n", options: { color: C.navyMid, breakLine: true } },
{ text: "3rd hour: ", options: { bold: true, color: C.navy } },
{ text: "25% = 144 mL + 72 mL maint.", options: { color: C.navyMid } },
], { x: 5.3, y: 1.4, w: 4.2, h: 1.85, fontSize: 10.5, fontFace: "Calibri", lineSpacingMultiple: 1.5 });
// Blood
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 3.55, w: 4.6, h: 1.8, fill: { color: C.navy }, rectRadius: 0.1 });
s.addText("BLOOD LOSS MANAGEMENT", { x: 0.45, y: 3.62, w: 4.2, h: 0.32, fontSize: 11, bold: true, color: C.amber });
s.addText([
...bullets([
"TBV = 70 mL/kg = 2240 mL",
"MABL = TBV × (Hct_start–Hct_min)/Hct_avg",
"Hb 12→ min 8 g/dL = allow ~50 mL/kg",
"Replace crystalloid 3:1 up to MABL",
])
], { x: 0.45, y: 3.98, w: 4.25, h: 1.3, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 3.55, w: 4.6, h: 1.8, fill: { color: C.offWhite }, rectRadius: 0.1 });
s.addText("FLUID CHOICE", { x: 5.35, y: 3.62, w: 4.2, h: 0.32, fontSize: 11, bold: true, color: C.tealDark });
s.addText([
...bulletsTeal([
"Balanced crystalloid: Plasmalyte / Lactated Ringer's",
"Avoid large-volume normal saline (hyperchloraemic acidosis)",
"Colloid if persistent hypotension after crystalloid",
"Glucose-containing solution if hypoglycaemia detected",
])
], { x: 5.35, y: 3.98, w: 4.35, h: 1.3, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
addSlideNumber(s, 17, TOTAL);
}
// ── SLIDE 18: SECTION HEADER — EMERGENCE ────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "SECTION 3\nEmergence & Extubation", "The most critical phase — protecting the graft");
s.addShape(pres.shapes.RECTANGLE, { x: 0.55, y: 1.8, w: 2.5, h: 0.07, fill: { color: C.teal } });
}
// ── SLIDE 19: EMERGENCE & EXTUBATION ─────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Emergence — Smooth is Safe");
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 9.5, h: 0.55, fill: { color: C.red }, rectRadius: 0.06 });
s.addText("⚠ Coughing on ETT raises venous pressure → bleeding → graft displacement | PONV = graft at risk", {
x: 0.4, y: 0.9, w: 9.3, h: 0.55, fontSize: 11, bold: true, color: C.white, valign: "middle",
});
// Deep extubation
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 1.55, w: 4.6, h: 3.8, fill: { color: C.navyMid }, rectRadius: 0.1 });
tealBadge(s, "DEEP EXTUBATION (Preferred)", 0.4, 1.63, 3.8);
s.addText([
...bullets([
"Pre-requisites: fasted, easy airway, haemodynamically stable",
"Turn patient lateral (recovery position) before removing ETT",
"Remove ETT while patient in deep anaesthesia plane",
"Transition to spontaneous ventilation on face mask",
"Maintain airway with jaw thrust + gentle CPAP",
"Move to PACU once SpO₂ >95% breathing spontaneously",
])
], { x: 0.4, y: 2.02, w: 4.25, h: 3.1, fontFace: "Calibri", lineSpacingMultiple: 1.35 });
// Awake extubation
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 5.15, y: 1.55, w: 4.6, h: 3.8, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "AWAKE EXTUBATION (Alternative)", 5.3, 1.63, 3.6);
s.addText([
...bulletsTeal([
"Reverse NMB: neostigmine 50 mcg/kg + glycopyrrolate 10 mcg/kg",
"Wait: TOF ratio >0.9 (quantitative monitoring preferred)",
"Signs: spontaneous breathing, eye opening, purposeful movement",
"Lignocaine 1 mg/kg IV 2 min before extubation (blunt cough reflex)",
"OR: remifentanil 0.01–0.05 mcg/kg/min at emergence (suppresses cough without apnoea)",
"Suction gently before removal",
])
], { x: 5.3, y: 2.02, w: 4.3, h: 3.1, fontFace: "Calibri", lineSpacingMultiple: 1.35 });
addSlideNumber(s, 19, TOTAL);
}
// ── SLIDE 20: VIVA — LARYNGOSPASM ────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.08, h: 5.625, fill: { color: C.red } });
s.addText("VIVA — Emergency Scenario: Post-Extubation", {
x: 0.3, y: 0.18, w: 9, h: 0.42, fontSize: 16, bold: true, color: C.red, charSpacing: 2,
});
s.addText("You performed deep extubation. Child now has stridor. SpO₂ falling. What is your diagnosis and management?", {
x: 0.25, y: 0.72, w: 9.5, h: 0.5, fontSize: 12, bold: true, color: C.amber,
});
// Diagnosis
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 1.3, w: 9.5, h: 0.55, fill: { color: C.navyMid }, rectRadius: 0.08 });
s.addText("Diagnosis: LARYNGOSPASM — inspiratory stridor + paradoxical chest movement + absent air entry on auscultation", {
x: 0.4, y: 1.3, w: 9.3, h: 0.55, fontSize: 10.5, color: C.white, valign: "middle",
});
const steps = [
["1", "Call for Help", "Activate emergency protocol immediately"],
["2", "Jaw thrust + 100% O₂", "CPAP 20–30 cmH₂O via tight-fitting mask — may break incomplete laryngospasm"],
["3", "Larson's manoeuvre", "Firm pressure in notch posterior to mandibular condyle bilaterally"],
["4", "Propofol 0.5–1 mg/kg IV", "Small subanaesthetic dose often breaks laryngospasm without full induction"],
["5", "Succinylcholine 1–2 mg/kg IV", "Complete relaxation if SpO₂ <85% or no response — bag-mask → re-intubate"],
["6", "Atropine if bradycardia", "Suxamethonium + hypoxia → bradycardia in children — 0.02 mg/kg IV"],
];
steps.forEach(([num, action, detail], i) => {
const y = 2.0 + i * 0.57;
s.addShape(pres.shapes.OVAL, { x: 0.28, y: y + 0.06, w: 0.32, h: 0.32, fill: { color: C.red } });
s.addText(num, { x: 0.28, y: y + 0.06, w: 0.32, h: 0.32, fontSize: 10, bold: true, color: C.white, align: "center", valign: "middle" });
s.addText(action + ": ", { x: 0.7, y, w: 2.1, h: 0.32, fontSize: 10.5, bold: true, color: C.amber, valign: "bottom" });
s.addText(detail, { x: 0.7, y: y + 0.3, w: 9.0, h: 0.24, fontSize: 9.5, color: C.grayLight });
});
addSlideNumber(s, 20, TOTAL);
}
// ── SLIDE 21: SECTION HEADER — POSTOPERATIVE ────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "SECTION 4\nPostoperative Management", "Recovery · Analgesia · PONV · Complications");
s.addShape(pres.shapes.RECTANGLE, { x: 0.55, y: 1.8, w: 2.5, h: 0.07, fill: { color: C.teal } });
}
// ── SLIDE 22: POSTOP ANALGESIA ────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Postoperative Analgesia — Multimodal Approach");
const drugs = [
["Paracetamol", "15 mg/kg", "IV/oral", "q6h (max 60 mg/kg/day)", C.teal, "First-line — all cases"],
["Ibuprofen", "10 mg/kg", "Oral", "q8h PRN", C.teal, "Add if no contraindication"],
["Tramadol", "1–2 mg/kg", "IV/oral", "q6h PRN", C.amber, "Moderate pain"],
["Morphine", "0.05–0.1 mg/kg", "IV", "PRN (titrate)", C.amber, "Severe pain — mastoidectomy"],
];
const colWd = [1.8, 1.4, 1.0, 2.0, 1.3, 2.0];
const colXd = [0.25, 2.1, 3.55, 4.6, 6.65, 7.75];
const hdrs = ["Drug", "Dose", "Route", "Frequency", "Tier", "Notes"];
hdrs.forEach((h, ci) => {
s.addShape(pres.shapes.RECTANGLE, { x: colXd[ci], y: 0.9, w: colWd[ci], h: 0.42, fill: { color: C.navy }, line: { color: C.navyMid, width: 0.5 } });
s.addText(h, { x: colXd[ci] + 0.05, y: 0.9, w: colWd[ci] - 0.1, h: 0.42, fontSize: 10, bold: true, color: C.white, valign: "middle" });
});
drugs.forEach((row, ri) => {
const y = 1.32 + ri * 0.62;
const cells = [row[0], row[1], row[2], row[3], "", row[5]];
cells.forEach((cell, ci) => {
const bg = ri % 2 === 0 ? C.white : C.offWhite;
s.addShape(pres.shapes.RECTANGLE, { x: colXd[ci], y, w: colWd[ci], h: 0.62, fill: { color: bg }, line: { color: C.grayLight, width: 0.5 } });
s.addText(cell, { x: colXd[ci] + 0.05, y, w: colWd[ci] - 0.1, h: 0.62, fontSize: 10, color: C.navyMid, valign: "middle" });
});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: colXd[4] + 0.15, y: y + 0.15, w: 0.95, h: 0.3, fill: { color: row[4] }, rectRadius: 0.04 });
s.addText(row[4] === C.teal ? "First Line" : "Second Line", { x: colXd[4] + 0.15, y: y + 0.15, w: 0.95, h: 0.3, fontSize: 8, bold: true, color: C.white, align: "center", valign: "middle" });
});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 3.9, w: 9.5, h: 1.5, fill: { color: C.navyMid }, rectRadius: 0.1 });
s.addText("SCOTT-BROWN'S KEY POINT:", { x: 0.4, y: 3.98, w: 4.0, h: 0.3, fontSize: 10, bold: true, color: C.teal });
s.addText('"Post-operative pain is relatively low and well managed with paracetamol and NSAIDs EXCEPT in the mastoidectomy group — where opioid analgesia is required."', {
x: 0.4, y: 4.3, w: 9.2, h: 0.88, fontSize: 11, color: C.white, italic: true, fontFace: "Calibri",
});
addSlideNumber(s, 22, TOTAL);
}
// ── SLIDE 23: PONV MANAGEMENT ─────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "PONV — Risk, Prophylaxis & Rescue");
// Apfel score
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 0.9, w: 4.3, h: 2.8, fill: { color: C.navyMid }, rectRadius: 0.1 });
tealBadge(s, "APFEL SCORE — THIS PATIENT", 0.4, 0.98, 3.6);
const apfelItems = [
["Female sex", "Male → 0 points"],
["Non-smoker", "12-yr-old → +1"],
["Hx of PONV/motion sickness", "+1 if present"],
["Post-op opioids", "+1 if used"],
["Middle ear surgery", "Independent risk factor +++"],
];
apfelItems.forEach(([factor, score], i) => {
const y = 1.48 + i * 0.48;
s.addText(factor, { x: 0.4, y, w: 2.4, h: 0.26, fontSize: 10, color: C.grayLight, valign: "bottom" });
s.addText(score, { x: 2.85, y, w: 1.55, h: 0.4, fontSize: 9.5, color: score.includes("+") ? C.amber : C.gray, valign: "middle" });
});
// Prophylaxis given
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 4.8, y: 0.9, w: 4.95, h: 2.8, fill: { color: C.offWhite }, rectRadius: 0.1 });
amberBadge(s, "INTRAOPERATIVE PROPHYLAXIS", 4.95, 0.98, 3.8);
const ponvDrugs = [
["Dexamethasone 0.1 mg/kg IV", "At induction", "Anti-inflammatory + antiemetic"],
["Ondansetron 0.1 mg/kg IV", "End of surgery", "5-HT3 antagonist"],
["TIVA (propofol)", "Throughout", "Propofol per se reduces PONV"],
["Avoid N₂O", "Entire case", "N₂O increases PONV independently"],
];
ponvDrugs.forEach(([drug, timing, note], i) => {
const y = 1.48 + i * 0.58;
s.addShape(pres.shapes.RECTANGLE, { x: 4.95, y: y + 0.1, w: 0.05, h: 0.28, fill: { color: C.teal } });
s.addText(drug, { x: 5.12, y, w: 3.0, h: 0.3, fontSize: 10, bold: true, color: C.navy });
s.addText(timing + " | " + note, { x: 5.12, y: y + 0.3, w: 4.5, h: 0.22, fontSize: 9, color: C.gray });
});
// Rescue in PACU
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.25, y: 3.82, w: 9.5, h: 1.6, fill: { color: C.navy }, rectRadius: 0.1 });
s.addText("RESCUE ANTIEMETICS IN PACU (if PONV despite prophylaxis)", {
x: 0.4, y: 3.9, w: 9.2, h: 0.32, fontSize: 11, bold: true, color: C.amber,
});
s.addText([
...bullets([
"Switch antiemetic class: droperidol 0.01 mg/kg IV | metoclopramide 0.15 mg/kg IV | promethazine 0.25 mg/kg IM",
"Ensure adequate hydration and pain control — pain drives PONV",
"Keep lateral position — reduces aspiration risk; inform surgeon (vomiting threatens graft integrity)",
])
], { x: 0.4, y: 4.25, w: 9.2, h: 1.1, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
addSlideNumber(s, 23, TOTAL);
}
// ── SLIDE 24: POSTOP COMPLICATIONS ───────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Postoperative Complications — Monitor & Act");
const comps = [
["Haematoma / Bleeding", C.red,
"Monitor wound dressing hourly. Expanding haematoma or airway compromise → return to OT immediately."],
["Facial Nerve Palsy", C.red,
"Document nerve function BEFORE surgery. Immediate + complete palsy post-op = surgical injury → urgent re-exploration. Delayed partial palsy = oedema → steroids + expectant management."],
["Postoperative Vertigo", C.amber,
"Common after inner ear manipulation. Reassure patient and parents. Monitor ambulation closely — fall risk. Anti-vertigo: betahistine, promethazine."],
