I have to understand COPD fully with each points like pathophysiology cf and mangrment
Reading File
Finding Sources
Searching PubMed
"COPD" AND "management"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-structured answer.
Chronic Obstructive Pulmonary Disease (COPD) - Complete Guide
1. Definition
COPD is a chronic, progressive, largely irreversible respiratory disease characterized by persistent airflow limitation due to an abnormal inflammatory response of the lungs to noxious particles or gases, most importantly cigarette smoke. It most commonly manifests as emphysema and/or chronic bronchitis, which typically coexist.
- Chronic bronchitis is defined clinically: persistent productive cough for at least 3 consecutive months in at least 2 consecutive years
- Emphysema is defined anatomically: permanent enlargement and destruction of airspaces distal to the terminal bronchioles
2. Epidemiology & Risk Factors
- Third most common cause of death in the United States
- Costs over $40 billion/year in direct and indirect healthcare costs
- Only 10-15% of smokers develop clinically significant disease (genetic susceptibility matters)
- Heritability of COPD is estimated at 37-50%
- COPD usually develops ~10-12 years after smoking initiation
Risk Factors:
| Category | Factors |
|---|---|
| Most common | Cigarette smoking (primary) |
| Environmental | Air pollution, occupational dusts, chemical fumes, biomass fuels |
| Genetic | Alpha-1 antitrypsin (A1AT) deficiency, TERT polymorphisms |
| Other | Recurrent childhood respiratory infections, low socioeconomic status |
Any patient developing COPD before age 45 or without significant smoking history should be screened for A1AT deficiency
3. Pathophysiology
3a. Core Mechanism - Protease-Antiprotease Imbalance
The central pathologic event is an imbalance between proteases and antiproteases in the lung:
- Noxious stimuli (cigarette smoke, pollutants) → recruitment of neutrophils, macrophages, and CD8+ lymphocytes to the lung
- These inflammatory cells release proteases (elastase, matrix metalloproteinases)
- Proteases destroy the elastic support structures of alveolar walls
- Normally, alpha-1 antitrypsin (A1AT) inhibits neutrophil elastase - when this fails, destruction proceeds unchecked
- Oxidative stress from reactive oxygen species amplifies the inflammatory cascade
3b. Emphysema Pathway
Cigarette smoke → Alveolar macrophage + Neutrophil activation
↓
Protease release (elastase, MMPs)
↓
Alveolar wall destruction + Loss of elastic recoil
↓
Enlarged air spaces + Air trapping (static hyperinflation)
↓
Loss of radial tethering → Dynamic airway collapse on expiration
↓
Dynamic hyperinflation → Barrel chest
- Cigarette smoking also causes intimal thickening and smooth muscle proliferation in pulmonary vasculature, with decreased VEGF expression and endothelial cell apoptosis, contributing to pulmonary hypertension
3c. Chronic Bronchitis Pathway
Tobacco smoke / pollutants → Mucosal irritation
↓
Goblet cell metaplasia + Mucous gland hypertrophy (Reid index >0.4)
↓
MUC5AC concentration ↑ 10-fold; MUC5B ↑ 3-fold
↓
Mucus hypersecretion + Ciliary dysfunction (CFTR ↓, ENaC ↑)
↓
Persistent airway infection (especially H. influenzae)
↓
Small airway inflammation → Bronchiolitis → Fibrosis
↓
Airflow obstruction (primary site = small airways <2 mm)
3d. Emphysema Subtypes
| Type | Location | Cause | Features |
|---|---|---|---|
| Centriacinar (most common) | Central part of acinus (respiratory bronchioles) | Cigarette smoking | Upper lobe predominant |
| Panacinar | Entire acinus uniformly | Alpha-1 antitrypsin deficiency | Lower lobe predominant |
| Paraseptal | Distal part of acinus near pleura | Unknown | Risk factor for spontaneous pneumothorax |
| Irregular | Scar-related | Post-inflammatory scarring | Clinically less significant |
3e. Pulmonary Function Consequences
- Increased residual volume (RV) and functional residual capacity (FRC) due to air trapping
- Decreased FEV1 due to loss of elastic recoil and airflow obstruction
- FEV1/FVC ratio < 0.70 (hallmark of obstructive defect)
- V/Q mismatch → hypoxemia
- Dynamic hyperinflation → diaphragm flattening, barrel chest, increased work of breathing
- In emphysema: hypoxemia alone (compensated by hyperventilation)
- In chronic bronchitis: both hypoxemia and hypercapnia (CO2 retention)
4. Genetics - Alpha-1 Antitrypsin Deficiency
- Most common monogenic risk factor for COPD
- Encoded by the SERPINA1 gene - product is a serine protease inhibitor synthesized and secreted by the liver
- Alleles designated by electrophoretic mobility: M (normal), S (slow), Z (ultraslow)
- Normal genotype: PiMM (present in ~95% of adults)
- Pathologic genotypes: PiZZ (most severe - very low A1AT), PiSS, PiZS
- PiZZ homozygotes have markedly elevated risk of emphysema (panacinar, lower lobe)
- Even PiMZ heterozygotes show more airflow impairment and CT emphysema than PiMM
5. Clinical Features
Classic Presentation
- Onset in midlife (typically after age 40), with slow progression over decades
- Progressive dyspnea - initially only on exertion, later at rest
- Chronic productive cough (morning sputum common)
- Long history of cigarette smoking
Emphysema "Pink Puffer" vs. Chronic Bronchitis "Blue Bloater"
| Feature | Emphysema ("Pink Puffer") | Chronic Bronchitis ("Blue Bloater") |
|---|---|---|
| Build | Thin, cachectic | Overweight |
| Cyanosis | Absent (pink) | Present (blue) |
| Cough/sputum | Minimal | Copious productive cough |
| Dyspnea | Severe, at rest | Less severe |
| Hypoxemia | Mild (hyperventilates to compensate) | Severe |
| Hypercapnia | No (low PaCO2) | Yes (high PaCO2) |
| PFTs | Increased TLC, RV; decreased DLCO | Obstruction; near-normal DLCO |
| CXR | Hyperinflation, flat diaphragms, bullae | Cardiomegaly, increased markings |
Physical Examination Signs
- Barrel chest (increased AP diameter) - due to chronic hyperinflation
- Flattened diaphragm on chest X-ray and percussion
- Prolonged expiratory phase with expiratory wheeze
- Decreased breath sounds globally
- Use of accessory muscles of respiration
- Pursed-lip breathing (to maintain positive expiratory pressure)
- In severe disease: peripheral edema, cyanosis, cor pulmonale
Chest X-Ray Findings (COPD)