["PONV (Nausea/Vomiting)", C.amber,
"See previous slide. Repeated vomiting → graft displacement risk + aspiration. Treat aggressively with rescue antiemetics."],
["CSF Leak / Otorrhoea", C.amber,
"Clear watery discharge post-op. Test for glucose (CSF positive) or beta-2 transferrin. Conservative: head elevation, avoid blowing nose. Persistent → surgical repair."],
["Graft Failure", C.gray,
"Suspected if hearing fails to improve at 6–8 week audiometry. May require revision surgery. Prevent by smooth emergence, avoiding PONV, avoiding N₂O."],
];
comps.forEach(([title, col, detail], i) => {
const y = 0.92 + i * 0.77;
s.addShape(pres.shapes.RECTANGLE, { x: 0.25, y, w: 0.06, h: 0.68, fill: { color: col } });
s.addText(title, { x: 0.4, y: y + 0.02, w: 2.4, h: 0.3, fontSize: 10.5, bold: true, color: C.navyMid });
s.addText(detail, { x: 0.4, y: y + 0.33, w: 9.35, h: 0.38, fontSize: 9.5, color: C.gray, fontFace: "Calibri" });
if (i < comps.length - 1) {
s.addShape(pres.shapes.RECTANGLE, { x: 0.25, y: y + 0.72, w: 9.5, h: 0.01, fill: { color: C.grayLight } });
}
});
addSlideNumber(s, 24, TOTAL);
}
// ── SLIDE 25: MODIFIED ALDRETE SCORE ─────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "PACU Discharge — Modified Aldrete Score");
const rows2 = [
["Parameter", "Score 2", "Score 1", "Score 0"],
["Activity", "Moves all 4 limbs", "Moves 2 limbs", "No movement"],
["Respiration", "Deep breath + cough", "Dyspnoea / limited", "Apnoeic"],
["Circulation", "BP within 20% of pre-op", "BP within 20–50% of pre-op", "BP >50% from pre-op"],
["Consciousness", "Fully awake", "Arousable on calling", "Not responding"],
["SpO₂", ">92% on room air", ">90% with O₂", "<90% with O₂"],
];
const cW = [2.0, 2.5, 2.5, 2.5];
const cX = [0.25, 2.3, 4.85, 7.35];
rows2.forEach((row, ri) => {
const y = 0.92 + ri * 0.7;
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const isCol2 = ci === 1;
const bg = isHeader ? C.navy : (isCol2 ? "#E8F7F4" : C.white);
s.addShape(pres.shapes.RECTANGLE, { x: cX[ci], y, w: cW[ci], h: 0.7, fill: { color: isHeader ? C.navy : (isCol2 ? "D0F0EB" : "FFFFFF") }, line: { color: C.grayLight, width: 0.5 } });
s.addText(cell, {
x: cX[ci] + 0.08, y, w: cW[ci] - 0.16, h: 0.7,
fontSize: isHeader ? 11 : 10, bold: isHeader, color: isHeader ? C.white : (isCol2 ? C.tealDark : C.navyMid), valign: "middle",
});
});
});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y: 5.1, w: 9.5, h: 0.42, fill: { color: C.teal }, rectRadius: 0.05,
});
s.addText("Discharge from PACU when Aldrete Score ≥ 9 | Pain NRS ≤ 3 | No active vomiting | SpO₂ ≥ 95% on room air", {
x: 0.35, y: 5.1, w: 9.3, h: 0.42, fontSize: 10.5, bold: true, color: C.white, valign: "middle",
});
addSlideNumber(s, 25, TOTAL);
}
// ── SLIDE 26: VIVA — POSTOPERATIVE ───────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.08, h: 5.625, fill: { color: C.amber } });
s.addText("VIVA QUESTIONS — Postoperative", {
x: 0.3, y: 0.18, w: 9, h: 0.42, fontSize: 16, bold: true, color: C.amber, charSpacing: 2,
});
vivaBox(s,
"Child is vomiting repeatedly in PACU despite ondansetron. What next?",
"Rule out surgical cause (haematoma, CSF leak) and pain as a PONV driver. Switch antiemetic CLASS — if 5-HT3 has failed use droperidol 0.01 mg/kg IV or metoclopramide 0.15 mg/kg IV. Ensure adequate IV hydration. Keep lateral position (aspiration prevention). Inform surgeon — vomiting threatens graft integrity.",
0.25, 0.75, 9.5, 1.5);
vivaBox(s,
"You notice new-onset complete facial palsy immediately after surgery. What do you do?",
"This is a surgical emergency. Immediate complete palsy = direct facial nerve injury. Inform surgeon immediately. Return to OT for urgent re-exploration. Contrast with delayed partial palsy = post-operative oedema → managed conservatively with steroids and observation. Always document pre-operative baseline nerve function.",
0.25, 2.4, 9.5, 1.65);
vivaBox(s,
"Patient needs to return to OT within 4 hours for haematoma. How do you manage anaesthesia?",
"Treat as FULL STOMACH: impaired gastric motility post-opioids, pain, fear delay emptying. Use RSI: preoxygenate, cricoid pressure, fentanyl + propofol IV + succinylcholine 1–2 mg/kg (or high-dose rocuronium 1.2 mg/kg). Have sugammadex ready. Intubate quickly. Continue TIVA — avoid N₂O (graft still at risk).",
0.25, 4.18, 9.5, 1.3);
addSlideNumber(s, 26, TOTAL);
}
// ── SLIDE 27: THE 5 KEY TAKEAWAYS ────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "5 Key Anaesthetic Takeaways — What the Examiner Expects");
const takeaways = [
["1", "NO Nitrous Oxide", "Middle ear graft = closed space. N₂O diffuses in faster than N₂ escapes → pressure rise → graft displacement. Contraindicated throughout. CSOM obstructs Eustachian tube = no passive venting.", C.red],
["2", "TIVA is the Technique of Choice", "Propofol + remifentanil TIVA: avoids N₂O, ↓PONV vs volatiles, enables controlled hypotension, smooth rapid emergence. Graft is protected by every drug choice.", C.teal],
["3", "Dual PONV Prophylaxis is Mandatory", "Dexamethasone at induction + ondansetron at emergence. Ear surgery is a high-risk independent factor beyond Apfel score. Repeated PONV = graft failure + aspiration.", C.teal],
["4", "Communicate with Surgeon Pre-Induction", "Confirm: NIM facial nerve monitoring in use? If YES — no muscle relaxants post-induction. Plan must be agreed BEFORE first dose of drug is given. This is a team sport.", C.amber],
["5", "Smooth Emergence = Protected Graft", "Coughing on ETT raises venous pressure → bleeding and graft displacement. Deep extubation, lignocaine, or low-dose remifentanil at emergence — every anaesthetist's responsibility.", C.amber],
];
takeaways.forEach(([num, title, detail, col], i) => {
const y = 0.93 + i * 0.9;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.25, y, w: 9.5, h: 0.82, fill: { color: C.white }, rectRadius: 0.06,
line: { color: C.grayLight, width: 0.5 },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.1 },
});
s.addShape(pres.shapes.OVAL, { x: 0.32, y: y + 0.22, w: 0.38, h: 0.38, fill: { color: col } });
s.addText(num, { x: 0.32, y: y + 0.22, w: 0.38, h: 0.38, fontSize: 13, bold: true, color: C.white, align: "center", valign: "middle" });
s.addText(title, { x: 0.85, y: y + 0.04, w: 3.5, h: 0.36, fontSize: 12, bold: true, color: C.navyMid });
s.addText(detail, { x: 0.85, y: y + 0.42, w: 8.75, h: 0.36, fontSize: 9.5, color: C.gray, fontFace: "Calibri" });
});
addSlideNumber(s, 27, TOTAL);
}
// ── SLIDE 28: CLOSING SLIDE ───────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.shapes.OVAL, { x: 6.8, y: -1.0, w: 4.5, h: 4.5, fill: { color: C.navyMid }, line: { color: C.teal, width: 1.5 } });
s.addShape(pres.shapes.OVAL, { x: -1.2, y: 3.5, w: 3, h: 3, fill: { color: C.tealDark } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.15, w: 10, h: 0.475, fill: { color: C.teal } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.1, h: 5.625, fill: { color: C.teal } });
s.addText("PROFESSOR'S CLOSING NOTE", {
x: 0.4, y: 0.65, w: 7, h: 0.4,
fontSize: 12, bold: true, color: C.teal, charSpacing: 3,
});
s.addText('"The moment you anchor your management to patient safety,\nthe examiner knows you are a clinician — not just a student."', {
x: 0.4, y: 1.15, w: 8.5, h: 1.3,
fontSize: 19, color: C.white, italic: true, fontFace: "Calibri Light", lineSpacingMultiple: 1.5,
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.4, y: 2.55, w: 3.5, h: 0.04, fill: { color: C.teal } });
s.addText("Always close your case by saying:", { x: 0.4, y: 2.72, w: 9, h: 0.32, fontSize: 11, color: C.gray });
s.addText('"I would like to re-examine the child in the anaesthetic room immediately before induction to confirm no interval changes, re-check fasting status, and obtain final assent from the child."', {
x: 0.4, y: 3.08, w: 8.8, h: 1.0,
fontSize: 12, color: C.amber, italic: true, fontFace: "Calibri", lineSpacingMultiple: 1.4,
});
s.addText("Anaesthesia for Tympanomastoidectomy | MD Anaesthesia Exam Prep | Department of Anaesthesiology", {
x: 0.3, y: 5.18, w: 9.5, h: 0.38,
fontSize: 10, color: C.white, valign: "middle",
});
}
// ── WRITE FILE ────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/csom-anaesthesia-pptx/CSOM_Anaesthesia_Tympanomastoidectomy.pptx" })
.then(() => console.log("SUCCESS: PPTX written."))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
cd /home/daytona/workspace/csom-anaesthesia-pptx && node generate.js 2>&1
ls -lh /home/daytona/workspace/csom-anaesthesia-pptx/
CSOM Anaesthesia Tympanomastoidectomy
Presentation · PPTX
| # | Slide | Content |
|---|---|---|
| 1 | Title slide | Case overview with bold typographic layout |
| 2 | Learning objectives | 7 numbered objectives with teal icons |
| 3 | Case at a Glance | Patient profile card + 6 anaesthetic flag boxes |
| 4 | Section header | Preoperative Assessment |
| 5 | History | Chief complaints + anaesthetic relevance side-by-side |
| 6 | Airway Assessment | Full table with Mallampati, TMD, ULBT, verdict |
| 7 | Investigations | Table with anaesthetic relevance for each test |
| 8 | NPO & Premedication | ASA 2023 fasting table + premedication chart |
| 9 | VIVA slide | N₂O physiology, NPO timing, MH family history |
| 10 | Section header | Intraoperative Management |
| 11 | Induction | 7-step protocol + ETT selection + why avoid sux |
| 12 | Positioning | 7 positioning points with color-coded bars |
| 13 | Maintenance (TIVA) | Why TIVA, infusion rates, BIS, ventilation targets |
| 14 | Controlled Hypotension | Methods table + MAP target + contraindications |
| 15 | VIVA slide | Epinephrine injection reaction, relaxant mid-surgery, NIM |
| 16 | Monitoring | Full monitoring checklist with color tiers |
| 17 | Fluid Management | Holliday-Segar calculation + MABL + fluid choice |
| 18 | Section header | Emergence & Extubation |
| 19 | Emergence | Deep vs awake extubation side-by-side |
| 20 | VIVA - Emergency | Laryngospasm 6-step ladder on dark red slide |
| 21 | Section header | Postoperative Management |
| 22 | Postop Analgesia | Drug table + Scott-Brown's quote |
| 23 | PONV | Apfel score + dual prophylaxis + rescue antiemetics |
| 24 | Complications | 6 complications with color-coded severity |
| 25 | Aldrete Score | Modified Aldrete table + PACU discharge criteria |
| 26 | VIVA slide | Return PONV, facial palsy, urgent return to OT |
| 27 | 5 Key Takeaways | Card-style numbered summary |
| 28 | Closing | Professor's quote + closing statement to say in exam |
retry
ls -lh /home/daytona/workspace/csom-anaesthesia-pptx/ 2>&1
cd /home/daytona/workspace/csom-anaesthesia-pptx && node generate.js 2>&1
ls -lh /home/daytona/workspace/csom-anaesthesia-pptx/CSOM_Anaesthesia_Tympanomastoidectomy.pptx
CSOM Anaesthesia Tympanomastoidectomy
Presentation · PPTX
bains circuit- act like a professor of anesthesia and explain it to me -include functional analysis ,advantages and disadvantages
THE BAIN CIRCUIT
A Professor's Complete Teaching Session
"Before I explain the Bain circuit, I want you to understand why it was invented. The year was 1972. Drs. Bain and Spoerel were looking at the Mapleson D circuit — a good system for controlled ventilation — and asking: can we make it smaller, lighter, and clinically smarter? What they came up with is an elegant piece of engineering that every anaesthesiologist must understand cold. Not just memorise — understand. Because if you understand it, you can troubleshoot it in the dark at 3 AM."
PART 1: HISTORICAL CONTEXT & CLASSIFICATION
Origin
- Bain JA, Spoerel WE. A streamlined anaesthetic system. Can Anaesth Soc J. 1972;19(4):426-435.
- Bain JA, Spoerel WE. Flow requirements for a modified Mapleson D system during controlled ventilation. Can Anaesth Soc J. 1973;20(5):629-636.
Classification
PART 2: THE MAPLESON CLASSIFICATION — THE ESSENTIAL FOUNDATION
- Fresh gas flow (FGF) inlet
- Adjustable pressure-limiting (APL) valve
- Reservoir bag
| System | FGF inlet position | APL valve position | Best for |
|---|---|---|---|
| A (Magill) | Near reservoir bag | Near patient | Spontaneous ventilation |
| B | Near patient | Near patient | Neither very efficient |
| C | Near patient | Near patient | Neither |
| D | Near patient | Near reservoir bag | Controlled ventilation |
| E | Near patient | No bag, no valve (T-piece) | Paediatric spontaneous |
| F | Near patient | Open-tail bag (Jackson-Rees) | Paediatric both modes |
"The golden rule of Mapleson circuits: where fresh gas is delivered relative to the APL valve determines everything. If FGF is near the patient and the APL valve is away - that is your Mapleson D. Fresh gas pushes exhaled alveolar gas away from the patient and toward the valve. This is efficient for controlled ventilation."
PART 3: ANATOMY OF THE BAIN CIRCUIT
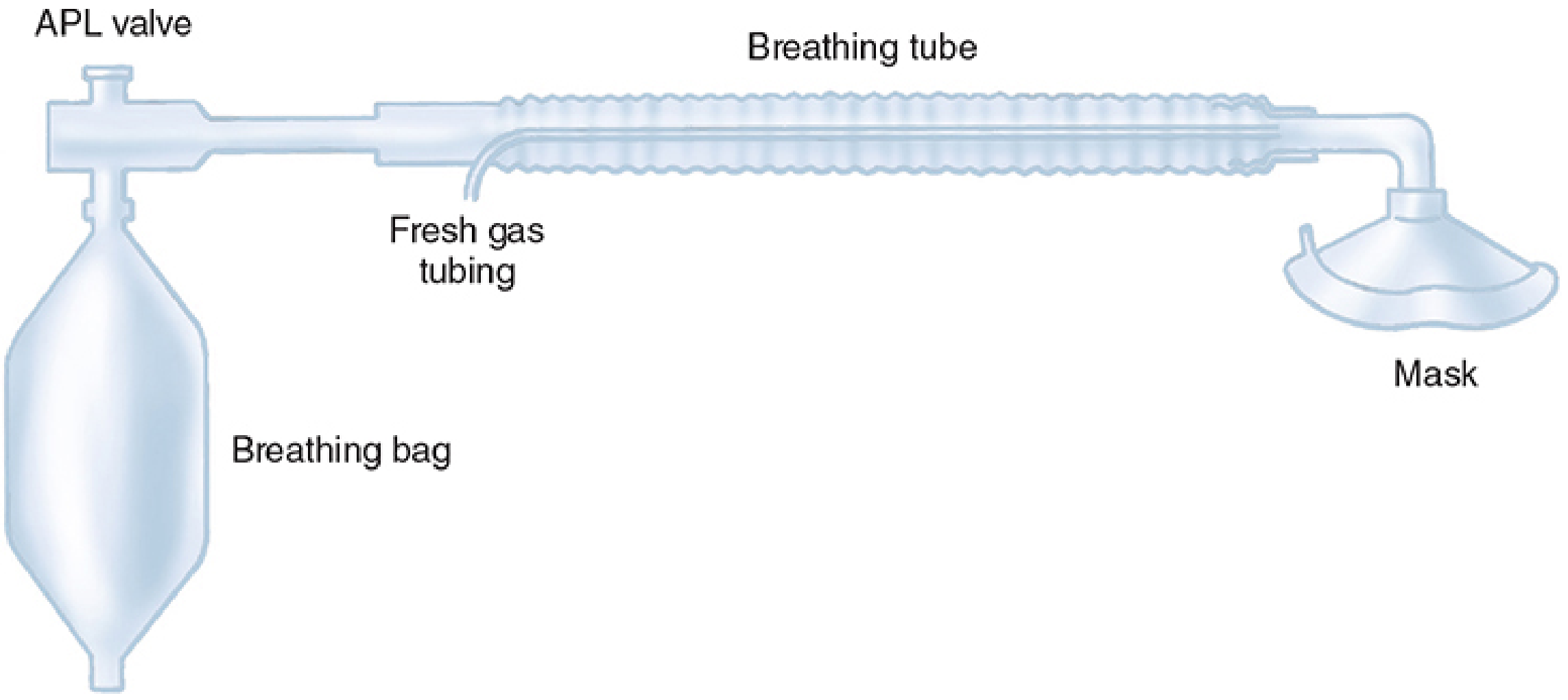
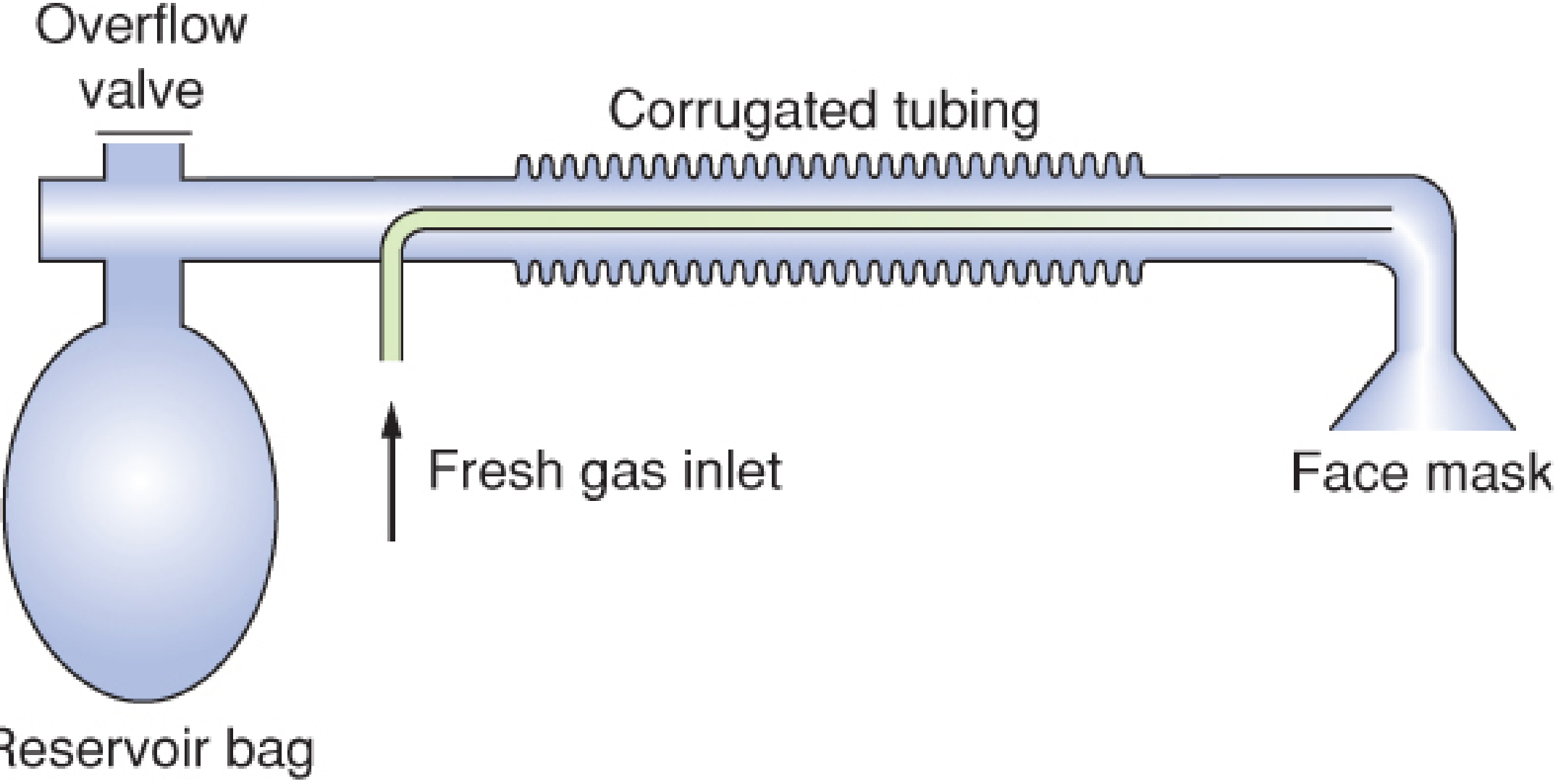
Components (from machine end to patient end):
MACHINE END PATIENT END
│ │
[Reservoir Bag] ── [APL/Pop-off Valve] ── [Outer corrugated tube] ── [Patient]
↑
[Inner narrow tube: FGF inlet]
(enters near bag end, opens at PATIENT end)
| Component | Description | Location |
|---|---|---|
| Outer corrugated tube | The expiratory limb; carries exhaled gas from patient to APL valve | Entire length |
| Inner narrow tube | Carries fresh gas from machine; enters near the reservoir bag end but opens at the patient end | Runs coaxially within outer tube |
| Reservoir bag | Stores gas during expiration for next breath | Machine end |
| APL (pop-off) valve | Vents excess gas to scavenging; adjustable | Machine end (away from patient) |
| FGF inlet | Where O₂/anaesthetic agent enters the circuit from the anaesthesia machine | Machine end physically, but functionally delivers at patient end |
PART 4: FUNCTIONAL ANALYSIS — THE MOST IMPORTANT PART
"This is where students lose marks. They memorise the answer but they can't explain WHY. I want you to be able to draw this and explain gas flow at every phase of the respiratory cycle."
Phase 1: INSPIRATION
- Patient inhales
- Fresh gas from the inner tube flows directly into the patient's airway
- If FGF rate > inspiratory flow rate: pure fresh gas is inspired (no rebreathing)
- If FGF rate < inspiratory flow rate: some gas from the outer tube (exhaled gas) is also drawn in - rebreathing occurs
- Bag is squeezed (or ventilator drives gas)
- Gas in the outer tube (fresh gas + any expired gas mixture) is pushed into the patient
- FGF from inner tube continues simultaneously
Phase 2: EXPIRATION
- Patient exhales - expired gas (CO₂-rich alveolar gas + dead space gas) enters the outer corrugated tube
- Gas travels from patient end toward the machine end (reservoir bag)
- The first portion of exhaled gas is dead space gas (from anatomical dead space - the conducting airways). This gas has NOT undergone gas exchange, so it contains very little CO₂ and retains the inhaled gas mixture.
- The later portion is alveolar gas - CO₂-rich, oxygen-depleted
- Simultaneously, FGF continues flowing through the inner tube toward the patient end, pushing the exhaled gas further toward the APL valve end
- Excess gas exits via the APL valve into the scavenging system
The Key Functional Principle: Flushing Effect
During EXPIRATION:
FGF → [inner tube] → patient end → pushes exhaled gas AWAY from patient
→ exhaled gas travels toward APL valve
→ excess vented via APL valve
During next INSPIRATION:
Gas nearest the patient (at patient end of outer tube) gets inhaled first
= This is the LAST exhaled gas = dead space gas = CO₂ POOR
∴ If FGF is adequate, the CO₂-rich alveolar gas never returns to the patient
PART 5: FRESH GAS FLOW REQUIREMENTS — THE NUMBERS YOU MUST KNOW
"If an examiner gives you one question about the Bain circuit, this will be it. Know these numbers. Know WHY they differ."
| Mode of Ventilation | FGF Required | Why |
|---|---|---|
| Controlled ventilation | 70 mL/kg/min (approximately 1× minute ventilation, or 2.5× MV for safety margin per Barash) | Positive pressure + FGF effectively flushes alveolar gas; efficient CO₂ elimination |
| Spontaneous ventilation | 200–300 mL/kg/min (2.5–3× minute ventilation) | Inspiratory flow demand is variable and fast; less efficient flushing |
- Controlled ventilation: ~70 mL × 70 kg = 4.9 L/min (round to 5 L/min)
- Spontaneous ventilation: ~200-300 mL × 70 kg = 14–21 L/min (very high - expensive and wastes agent)
"This is the Achilles heel of the Bain circuit. For spontaneous breathing in an adult, you need 3× the minute volume. At those flow rates, you are blowing expensive volatile agent out of the pop-off valve. This is why the Bain circuit is not ideal for spontaneous ventilation in adults. It is preferred for controlled ventilation."
PART 6: THE COAXIAL DESIGN — WHY IT MATTERS
Countercurrent Heat Exchange
- Exhaled gas travels in the outer tube from patient → machine end
- Inhaled fresh gas travels in the inner tube from machine → patient end
- These two gas streams travel in opposite directions separated by a thin wall
- Exhaled gas is warm and humid (body temperature, 100% saturated)
- It partially warms and humidifies the incoming cold dry fresh gas
- Result: inspired gas is warmer and more humid than a conventional Mapleson D
- Morgan & Mikhail, 7e: "This modification... retains heat and humidity better than a conventional Mapleson D circuit as a result of partial warming of the inspiratory gas by countercurrent exchange with the warmer expired gases."
- Increased insensible water loss → dehydration
- Mucosal drying → increased airway secretions
- Hypothermia (particularly dangerous in paediatrics)
PART 7: ADVANTAGES OF THE BAIN CIRCUIT
1. Lightweight and compact
- The coaxial design keeps a single tube where a conventional Mapleson D needs two separate limbs (inspiratory + expiratory)
- Less cumbersome during head and neck surgery, ENT, dental procedures
- Particularly convenient when the anaesthesiologist needs to be away from the patient's airway (e.g., remote locations, MRI suites)
2. APL valve positioned away from patient
- In conventional circuits, the pop-off valve is close to the patient's airway - it can get in the surgeon's way during head/neck procedures
- In the Bain circuit, the APL valve is at the machine end (near the reservoir bag), far from the surgical field
- This also facilitates scavenging of waste anaesthetic gases - the scavenging connection is away from the operative field and easy to connect
3. Countercurrent heat and humidity conservation
- Described above - clinical benefit especially in longer cases and paediatric patients
4. Disposable
- Single-use versions available - reduces infection risk
- No cleaning or sterilisation needed between cases
5. Easy to use with spontaneous and controlled ventilation
- Versatile - though FGF requirements differ significantly between the two modes
6. Efficient for controlled ventilation
- At 70 mL/kg/min FGF, provides adequate CO₂ clearance
- The Spoerel flow rate (70 mL/kg/min) has been well validated in clinical studies
7. Low resistance
- No CO₂ absorber, no unidirectional valves (unlike circle system)
- The patient's breathing effort is not fighting against valve resistance
- Particularly advantageous for spontaneously breathing patients with respiratory compromise
8. Useful in remote/field anaesthesia
- Does not require electricity or a complex anaesthesia machine
- Can be used with a draw-over vaporiser in resource-limited settings
PART 8: DISADVANTAGES OF THE BAIN CIRCUIT
1. High FGF requirement for spontaneous ventilation
- 200-300 mL/kg/min is expensive
- Wastes volatile anaesthetic agents
- Causes operating room air pollution if scavenging is inefficient
- Environmental concern (volatile agents have global warming potential)
2. Risk of inner tube kinking or disconnection — The Critical Hazard
"This is the most dangerous and exam-favourite disadvantage. Understand it completely."
- The inner tube is narrow, thin-walled, and runs the full length of the circuit
- It can kink (collapse from external pressure) or disconnect at the machine end
- If this happens:
- Fresh gas no longer reaches the patient end
- Fresh gas instead leaks into the proximal end of the outer tube (near the bag)
- The patient rebreathes exhaled CO₂ from the outer tube
- This causes progressive hypercapnia - and it can be subtle and insidious
- The circuit still looks and feels normal from outside (the outer tube is intact)
- SpO₂ may remain normal for a while (rebreathing does not immediately cause hypoxia if O₂ concentration is adequate)
- The only warning sign may be a rising EtCO₂ on capnography - or in the absence of capnography, nothing until the patient is in severe hypercapnia
- Barash, 9e: "The main hazards related to the use of the Bain circuit are either an unrecognized disconnection or kinking of the inner fresh gas hose. These problems can cause hypercapnia from inadequate gas flow or increased respiratory resistance."
- Morgan & Mikhail, 7e: "Periodic inspection of the inner tubing is mandatory to identify this complication; if unrecognized, either of these mishaps could result in significant rebreathing of exhaled gas."
3. No CO₂ absorption
- Unlike the circle system, there is no soda lime
- CO₂ clearance depends entirely on adequate FGF - if FGF drops, CO₂ accumulates immediately
- No buffer against momentary decreases in gas flow
4. Inefficient use of anaesthetic agents
- High flow rates mean volatile agent is continuously vented through the APL valve
- Cannot use the low-flow or closed-circuit technique (unlike circle system with CO₂ absorber)
- Running cost of volatile agent is substantially higher
5. No rebreathing of humidified gas (compared to circle system)
- Despite countercurrent warming, the heat/humidity conservation is partial, not complete
- Circle system with CO₂ absorber provides better heat and humidity conservation over long cases
6. Outer tube must be transparent
- Miller's 10e: "The outer corrugated tube should be transparent to allow ongoing inspection of the inner tube."
- Opaque circuits cannot be safely used because inner tube integrity cannot be visually confirmed
- A finding frequently missed in hurried setups
PART 9: THE PETHICK TEST — HOW TO TEST BAIN CIRCUIT INTEGRITY
"Every time you pick up a Bain circuit, you must test it. The Pethick test is your safety check. Examiner will ask you this."
Steps:
- Occlude the patient end of the circuit with your thumb
- Flush O₂ at high flow (>30 L/min using the O₂ flush valve) until the reservoir bag is fully distended
- Remove your thumb from the patient end
- Immediately activate the O₂ flush valve again
Interpretation:
| Observation | Interpretation | Mechanism |
|---|---|---|
| Reservoir bag deflates (collapses) | Inner tube INTACT | High-velocity O₂ from the inner tube creates a Venturi effect at the patient end — entrains gas from the outer tube — bag deflates |
| Reservoir bag stays inflated (does not deflate) | Inner tube DAMAGED (kinked or disconnected) | O₂ escapes into the outer tube near the machine end rather than exiting at patient end — no Venturi effect — bag remains full |
"The Venturi effect is the key physical principle. A high-velocity jet of gas at the patient end creates a zone of low pressure around it, which sucks gas out of the outer tube — deflating the bag. If the inner tube is broken, the gas never reaches the patient end, the Venturi effect never occurs, and the bag stays full. This test is recommended as part of the preanesthesia check whenever a Bain circuit is used."
PART 10: COMPARISON TABLE — BAIN vs CIRCLE SYSTEM
| Feature | Bain Circuit (Mapleson D coaxial) | Circle System |
|---|---|---|
| Complexity | Simple | Complex |
| CO₂ elimination | FGF-dependent | CO₂ absorber (soda lime) |
| FGF requirement | High (especially spontaneous) | Low (low-flow possible) |
| Heat & humidity | Partial (countercurrent) | Better (rebreathing of humidified gas) |
| Rebreathing | Absent if adequate FGF | Intentional (CO₂ removed by absorber) |
| Agent wastage | High | Low |
| Resistance | Low | Moderate (valves + absorber) |
| Environmental pollution | Higher | Lower |
| Portability | High | Low (heavy machine dependent) |
| Inner tube hazard | Yes (unique to coaxial design) | No |
| Scavenging ease | Easy (APL at machine end) | Easy |
| Cost per case | Higher (agent waste) | Lower |
| Preferred for | Controlled ventilation, head/neck surgery, short cases, remote anaesthesia | Long cases, paediatrics, low-flow technique |
PART 11: CLINICAL APPLICATIONS — WHERE THE BAIN CIRCUIT SHINES
- Head, neck, and ENT surgery - APL valve away from surgical field; lightweight circuit does not impose torque on the ETT
- Dental anaesthesia - Same reason; access to airway not compromised
- Remote/transport anaesthesia - Simple, lightweight, no CO₂ absorber needed
- Short procedures under controlled ventilation - Efficient and cost-effective for brief cases
- MRI environment - No ferromagnetic components; the simplicity is an advantage
- Resource-limited settings - Requires only gas supply and vaporiser
"Notice that the Bain circuit is predominantly chosen for situations where surgeon-anaesthesiologist proximity at the airway is a concern, and where controlled ventilation is planned. That is the clinical niche. Understand the niche and you will always know when to reach for it."
PART 12: SUMMARY — WHAT THE EXAMINER WANTS TO HEAR
| Question | Answer |
|---|---|
| What is the Bain circuit? | Coaxial modification of Mapleson D system |
| Who described it? | Bain and Spoerel, 1972 |
| What makes it coaxial? | Inner FGF tube runs inside outer expiratory tube |
| Where does FGF exit? | At the patient end (though it enters near the bag) |
| Where is the APL valve? | Machine end (away from patient) |
| FGF for controlled ventilation? | 70 mL/kg/min |
| FGF for spontaneous ventilation? | 200-300 mL/kg/min |
| Most dangerous hazard? | Kinking/disconnection of inner tube → hypercapnia |
| How to detect the hazard? | Pethick test (Venturi principle) |
| Key advantage over conventional Mapleson D? | Countercurrent heat/humidity conservation; compact |
| Key advantage over circle system? | Lightweight, low resistance, no CO₂ absorber |
| Key disadvantage? | High FGF for spontaneous breathing; inner tube risk; agent wastage |
Professor's closing thought: "The Bain circuit is 50 years old and still in widespread use because it solves a real clinical problem elegantly. The coaxial design is engineering genius - one tube inside another, achieving countercurrent heat exchange without adding a single extra component. When you use it, respect its one vulnerability: that inner tube. Check it every single time with the Pethick test before you touch a patient. A disconnected inner tube with no capnography monitoring is how patients die quietly from CO₂ narcosis. The circuit never looks broken from outside. That is what makes it dangerous."
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 3, Breathing Systems
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Chapter 25, The Bain Circuit
- Miller's Anesthesia, 10e - Chapter 20, Mapleson Breathing Systems
- Bain JA, Spoerel WE. Can Anaesth Soc J. 1972;19(4):426-435 (original description)
- Bain JA, Spoerel WE. Can Anaesth Soc J. 1973;20(5):629-636 (FGF requirements)
NEUROMUSCULAR JUNCTION OHYSIOLOGY & MUSCLE RELAXANTS & NEUROMUSCULAR MONITORING - ACT like professor of anaesthesia and explain to a junior resident - with viva questions
NEUROMUSCULAR JUNCTION PHYSIOLOGY, MUSCLE RELAXANTS & NEUROMUSCULAR MONITORING
Professor of Anaesthesia — Teaching Session for Junior Residents
"Sit down. Put your phone away. What I am about to teach you is the foundation of safe anaesthesia practice. Every time you give a muscle relaxant and walk out of the OT without confirming adequate reversal, you are leaving a loaded gun with the patient. Residual paralysis kills people. Quietly. Insidiously. And it is entirely preventable. By the time this session ends, you will understand why — from the molecular level to the bedside."
PART 1: NEUROMUSCULAR JUNCTION PHYSIOLOGY
1.1 Anatomy of the NMJ
MOTOR NERVE TERMINAL
│
[Synaptic Cleft] ← ~50 nm wide
│
MOTOR END PLATE (postjunctional membrane)
The Motor Nerve Terminal (Presynaptic)
- The axon terminal swells into a bouton (terminal knob)
- Contains synaptic vesicles - each vesicle holds approximately 5,000-10,000 molecules of acetylcholine (ACh)
- About 300,000 vesicles are present in an active nerve terminal
- Mitochondria provide ATP for synthesis and storage of ACh
- The presynaptic membrane has voltage-gated calcium channels (VGCCs) - these are the trigger for vesicle release
- Presynaptic membrane also has nicotinic ACh receptors (α₃β₂ subtype) - these modulate ACh release (autoreceptors)
The Synaptic Cleft
- ~50 nm wide
- Contains acetylcholinesterase (AChE) - the enzyme that destroys ACh
- AChE is extraordinarily fast: hydrolyses each ACh molecule in 80-100 microseconds
- There are approximately 10 AChE binding sites for every molecule of ACh released - so most ACh never even reaches the postsynaptic receptor
- Miller's 10e: "Nearly half of the acetylcholine molecules released from the presynaptic nerve membrane are hydrolyzed by acetylcholinesterase before reaching the postsynaptic nAchR."
The Motor End Plate (Postsynaptic)
- The muscle membrane is thrown into junctional folds - this massively increases the surface area
- The nicotinic acetylcholine receptor (nAChR) is concentrated here
- Density: 10,000-30,000 receptors per μm² at the crest of the junctional folds
- AChE is located in the troughs of these folds
1.2 The Nicotinic ACh Receptor (nAChR) — Structure and Function
"This receptor is the most important molecule in NMJ pharmacology. Know its structure cold. Every drug we use acts on it or near it."
Adult (Mature) Receptor
- Pentameric transmembrane glycoprotein
- Composed of five subunits: α₂βδε (two alpha, one beta, one delta, one epsilon)
- Forms an ion channel (ligand-gated) through the centre
- The two α subunits are the ligand-binding sites — BOTH must bind ACh simultaneously for the channel to open
- Miller's 10e: "Each of the two α subunits of the postsynaptic receptors has a ligand (acetylcholine) binding site."
Fetal (Immature) Receptor
- Subunits: α₂βδγ — the ε (epsilon) subunit is replaced by γ (gamma)
- Located extrajunctionally (outside the NMJ) in fetal life and in denervated/burned/immobilised muscle
- Has longer open-channel time and lower conductance than adult receptor
- Clinical significance: upregulated in burns, prolonged immobility, UMN lesions, denervation → succinylcholine causes massive K⁺ release in these conditions
Presynaptic nAChR
- Subunits: α₃β₂ (different from postsynaptic)
- Function: positive feedback — when ACh binds the presynaptic receptor, it stimulates further ACh release (a "mobilisation" mechanism)
- This is why nondepolarising agents that block presynaptic receptors cause FADE on repetitive stimulation — they prevent this mobilisation/positive feedback
How the Channel Works
- ACh binds to both α subunits simultaneously
- Channel opens — allows Na⁺ (and Ca²⁺) to flow IN, K⁺ flows OUT
- Net result: depolarisation of the end plate = end-plate potential (EPP)
- If EPP is large enough, it triggers an action potential along the sarcolemma
- Action potential enters T-tubules → releases Ca²⁺ from SR → excitation-contraction coupling → muscle contraction
1.3 Sequence of Events at the NMJ — Step by Step
"Recite this sequence in your exam. Every step is a potential drug target."
| Step | Event | Drug target? |
|---|---|---|
| 1 | Action potential arrives at motor nerve terminal | Local anaesthetics block axon |
| 2 | Membrane depolarisation opens VGCCs | - |
| 3 | Ca²⁺ influx triggers vesicle fusion with membrane | - |
| 4 | ACh exocytosis into synaptic cleft (~300 vesicles/impulse) | Botulinum toxin blocks this |
| 5 | ACh diffuses across cleft | Partly destroyed by AChE |
| 6 | ACh binds both α subunits of postsynaptic nAChR | NDNMBDs compete here |
| 7 | Ion channel opens → Na⁺ influx → EPP | Succinylcholine activates here |
| 8 | EPP triggers muscle action potential | - |
| 9 | AP propagates via T-tubules → Ca²⁺ release from SR | - |
| 10 | Muscle contraction | - |
| 11 | ACh hydrolysed by AChE → choline reuptaken for resynthesis | Neostigmine inhibits AChE here |
1.4 The Safety Margin of NMJ Transmission
- The normal nerve impulse releases enough ACh to activate 5× more receptors than needed for a maximal EPP
- This safety margin means that a significant fraction of receptors can be blocked without any detectable weakness
- When nondepolarising agents occupy >75-80% of receptors: EPP falls below threshold → muscle contraction fails → clinical paralysis
- When 25-30% of receptors remain available: enough ACh can overcome the block → recovery begins
- This is why single twitch disappears only when 80-90% of receptors are blocked, but TOF fade appears at 70-80% blockade of postsynaptic receptors
PART 2: MUSCLE RELAXANTS — CLASSIFICATION & PHARMACOLOGY
2.1 Classification
NEUROMUSCULAR BLOCKING DRUGS
├── DEPOLARISING
│ └── Succinylcholine (Suxamethonium)
│ - Only clinically available agent
│ - Short-acting (10–15 min)
│
└── NON-DEPOLARISING (NDNMBDs)
├── By CHEMICAL CLASS
│ ├── Benzylisoquinolinium: Atracurium, Cisatracurium, Mivacurium
│ └── Aminosteroid: Rocuronium, Vecuronium, Pancuronium
│
└── By DURATION OF ACTION
├── Short-acting: Mivacurium (~20 min)
├── Intermediate-acting: Rocuronium, Vecuronium, Atracurium, Cisatracurium (~30–60 min)
└── Long-acting: Pancuronium (~60–120 min)
2.2 DEPOLARISING BLOCKADE — SUCCINYLCHOLINE
Structure
- Two acetylcholine molecules joined end-to-end
- The only depolarising agent in clinical use
Mechanism of Action
"Succinylcholine is an ACh mimic that the body cannot destroy fast enough at the NMJ. That is the whole story."
- Binds to both α subunits of nAChR (just like ACh)
- Opens the ion channel → Na⁺ influx → depolarisation → EPP → action potential
- This initial depolarisation causes fasciculations (asynchronous muscle twitching)
- Unlike ACh (destroyed in microseconds by AChE), succinylcholine is NOT a substrate for AChE
- It is metabolised by pseudocholinesterase (plasma butyrylcholinesterase) in plasma — but only after it diffuses AWAY from the NMJ
- The receptor remains persistently depolarised — the membrane is locked in a depolarised state
- A depolarised membrane cannot respond to subsequent ACh release → neuromuscular blockade
- This is called Phase I (depolarising) block
Pharmacokinetics
- Onset: Maximum block within 60 seconds (fastest of all NMBDs)
- Duration: ~10–15 minutes at 1 mg/kg (DUR25% = 10–12 min)
- ED95: 0.3 mg/kg; intubating dose: 1–1.5 mg/kg (3–5× ED95)
- Metabolism: Pseudocholinesterase in plasma → succinylmonocholine → succinic acid + choline
- Only ~10% of administered dose ever reaches the NMJ — the rest is destroyed in plasma
- Barash 9e: "The very short duration of succinylcholine is primarily due to its rapid hydrolysis by pseudocholinesterase... only a small fraction, approximately 10%, of the original intravenous dose reaches the neuromuscular junction."
Characteristics of Phase I Block (on nerve stimulator)
| Feature | Phase I (Depolarising) Block |
|---|---|
| Train-of-four (TOF) | No fade — all 4 twitches equal in height |
| Tetanic stimulation | No fade — sustained tetanus |
| Post-tetanic potentiation (PTP) | Absent |
| Anticholinesterase effect | Potentiates block (worsens it) |
| Fasciculations | Present before onset |
| Preceding NDNMBDs | Antagonises block |
Phase II Block (Dual Block)
"This trips up every resident. Phase II block is what happens when you give too much succinylcholine."
- Occurs after large single dose (≥10× ED95), repeated doses, or prolonged infusion
- The receptor undergoes receptor desensitisation — it enters a refractory state despite persistent occupancy by succinylcholine
- The membrane repolarises but the receptor is now unresponsive
- Block characteristics change and begin to resemble nondepolarising block
| Feature | Phase II Block |
|---|---|
| TOF | Fade appears |
| Tetanic stimulation | Fade appears |
| Post-tetanic potentiation | Present |
| Anticholinesterase | May partially reverse it |
| When it occurs | After prolonged/large dose sux infusion |
Side Effects of Succinylcholine — The Examiner's Favourite Topic
| Side Effect | Mechanism | Clinical Relevance |
|---|---|---|
| Fasciculations | Asynchronous muscle depolarisation | 80-90% of patients; muscle damage, myoglobinuria; pretreat with small dose NDNMBD |
| Myalgias | Fasciculation-related muscle injury | 50-60% of patients; postoperative pain (1-2 days) |
| Hyperkalaemia | K⁺ exits muscle during depolarisation; normal rise +0.5 mEq/L | Dangerous (cardiac arrest) in: burns, crush injuries, prolonged immobility, UMN/LMN lesions, denervation, severe sepsis, rhabdomyolysis — due to upregulated extrajunctional (fetal-type) receptors |
| Bradycardia / Asystole | Muscarinic stimulation; greater risk in children and with repeat doses | Pretreat with atropine in children |
| Increased IOP | Extraocular muscle contraction | Relative contraindication in open globe injury (though evidence debated) |
| Increased intragastric pressure | Fasciculations of abdominal muscles | Usually matched by increased LOS pressure |
| Increased ICP | Mechanism unclear; possibly related to cerebral blood flow | Use with caution in raised ICP |
| Masseter spasm | Succinylcholine-induced jaw rigidity | Early sign of MH; if isolated → can proceed cautiously; if generalised → MH protocol |
| Malignant hyperthermia | Pharmacogenetic trigger — ryanodine receptor mutation | Potentially fatal; treat with dantrolene |
| Prolonged apnoea | Pseudocholinesterase deficiency (qualitative or quantitative) | See dibucaine number |
Pseudocholinesterase Deficiency & Dibucaine Number
| Genotype | Dibucaine Number | Duration of Block |
|---|---|---|
| Normal (EuEu) | 70-80% | ~10-15 min |
| Heterozygous atypical (EuEa) | 40-60% | ~30 min |
| Homozygous atypical (EaEa) | <20% | 2-8 hours |
"Dibucaine is a local anaesthetic that inhibits normal pseudocholinesterase by ~80% but inhibits atypical enzyme by only ~20%. So a LOW dibucaine number means ATYPICAL enzyme means PROLONGED succinylcholine action. Low number = bad news. Remember: Low = problem."
Contraindications to Succinylcholine (Absolute)
- Personal or family history of malignant hyperthermia
- Burns (>24 hours post-burn)
- Crush injuries / rhabdomyolysis
- Denervation injuries (spinal cord injury, stroke, Guillain-Barré)
- Prolonged immobility (ICU patients >48-72 hours)
- Hyperkalaemia (K⁺ >5.5 mEq/L)
- Known pseudocholinesterase deficiency
- Myopathies / muscular dystrophies (especially Duchenne's — risk of rhabdomyolysis, hyperkalaemia, cardiac arrest)
- Open globe injury (relative — controversial)
2.3 NON-DEPOLARISING NEUROMUSCULAR BLOCKING DRUGS (NDNMBDs)
Mechanism of Action
- Bind to one or both α subunits of the nAChR competitively — without activating the receptor
- No channel opening — no depolarisation
- When enough receptors are occupied: EPP falls below threshold → no muscle contraction
- Barash 9e: "Nondepolarizing neuromuscular blocking drugs bind to one or both alpha subunits of the nicotinic acetylcholine receptor without causing any activation of these ion receptor channels."
- Block the α₃β₂ presynaptic autoreceptors
- Normal function of these receptors: ACh released → binds presynaptic receptor → promotes mobilisation and further release of ACh (positive feedback)
- When blocked: reduced ACh mobilisation during repeated stimulation → ACh stores become depleted → FADE on TOF and tetanic stimulation
- Miller's 10e: "Fade in response to tetanic and train-of-four stimuli results mainly from block of presynaptic nicotinic receptors."
Key Pharmacological Concepts
- Dose required for 95% twitch depression at the adductor pollicis
- Succinylcholine: 0.3 mg/kg
- Rocuronium: 0.3 mg/kg
- Vecuronium: 0.05 mg/kg
- Cisatracurium: 0.05 mg/kg
"This is a beautiful piece of pharmacology. The less potent the drug, the more molecules you have to give to achieve effect. More molecules at the NMJ = faster onset. This is why rocuronium (low potency) has fast onset, and cisatracurium (high potency, few molecules) has slow onset."
- Miller's 10e: "The speed of onset is inversely proportional to the potency of nondepolarizing neuromuscular blocking drugs... Rocuronium has a molar potency that is approximately 13% that of vecuronium. Its onset of effect is more rapid."
- Clinically: intubating conditions develop before the adductor pollicis is fully blocked
- Monitoring site (adductor pollicis) overestimates blockade of larynx/diaphragm
- Recovery at the adductor pollicis occurs AFTER recovery at central muscles
Individual NDNMBDs — Drug Profiles
ROCURONIUM
| Feature | Value |
|---|---|
| Class | Aminosteroid |
| Duration | Intermediate (30–60 min) |
| ED95 | 0.3 mg/kg |
| Intubating dose | 0.6 mg/kg (2× ED95) |
| RSI dose | 1.2 mg/kg (4× ED95) — approaches succinylcholine onset speed |
| Onset at 0.6 mg/kg | ~2–3 min |
| Onset at 1.2 mg/kg | ~60 seconds |
| Elimination | Hepatobiliary (>75%), renal (10-25%) |
| Reversible by | Neostigmine (moderate block) or Sugammadex (any depth) |
| Unique features | Fastest onset of all NDNMBDs at high dose; preferred alternative to suxamethonium with sugammadex as backup |
VECURONIUM
| Feature | Value |
|---|---|
| Class | Aminosteroid (monoquaternary) |
| Duration | Intermediate (25–40 min) |
| ED95 | 0.05 mg/kg |
| Intubating dose | 0.1 mg/kg |
| Elimination | Hepatobiliary, renal |
| Unique features | Minimal cardiovascular effects; active metabolite (3-OH vecuronium) accumulates in renal failure |
ATRACURIUM
| Feature | Value |
|---|---|
| Class | Benzylisoquinolinium |
| Duration | Intermediate (25–40 min) |
| ED95 | 0.2 mg/kg |
| Intubating dose | 0.5 mg/kg |
| Elimination | Hofmann elimination + ester hydrolysis (organ-independent) |
| Active metabolite | Laudanosine — CNS stimulant; seizures at very high concentrations |
| Histamine release | Yes, with rapid injection at high doses |
| Unique features | Safe in renal AND hepatic failure — gold standard for organ failure patients |
CISATRACURIUM
| Feature | Value |
|---|---|
| Class | Benzylisoquinolinium (isomer of atracurium) |
| Duration | Intermediate (40–60 min) |
| ED95 | 0.05 mg/kg |
| Intubating dose | 0.1–0.15 mg/kg |
| Elimination | Hofmann elimination (slower than atracurium) |
| Histamine release | Minimal to none |
| Unique features | Preferred in critically ill patients — no histamine, less laudanosine; safe in organ failure |
PANCURONIUM
| Feature | Value |
|---|---|
| Class | Aminosteroid (bisquaternary) |
| Duration | Long (60–120 min) |
| Elimination | Renal (70%), hepatic (30%) |
| CVS effects | Tachycardia and hypertension (vagolytic + sympathomimetic) |
| Unique features | Cheap; still used in low-resource settings; avoid in renal failure, cardiac disease |
MIVACURIUM
| Feature | Value |
|---|---|
| Class | Benzylisoquinolinium |
| Duration | Short (15–20 min) |
| Elimination | Pseudocholinesterase (like succinylcholine) |
| Unique features | Shortest-acting NDNMBD; histamine release; prolonged in pseudocholinesterase deficiency |
Characteristics of Non-Depolarising Block (nerve stimulator)
| Feature | Non-Depolarising Block |
|---|---|
| TOF | Fade — T4 < T3 < T2 < T1 (progressively smaller) |
| Tetanic stimulation | Fade — sustained tetanus not maintained |
| Post-tetanic potentiation | Present — twitches stronger after tetanus |
| Anticholinesterase | Reverses block |
| Fasciculations | Absent |
| Prior NDNMBDs | Potentiate each other |
PART 3: REVERSAL OF NEUROMUSCULAR BLOCKADE
3.1 Anticholinesterases (Neostigmine-based reversal)
Mechanism
- Inhibit acetylcholinesterase (AChE) at the NMJ
- Result: ACh accumulates in the synapse → higher [ACh] → outcompetes the NDNMBD for α subunit binding sites
- The reversal is competitive — it works by shifting the equilibrium, not by destroying the blocker
- Miller's 10e: "If larger concentrations of acetylcholine are present at the neuromuscular junction, acetylcholine will be more likely to attach to the postsynaptic receptor."
The Ceiling Effect — Critical Concept
- Neostigmine has a ceiling effect — once AChE is maximally inhibited (~100%), giving more neostigmine provides NO additional reversal
- Maximum effective dose: ~50-70 mcg/kg (doses >70 mcg/kg provide no benefit and add side effects)
- If the block is too deep when neostigmine is given, there is simply not enough ACh to overcome the competition → inadequate reversal
- Miller's 10e: "Maximal effective doses of neostigmine have not been clearly defined, but may have been overestimated, and there is currently insufficient evidence to support the contention that doses higher than 50 mcg/kg provide additional benefit."
Neostigmine Dosing
| Depth of Block (TOF count/ratio) | Neostigmine Dose | Expected reversal time |
|---|---|---|
| TOF ratio 0.5–0.9 | 20–40 mcg/kg | 5–10 min |
| TOF count 3–4 (ratio <0.5) | 40–60 mcg/kg | 10–20 min (uncertain) |
| TOF count 0–2 / PTC 1–5 | Do NOT use neostigmine | Use sugammadex instead |
Muscarinic Side Effects of Neostigmine
- Because AChE is inhibited everywhere (not just at NMJ), muscarinic receptors are also activated
- Must ALWAYS be combined with an anticholinergic agent to block muscarinic effects:
- Glycopyrrolate 10 mcg/kg (preferred — does not cross BBB, less tachycardia)
- Atropine 20 mcg/kg (causes tachycardia)
- Muscarinic effects: bradycardia, bronchospasm, increased secretions, bowel peristalsis
3.2 Sugammadex — The Revolution in Reversal
"Sugammadex is one of the most clinically important drugs introduced in anaesthesia in the last two decades. It changed how we practice. Understand it mechanistically, not just as 'the reversal drug for rocuronium'."
What is Sugammadex?
- A modified γ-cyclodextrin — a ring-shaped sugar molecule with a hydrophobic (lipophobic) core and hydrophilic exterior
- It was specifically engineered to encapsulate aminosteroid NMBDs (rocuronium and vecuronium)
- Structure: 8 sugar units arranged in a donut shape with extended side chains that are negatively charged (electrostatic attraction to the quaternary ammonium groups of rocuronium)
Mechanism — Chemical Encapsulation
"This is completely different from neostigmine. Neostigmine works at the NMJ. Sugammadex never goes near the NMJ."
- Sugammadex administered IV → enters plasma
- Its hydrophobic core physically encapsulates rocuronium/vecuronium molecules in plasma — like a molecular cage capturing a molecule
- Plasma-free rocuronium concentration falls rapidly
- This creates a concentration gradient: high free rocuronium at NMJ (effect compartment) → low free rocuronium in plasma
- Rocuronium diffuses away from NMJ into plasma → gets encapsulated by more sugammadex
- NMJ is rapidly cleared of rocuronium → nAChR available again → neuromuscular transmission restored
- The rocuronium-sugammadex complex is excreted renally (intact)
- Miller's 10e: "Free rocuronium molecules rapidly diffuse towards the plasma compartment and are encapsulated by sugammadex. Thus, the increase in plasma levels of rocuronium after sugammadex administration illustrates the mechanism responsible for the rapid reversal of neuromuscular block by sugammadex."
Advantages over Neostigmine
| Feature | Neostigmine | Sugammadex |
|---|---|---|
| Mechanism | Enzyme inhibition (ACh accumulation) | Direct encapsulation (physically removes rocuronium) |
| Works at deep block? | No — ceiling effect | Yes — reverses any depth including profound block |
| Muscarinic side effects | Yes (bradycardia, bronchospasm) | None |
| Need for anticholinergic? | Yes (glycopyrrolate/atropine mandatory) | No |
| Reversal of benzylisoquinoliniums? | Yes (atracurium, cisatracurium) | No — only aminosteroids |
| Time to full reversal (moderate block) | ~10–15 min | ~2–3 min |
| Time to full reversal (profound block) | Cannot reliably reverse | ~3–5 min at 4 mg/kg |
| Residual blockade risk | Higher | Much lower (with correct dosing) |
Sugammadex Dosing
| Depth of Block | TOF Monitoring Finding | Dose |
|---|---|---|
| Moderate block | TOF count ≥2 (TOF ratio returning) | 2 mg/kg |
| Deep block | TOF count 0, PTC 1–2 | 4 mg/kg |
| Immediate reversal after rocuronium (e.g., can't intubate can't oxygenate) | Within 3 min of rocuronium 1.2 mg/kg | 16 mg/kg |
Underdosing — The Dangerous Mistake
- Doses <1 mg/kg at deep block → recurrence of paralysis (redistribution of rocuronium from peripheral compartments overwhelms available sugammadex)
- Miller's 10e: "Underdosing of sugammadex is associated with an increased risk of residual neuromuscular block or recurrence of neuromuscular block."
- Always dose by depth of block, confirmed by quantitative monitoring
PART 4: NEUROMUSCULAR MONITORING
"This is where residents fail their patients most often. They give the drug, they reverse, they extubate — and they rely on subjective clinical signs. That is wrong. That has been proven wrong by decades of research. You must use objective monitoring."
4.1 Why Monitor?
- Defined as TOF ratio <0.9 at the adductor pollicis
- Occurs in 30-65% of patients after intermediate-acting NMBDs reversed with neostigmine (based on studies cited in Barash)
- Consequences of RNMB:
- Decreased upper oesophageal sphincter tone → aspiration risk
- Impaired coordination of swallowing musculature
- Decreased hypoxic ventilatory response — patient does not respond to hypoxia normally
- Atelectasis, hypoventilation, airway obstruction
- Increased hospital length of stay, morbidity, mortality
4.2 Types of Nerve Stimulation Patterns
1. Single Twitch (ST)
- A single supramaximal stimulus (0.1 Hz)
- Records baseline twitch height, then compares during and after block
- 80-90% receptor occupancy needed before twitch is depressed
- Not sensitive enough to detect mild/residual block
2. Train-of-Four (TOF) — The Gold Standard
- Four stimuli at 2 Hz (0.5 seconds apart)
- Responses labelled T1, T2, T3, T4
- TOF ratio = T4/T1 (height of 4th twitch divided by 1st)
- In the absence of any block: all 4 twitches equal, TOF ratio = 1.0
- With nondepolarising block: fade appears (presynaptic ACh depletion)
| TOF count | Approximate receptor blockade | Clinical significance |
|---|---|---|
| 4 twitches with no fade (ratio >0.9) | <75% blockade | Adequate recovery — extubation criteria met |
| 4 twitches with fade (ratio 0.3–0.9) | 75–85% blockade | Partial recovery — inadequate for extubation |
| 3 twitches | ~85% blockade | Partial block |
| 2 twitches | ~90% blockade | Deep partial block |
| 1 twitch | ~95% blockade | Near-profound |
| 0 twitches (TOF count 0) | >95% blockade | Profound block — neostigmine INEFFECTIVE |
"Write this down: TOF ratio < 0.9 = residual paralysis. Not 0.7. Not 0.8. The target is 0.9 confirmed by quantitative (objective) monitoring. This is the standard of care."
3. Tetanic Stimulation
- 50 Hz or 100 Hz for 5 seconds
- Normal response: sustained contraction (no fade)
- With nondepolarising block: fade (progressive decrease in tension)
- Very painful — only used in anaesthetised patients
4. Post-Tetanic Count (PTC)
- Used during profound block when TOF count = 0
- Apply 50 Hz tetanus for 5 seconds, then after 3 seconds deliver single twitches at 1 Hz
- Count how many single twitches are detectable
- PTC 1-2 → very deep block; only sugammadex 4 mg/kg is appropriate
- PTC 10-15 → approaching moderate block; reversal with neostigmine may become feasible
- Used to predict when clinical recovery will begin
5. Double-Burst Stimulation (DBS)
- Two short bursts of 50 Hz separated by 750 ms
- Normal: both bursts equal
- With residual block: fade (second burst weaker than first)
- More sensitive than TOF for detecting residual block by tactile assessment — the fade is more easily felt by hand than 4 twitches
4.3 Subjective vs Objective Monitoring — The Critical Distinction
| Method | How it works | Reliability |
|---|---|---|
| Subjective (qualitative) | You FEEL or SEE the response to TOF stimulation | Unreliable for TOF ratio <0.4 — studies show clinicians cannot reliably detect fade until TOF ratio <0.4 |
| Objective (quantitative) | Acceleromyography (AMG) or EMG measures ACTUAL ratio | Accurately detects TOF ratio at all levels including 0.7-0.9 |
Types of Objective Monitors
- Acceleromyography (AMG) — measures acceleration of thumb with piezoelectric sensor; most common bedside device (TOF-Watch)
- Electromyography (EMG) — measures electrical activity of muscle; most accurate
- Mechanomyography (MMG) — measures force of thumb contraction against transducer; research gold standard
4.4 Monitoring Site
- Standard: Adductor pollicis (stimulate ulnar nerve at wrist)
- Reflects peripheral block — recovers AFTER central muscles (larynx, diaphragm)
- Therefore it is the most conservative site — if adductor pollicis shows full recovery, central muscles have definitely recovered
- Alternative sites: orbicularis oculi (face), flexor hallucis brevis (foot in paediatrics)
4.5 Clinical Signs of Adequate Reversal — And Why They Are Unreliable
"Residents still use these clinical signs. I want you to understand them — but also understand their limitations."
| Clinical Sign | What it tests | TOF ratio at which reliable |
|---|---|---|
| Head lift ≥5 seconds | Neck flexors | Unreliable below TOF ratio 0.5 |
| Hand grip sustained | Forearm muscles | Unreliable below TOF ratio 0.6 |
| Eye opening | Orbicularis oculi | Relatively sensitive |
| Tongue depressor test | Can patient resist removal of tongue depressor? | Useful but subjective |
| SpO₂ >95% | Peripheral oxygenation | Cannot detect subtle hypoventilation |
PART 5: VIVA QUESTIONS — HIGH YIELD
- Pseudocholinesterase deficiency (most likely) — quantitative (low enzyme levels) or qualitative (atypical enzyme — dibucaine number <30)
- Phase II block — though unlikely at 1.5 mg/kg without repeat doses
- Hypothermia — reduces enzyme activity
- Severe liver disease — liver synthesises pseudocholinesterase
- Pregnancy, oral contraceptives, echothiophate eye drops — reduce pseudocholinesterase
- Myasthenic crisis (rare — underlying disease unmasks)
Professor's Summary: "Three things I want you to take from this session: One — the NMJ is not a simple on/off switch. It is a complex pharmacological target with presynaptic and postsynaptic mechanisms, a safety margin, and drug targets at every step. Two — there are two fundamentally different types of blockade: depolarising (sux) and non-depolarising, with completely different pharmacology and completely different reversal strategies. Mix them up in the exam — or in the OT — and you will cause harm. Three — residual paralysis is a real, proven, common, and deadly complication of NMBDs. The only way to rule it out is quantitative TOF monitoring. TOF ratio ≥0.9, confirmed objectively, before every extubation. That is the standard. That is what I expect from you."
- Miller's Anesthesia, 10e — Chapter 24: Neuromuscular Blocking Agents (extensive use)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e — Chapter 21: Neuromuscular Blocking Drugs
- Morgan & Mikhail's Clinical Anesthesiology, 7e — Chapter on NMBDs
- Katzung's Basic and Clinical Pharmacology, 16e — Neuromuscular Pharmacology
PDPH - COMPREHENSIVE REVIEW - ACT LIKE PROFESSOR OF ANAESTHESIA AND EXPLAIN TO JUNIOR RESIDENT - INCLUDE Q&A WITH VIVA QUESTIONS FOR MD FINAL EXAM
POST-DURAL PUNCTURE HEADACHE (PDPH)
Comprehensive Review — Professor of Anaesthesia Teaching Session
For Junior Residents — MD Final Exam Level
"Before we start, let me tell you why PDPH matters beyond being just a headache. A 25-year-old woman who just delivered her baby is now bedridden with a splitting headache, unable to feed her infant, crying in pain. It happened because of something we did. Or something we can prevent. Or something we failed to treat correctly. PDPH is not a minor inconvenience — it has been associated with cerebral venous thrombosis, subdural haematoma, and long-term neurological sequelae. Know it completely. Know it comprehensively."
PART 1: DEFINITION AND HISTORICAL CONTEXT
PART 2: INCIDENCE
| Clinical Scenario | Incidence of PDPH |
|---|---|
| Spinal anaesthesia, 25G pencil-point needle | <1–2% |
| Spinal anaesthesia, 22G Quincke (cutting) needle | 2–5% |
| Spinal anaesthesia, 16–18G needle | >70% |
| Accidental dural puncture (ADP) with 18G Tuohy needle | 50–80% |
| Diagnostic lumbar puncture (LP), 20G cutting needle | 10–30% |
| Myelography | Variable (similar to LP) |
-
90% of PDPH cases begin within 3 days of procedure
- 66% begin within the first 48 hours
- 72% resolve spontaneously within 7 days
- 87% resolve by 6 months
- A small percentage become chronic (>6 months) — increasingly recognised as causing long-term neurological and psychological sequelae
PART 3: PATHOPHYSIOLOGY — THE TWO THEORIES
"Examiners love to ask this. Know BOTH theories. Know which one is currently favoured. And know the clinical sign that supports each theory."
Theory 1: CSF Hypovolemia → Traction on Pain-Sensitive Intracranial Structures
- Dural puncture → dural defect (hole) → CSF leaks from intrathecal space into epidural space
- CSF leak rate exceeds CSF production rate (~450 mL/day = ~0.3 mL/min)
- Intracranial CSF volume decreases → intracranial hypotension
- The brain is normally cushioned and suspended in CSF (Archimedes' principle — the 1400g brain effectively weighs only ~50g in CSF)
- With CSF loss, the brain sags downward under gravity
- Traction on pain-sensitive intracranial structures: dura, meninges, tentorium cerebelli, bridging veins, cranial nerves
- This traction is WORSE in the upright position (gravity pulls the brain further down) → postural component
- Relieved when supine → gravity effect eliminated → headache resolves
- The postural nature of the headache
- The onset delay (takes time for CSF to leak and pressure to drop)
- Cranial nerve palsies (traction on VI — abducens, causing diplopia; VIII — auditory/vestibular, causing tinnitus/hearing changes)
- Subdural haematoma — the bridging veins are stretched, they tear → bleeding
Theory 2: Compensatory Cerebral Vasodilation
- CSF loss → ↓intracranial pressure (ICP)
- Monroe-Kellie doctrine: Volume of brain + CSF + blood = constant
- ↓CSF volume → compensatory ↑cerebral blood volume → cerebral vasodilation
- Vasodilation of meningeal/intracranial vessels → vascular headache (similar to migraine mechanism)
- Vasodilation is worse upright (orthostatic) → postural headache
- Why caffeine helps (vasoconstrictor → reduces vasodilation)
- Why triptans may help (anti-migraine vasoconstrictors)
- The throbbing character of some PDPH (vascular pulsation)
PART 4: CLINICAL FEATURES
4.1 Classical Presentation
"The examiner gives you a patient. You must be able to DIAGNOSE PDPH and differentiate it from other post-neuraxial headaches. The postural component is the cardinal feature."
- Location: Frontal (most common), occipital, or fronto-occipital; extends to the neck; can be retro-orbital
- Character: Dull, throbbing, or pressure-like; may be constant or intermittent
- Postural hallmark: Worsens within 30 seconds of sitting/standing; improves within 30 seconds of lying flat
- Severity: Mild to completely debilitating
- Onset: Usually 12-72 hours after procedure; occasionally immediate
| Symptom | Mechanism | Frequency |
|---|---|---|
| Nausea and vomiting | Meningeal irritation / vagal | Common |
| Neck stiffness/pain | Meningeal traction | Common |
| Photophobia | Meningeal irritation | Common |
| Tinnitus, hearing changes | CN VIII traction | Less common |
| Diplopia | CN VI (abducens) traction — most common cranial nerve palsy | ~1-2% of PDPH |
| Dizziness/vertigo | CN VIII involvement | Present |
| Visual changes | CN II or III involvement (rare) | Rare |
| Cortical blindness | Severe cerebral vasodilation | Very rare |
| Seizures | Severe intracranial hypotension | Very rare |
4.2 Serious Complications — What You Must Not Miss
- Cerebral venous thrombosis AND subdural haematoma (composite adjusted OR = 19.0; 95% CI 11.2–32.1)
- Bacterial meningitis (adjusted OR = 39.7; 95% CI 13.6–115.1)
"Write that down. A patient with PDPH has a 19-times higher risk of CVT or subdural haematoma. This is not a benign headache. If a patient with PDPH develops a headache that is no longer postural — that persists when lying down, or is associated with fever, neck stiffness, or focal neurological signs — that is an emergency. Immediate imaging and neurosurgical review."
Red Flags — When to Investigate Urgently
| Red Flag | Think of |
|---|---|
| Headache no longer postural (now constant) | Subdural haematoma / CVT |
| Fever + neck stiffness | Bacterial meningitis |
| Focal neurological deficits | CVT / intracranial haematoma |
| Sudden severe "thunderclap" headache | Subarachnoid haemorrhage |
| Headache worsening despite blood patch | Subdural haematoma |
| Seizures | CVT / severe intracranial hypotension |
PART 5: RISK FACTORS
5.1 Non-Modifiable Risk Factors
| Factor | Relative Risk / Comment |
|---|---|
| Young age (18-30 yrs) | Higher risk vs elderly; elderly have lower intracranial pressure |
| Female sex | 2-3× higher risk than males |
| Pregnancy | Highest risk group — combination of age, sex, and post-delivery epidural pressure changes |
| Low BMI | Less epidural fat → more CSF drainage |
| History of PDPH | Prior occurrence increases future risk |
| Chronic headache disorders | Pre-existing headache predisposes |
| Anxiety | Possibly — lower pain threshold |
5.2 Modifiable Risk Factors (Operator-Controlled)
| Factor | Effect | Recommendation |
|---|---|---|
| Needle gauge | Larger gauge = larger hole = more CSF leak = more PDPH | Use smallest gauge appropriate |
| Needle tip design | Cutting (Quincke) > Pencil-point (Whitacre, Sprotte) | Use pencil-point whenever possible |
| Needle bevel orientation | Bevel perpendicular to dural fibres = cuts fibres = more CSF leak | Orient bevel PARALLEL to long axis of spine |
| Number of dural puncture attempts | More attempts = more holes | Skilled technique, ultrasound guidance |
| Stylet replacement before needle withdrawal | Leaving stylet out on withdrawal may carry arachnoid out, worsening defect | Replace stylet before withdrawing needle |
5.3 Needle Types — The Examiner's Favourite
Cutting Needles (Quincke type):
- Standard bevel at 45° angle
- Cut through dural fibres
- Larger dural defect persists → more CSF leak
Pencil-Point Needles (Whitacre, Sprotte, Gertie Marx):
- Rounded, non-cutting tip
- Separate (not cut) dural fibres — fibres spring back after needle withdrawal
- Side-opening aperture
- Significantly lower PDPH rates
- Miller's 10e (cited meta-analysis): "Noncutting needle tip designs have a lower frequency of post-dural puncture headache"
Bevel Orientation (for cutting needles):
- Dural fibres run longitudinally (parallel to spine)
- Quincke bevel inserted parallel to spine: separates fibres along their grain = smaller effective hole
- Quincke bevel inserted perpendicular: cuts across fibres = larger hole, more CSF loss
- Rule: always insert Quincke bevel parallel to the spine (bevel facing up or sideways in lateral position)
PART 6: DIFFERENTIAL DIAGNOSIS
"Not every headache after neuraxial anaesthesia is PDPH. You need a systematic approach."
| Diagnosis | Key Distinguishing Feature |
|---|---|
| PDPH | Postural — worse upright, better supine. Onset 12-72h post-procedure |
| Tension headache | No postural component. Bilateral, band-like. Common post-partum |
| Migraine | Unilateral, throbbing, photophobia, nausea. Personal history. No postural change |
| Pre-eclampsia headache | Hypertension (BP >140/90). No postural component. Associated with oedema, proteinuria |
| Meningitis (aseptic or bacterial) | Fever, neck stiffness, photophobia. Headache NOT postural. CSF pleocytosis on LP |
| Cortical venous thrombosis (CVT) | Constant headache (not postural). Focal deficits, seizures. MRI/MRV confirms |
| Subdural haematoma | Headache becomes CONSTANT (no longer postural) after initial PDPH. CT scan confirms |
| Non-specific post-neuraxial headache | Onset <12h, no postural component, resolves in <24h |
| Pneumocephalus | After loss-of-resistance to air technique. CT shows air in subarachnoid space. Worse upright |
| Caffeine-withdrawal headache | History of heavy caffeine use; relieved by caffeine |
PART 7: MANAGEMENT OF PDPH
7.1 Overview — Step-Up Approach
PDPH Confirmed
│
▼
Step 1: Conservative / Non-pharmacological
│ (Mild headache)
▼
Step 2: Pharmacological (non-invasive)
│ (Moderate headache, or failure of Step 1)
▼
Step 3: EPIDURAL BLOOD PATCH (Gold Standard)
│ (Severe / persistent / debilitating headache)
▼
Step 4: Rarely — repeat blood patch or surgical dural repair
7.2 Conservative / Non-Pharmacological Treatment
| Measure | Rationale | Evidence |
|---|---|---|
| Supine rest | ↓ hydrostatic pressure at dural defect → less CSF leak; relieves symptoms | Provides immediate symptomatic relief |
| Hydration (IV + oral) | Maintains circulating volume; stimulates CSF production | Supportive |
| Simple analgesics | Paracetamol 1g q6h; NSAIDs (ibuprofen 400-600 mg q8h) | Symptom control |
| Abdominal binder | ↑ intra-abdominal pressure → ↑ epidural venous pressure → ↓ CSF leak from defect | Limited evidence |
| Avoid Valsalva | Straining ↑ CSF pressure → ↑ leak through defect | Stool softeners, soft diet |
| Bed rest with call bell | Safety — fall risk from postural headache | Nursing measure |
7.3 Pharmacological (Non-Invasive) Treatments
Caffeine — First-Line Drug
- Dose: 300 mg orally OR 500 mg IV (as caffeine sodium benzoate in 1000 mL saline at 200 mL/hr)
- Mechanism:
- Adenosine receptor antagonist → cerebral vasoconstriction (reverses compensatory vasodilation)
- Stimulates CSF production
- Efficacy: Provides temporary relief in ~70% of cases — but effect is transient
- Limitation: Headache frequently recurs as caffeine wears off; does not seal the dural defect
- Barash 9e: "Caffeine (500 mg intravenously or 300 mg orally) has also been used in the treatment of PDPH, but the therapeutic effect is transient."
- Side effects: Tachycardia, insomnia, palpitations, anxiety, seizures at high doses
Theophylline
- Mechanism similar to caffeine (adenosine antagonist, cerebral vasoconstrictor)
- Oral theophylline shown effective in some studies
- Used when caffeine is unavailable or contraindicated
Gabapentin / Pregabalin
- Mechanism: Reduces central sensitisation and neuropathic pain
- Some studies show benefit as an adjunct
- Morgan & Mikhail 7e: "Intravenous gabapentin... has been shown to be successful in some studies"
Hydrocortisone / ACTH
- Proposed mechanism: Increases CSF production (by stimulating sodium-water transport at choroid plexus)
- ACTH (adrenocorticotrophic hormone): some evidence in refractory cases
- Morgan & Mikhail 7e mentions hydrocortisone as having some evidence
Triptans (e.g., Sumatriptan)
- Serotonin 5-HT1B/1D agonists → vasoconstriction
- Some case reports and small studies showing benefit
- Not yet standard of care
Cosyntropin (Synacthen)
- Synthetic ACTH analogue
- IV infusion reported in several studies to reduce PDPH severity
- Mechanism: Stimulates aldosterone → Na⁺ and water retention → ↑CSF production
Sphenopalatine Ganglion (SPG) Block
- SPG lies in the pterygopalatine fossa, innervates the meninges
- Technique: Long cotton-tipped applicators soaked in local anaesthetic (4% lidocaine or 2% xylocaine) inserted through the nares to the posterior nasopharynx bilaterally
- OR: intranasal lidocaine spray
- Provides temporary relief; minimal evidence base, but non-invasive and can buy time before EBP
- Morgan & Mikhail 7e: "Sphenopalatine ganglion block has been suggested as an approach to dural puncture headache. Local anesthetic is applied via swabs inserted into the posterior nasopharynx."
7.4 EPIDURAL BLOOD PATCH (EBP) — THE GOLD STANDARD DEFINITIVE TREATMENT
"This is the most important topic in PDPH management. Know every aspect of it. Know the indications, contraindications, technique, mechanism, success rate, and complications."
What is an Epidural Blood Patch?
Indications
- Moderate to severe PDPH not responding to 24-48 hours of conservative treatment
- PDPH with cranial nerve involvement (e.g., diplopia)
- PDPH severely impairing daily activities (especially in obstetric patients who need to care for their newborn)
- Patient request after counselling about conservative treatment failure
Timing
- Should NOT be performed in the first 24 hours after dural puncture as prophylaxis — 25-50% of patients will NOT develop PDPH even after ADP and receive unnecessary intervention
- Optimal timing: after 24-48 hours of failed conservative treatment
- Morgan & Mikhail 7e: "Delaying a blood patch for 24 h increases its efficacy, though supine bed rest for 24 h while awaiting the epidural blood patch is uncomfortable, inconvenient, and impractical for the new mother."
- Prophylactic EBP at time of ADP: Not recommended — Barash states "prophylactic administration of autologous blood does not influence the incidence and severity of PDPH"
Technique
- IV access secured, monitor attached, resuscitation equipment available
- Patient positioned in lateral decubitus or sitting
- Lumbar epidural space accessed at the same level or one level below the original dural puncture
- Two operators: One performs the epidural; one simultaneously draws blood under strict aseptic conditions
- Blood drawn from antecubital vein (same arm — reduces distance, maintains sterility)
- Aseptic technique throughout — contaminated blood injected into epidural space can cause epidural abscess/meningitis
- Volume: Inject 15-20 mL of autologous blood slowly into epidural space
- Stop if patient experiences:
- Backache (expected — normal)
- Radicular pain down the leg (nerve root compression — pause, allow to settle, continue cautiously)
- Neck pain (blood tracking up — STOP — can cause cranial nerve effects or brainstem compression)
- Patient kept supine for 1-2 hours after patch (prevents blood from dispersing before clot forms)
- Advise patient to avoid Valsalva for 24-48 hours (Valsalva raises CSF pressure and can disrupt the clot)
Mechanism of EBP — Two Phases
- Blood fills the epidural space → compresses the thecal sac → ↑CSF pressure → immediate relief
- This is the "mass effect" or "tamponade" mechanism
- Explains the rapid (minutes to hours) relief most patients experience
- Blood clots and forms a fibrin patch over the dural defect
- Seals the hole → stops CSF leak → intracranial pressure and volume normalise
- Permanent repair
Volume of Blood
- Standard recommendation: 15-20 mL (range 10-30 mL in literature)
- Too little: inadequate tamponade and insufficient clot to seal hole
- Too much: excessive epidural pressure → radicular pain, back pain, transiently increased neurological risk
- Volume of spread: 20 mL of blood spreads approximately 9 spinal segments in the epidural space (predominantly cephalad)
Success Rate
- ~90% of patients respond to a single EBP
- Of the 10% who do not respond: 90% will respond to a second EBP
- Therefore overall success rate with 1-2 patches: >98%
- Morgan & Mikhail 7e: "Approximately 90% of patients will respond to a single blood patch, and 90% of initial nonresponders will obtain relief from a second injection."
Contraindications to EBP
| Contraindication | Reason |
|---|---|
| Active systemic infection / sepsis | Blood from bacteraemic patient → epidural abscess |
| Fever / elevated CRP | Same reason — wait until infection resolved |
| Coagulopathy / anticoagulation | Epidural haematoma risk |
| Patient refusal | Informed consent required |
| Local infection at injection site | Epidural abscess |
| Raised intracranial pressure | Mass effect of EBP could worsen ICP |
| HIV/immunocompromised (relative) | Some advocate avoiding; others consider if benefits outweigh risks |
Complications of EBP
| Complication | Frequency | Comment |
|---|---|---|
| Backache | Very common (25-35%) | Usually resolves in 48-72 hours; expected |
| Radicular pain | Common (8-10%) | Transient; due to nerve root compression by blood |
| Dural puncture | ~1-2% | By Tuohy needle used for EBP itself |
| Recurrence of headache | 10-35% | Second EBP usually effective |
| Epidural abscess | Rare but severe | Strict asepsis mandatory |
| Epidural haematoma | Rare | Coagulopathy is a risk factor |
| Brainstem compression | Very rare | Blood tracks cephalad; neck pain is warning sign |
| Arachnoiditis | Very rare | Long-term complication |
| Failure | ~10% after first patch | Re-patch or re-evaluate diagnosis |
7.5 Alternative/Emerging Treatments
Epidural Saline
- 15-30 mL of saline injected into epidural space via existing catheter or fresh needle
- Mechanism: Tamponade effect (mass effect only — no sealing)
- Efficacy: Transient; works for 6-8 hours as saline absorbs
- Used as a temporising measure (especially if EBP not immediately available)
- Also used as prophylaxis when ADP recognised — epidural catheter saline infusion (500 mL-1L over 24 hours) may reduce PDPH incidence after ADP
Intrathecal Catheter after ADP
- When ADP is recognised with Tuohy needle during epidural attempt: leave a catheter in the intrathecal space and use it for spinal anaesthesia
- Proposed mechanism of headache prevention: The catheter prevents dural defect from retracting; the inflammatory reaction around the catheter promotes healing; reduced CSF leak
- Evidence: Inconsistent; Barash 9e: "Data supporting the use of intrathecal catheter placement for prevention of PDPH are inconsistent"
- If intrathecal catheter used: Must be clearly labelled; exceptional vigilance required against inadvertent intrathecal overdose
Fibrin Glue / Glue Patch
- Epidural injection of fibrin glue (commercial or cryoprecipitate)
- Used when EBP fails or when blood is contraindicated (HIV, infection, anticoagulated)
- Limited evidence; case reports primarily
PART 8: PREVENTION OF PDPH
"Prevention is better than treatment — especially because an EBP is itself an invasive procedure with its own risks."
8.1 Technical Strategies (Operator-Controlled)
- Use smallest gauge spinal needle appropriate for the clinical situation
- 25G or 27G pencil-point for routine spinal anaesthesia (rate: <2%)
- 22G pencil-point as compromise between adequate CSF flow and PDPH rate
- Use pencil-point needle design (Whitacre, Sprotte, Gertie Marx)
- Significantly lower PDPH rates at same gauge vs Quincke
- Orient Quincke bevel parallel to the spine (if cutting needle used)
- Bevel facing cephalad in sitting position; bevel facing ceiling in lateral position
- Replace stylet before withdrawing needle
- Prevents arachnoid strand being drawn through dura on withdrawal
- Limit number of attempts
- Multiple punctures = multiple dural holes
- Use ultrasound guidance to locate midline, identify interspace, estimate depth
- Paramedian approach may reduce wet tap rate in epidural placement
- Needle enters dura tangentially rather than perpendicularly
- Use loss-of-resistance to saline (not air) for epidural space identification
- Air can cause pneumocephalus if dural puncture occurs (worsens headache)
- Avoid aggressive needle insertion and recognise stop signs
- Free-flowing CSF = dural puncture; immediately acknowledge and re-plan
8.2 Pharmacological Prevention (after ADP is recognised)
- Epidural morphine (3 mg single dose): Some evidence of reduced PDPH incidence after ADP
- Epidural saline infusion (500 mL–1L over 24h): Temporary benefit; displaces CSF defect reduction
- Cosyntropin IV: Emerging evidence
- Prophylactic EBP at time of ADP: NOT RECOMMENDED — 25-50% of patients won't develop PDPH; exposes them to EBP risks unnecessarily
PART 9: SPECIAL SITUATIONS
9.1 PDPH in Obstetric Patients
- Accidental dural puncture (ADP) with 18G Tuohy needle in obstetric epidural placement = 50-80% chance of PDPH
- After delivery, epidural space pressure decreases → increased CSF drainage through defect
- Estrogen withdrawal after placental delivery may exacerbate vascular component
- Barash 9e: "After delivery, reduced pressure in the epidural space may increase the risk of cerebrospinal fluid leakage through a dural puncture, and estrogen withdrawal after delivery of the placenta may exacerbate vascular headaches."
- Post-partum depression has been associated with PDPH — patient cannot care for newborn; bonding impaired
- Anaesthetic management after ADP in obstetrics:
- Inform patient and obstetrician immediately and document
- Options: (a) Remove epidural, use intrathecal catheter at the same site; (b) Remove epidural, re-site in adjacent interspace; (c) Proceed with spinal anaesthesia
- If ADP used for analgesia — clearly label as "INTRATHECAL" — dramatically reduce local anaesthetic doses
- Monitor for PDPH closely for 72 hours post-procedure
9.2 Accidental Dural Puncture (ADP) Management Protocol
- Stop advancing needle immediately
- Communicate with patient and team
- Decisions:
- Abandon procedure and re-site: higher chance of second ADP, but avoids intrathecal catheter risk
- Leave catheter intrathecal: allows spinal anaesthesia/analgesia, may reduce PDPH, but overdose risk
- Document clearly: level, size of needle, management plan
- Inform: Senior anaesthetist, obstetrician, patient
- Post-procedure: Monitor for PDPH ×72h; initiate conservative management; plan EBP if PDPH develops
- Discharge advice: Explain PDPH symptoms; provide contact number; arrange follow-up
PART 10: LONG-TERM SEQUELAE
- Chronic headache
- Chronic back pain
- Auditory impairment (CN VIII traction/ischaemia)
- Postpartum depression"
- Subdural haematoma (tearing of bridging veins)
- Cerebral venous thrombosis (venous stasis secondary to intracranial hypotension)
- Bacterial meningitis (from contamination at time of procedure)
PART 11: VIVA QUESTIONS — MD FINAL EXAM LEVEL
- Headache that worsens within 15 minutes of sitting/standing and improves within 15 minutes of lying down
- At least one of: neck stiffness, tinnitus, hypacusia, photophobia, nausea
- Has developed within 5 days of dural puncture
- Not better accounted for by another diagnosis The postural component is the cardinal diagnostic feature. In more than 90% of cases onset is within 3 days of the procedure.
- Moderate to severe backache — normal and expected due to epidural space expansion; pause briefly, can resume cautiously
- Radicular pain (electric shock down the leg) — nerve root compression by blood; stop, wait for it to resolve, can cautiously re-attempt
- Neck pain or occipital pressure — blood is tracking cephalad toward the craniocervical junction; STOP IMMEDIATELY — risk of brainstem compression
- Patient cannot tolerate any more injection
- Re-assess the headache carefully — is it still postural? If yes, this is likely PDPH recurrence (the patch has partially failed or redistributed before fully sealing). If the headache is now constant (non-postural), I must urgently consider subdural haematoma — the bridging veins may have torn during the period of intracranial hypotension. Urgent CT/MRI head required.
- If PDPH recurrence confirmed: Second epidural blood patch is appropriate — success rate for second patch is ~90% of initial failures.
- Check timing: was the first EBP done within 24 hours of ADP (when it is known to be less effective)?
- Check volume injected: was it adequate (≥15 mL)?
- Check for contraindications to repeating EBP (coagulopathy, fever).
- Counsel patient about the second EBP.
- If second EBP also fails: re-evaluate diagnosis, consider neurology/neurosurgery referral, consider MRI spine to look for epidural CSF leak, consider fibrin glue or surgical dural repair (rare).
- Early PDPH (within 12 hours) can occasionally occur without a fully developed postural component — but should be watched closely
- Subarachnoid haemorrhage — thunderclap onset, severe ("worst headache of life"), not postural
- Bacterial meningitis — LP itself can seed infection; fever + meningismus + non-postural headache = emergency
- Raised intracranial pressure — if LP was performed in a patient with raised ICP (contraindicated), post-LP herniation is a catastrophic emergency
- Pneumocephalus — if air was used during the LP
Summary Table — High-Yield Facts for MD Final Exam
| Question | Answer |
|---|---|
| First described by | August Bier, 1898 |
| Pathophysiology | CSF leak → traction on intracranial structures + compensatory cerebral vasodilation |
| Cardinal feature | Postural headache — worse upright, relieved lying flat |
| Onset | 12-72 hours; >90% within 3 days |
| Spontaneous resolution | 72% by 7 days; 87% by 6 months |
| Highest incidence | Young, female, pregnant + large gauge cutting needle |
| Incidence with 16G needle | >70% |
| Incidence with 25G pencil-point | <1% |
| Most common cranial nerve | CN VI (abducens) — diplopia |
| First-line drug | Caffeine (300 mg oral / 500 mg IV) |
| Gold standard treatment | Epidural Blood Patch |
| EBP volume | 15-20 mL autologous blood |
| EBP success rate (1 patch) | ~90% |
| Stop EBP if | Neck pain (blood tracking cephalad) |
| Prophylactic EBP | NOT recommended |
| EBP timing | After 24-48 hours of failed conservative treatment |
| Most dangerous complications | Subdural haematoma, cerebral venous thrombosis, bacterial meningitis |
| EBP contraindication | Active infection / sepsis / fever / coagulopathy |
Professor's Closing Note: "PDPH sits at the intersection of physics, anatomy, pharmacology, and clinical skill. It is almost entirely preventable — choose the right needle, use the right technique, orient the bevel correctly. When it does happen, be honest with the patient, treat aggressively, and never dismiss it as 'just a headache.' A young mother with PDPH cannot hold her baby. That is your patient. That is your responsibility. The epidural blood patch is one of the most satisfying procedures in anaesthesia when you watch a woman who has been bedridden for 2 days sit up, smile, and say 'the headache is gone.' Know how to do it well. Know when to do it. And know when NOT to."
- Miller's Anesthesia, 10e — Chapter on Neuraxial Anesthesia: Post-Dural Puncture Headache
- Morgan & Mikhail's Clinical Anesthesiology, 7e — Chapter 45: Obstetric Anaesthesia; Chapter on Spinal Anaesthesia
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e — Chapter on Obstetric Anaesthesia: PDPH
- Rosen's Emergency Medicine — Post-Dural Puncture and Low CSF Pressure Headaches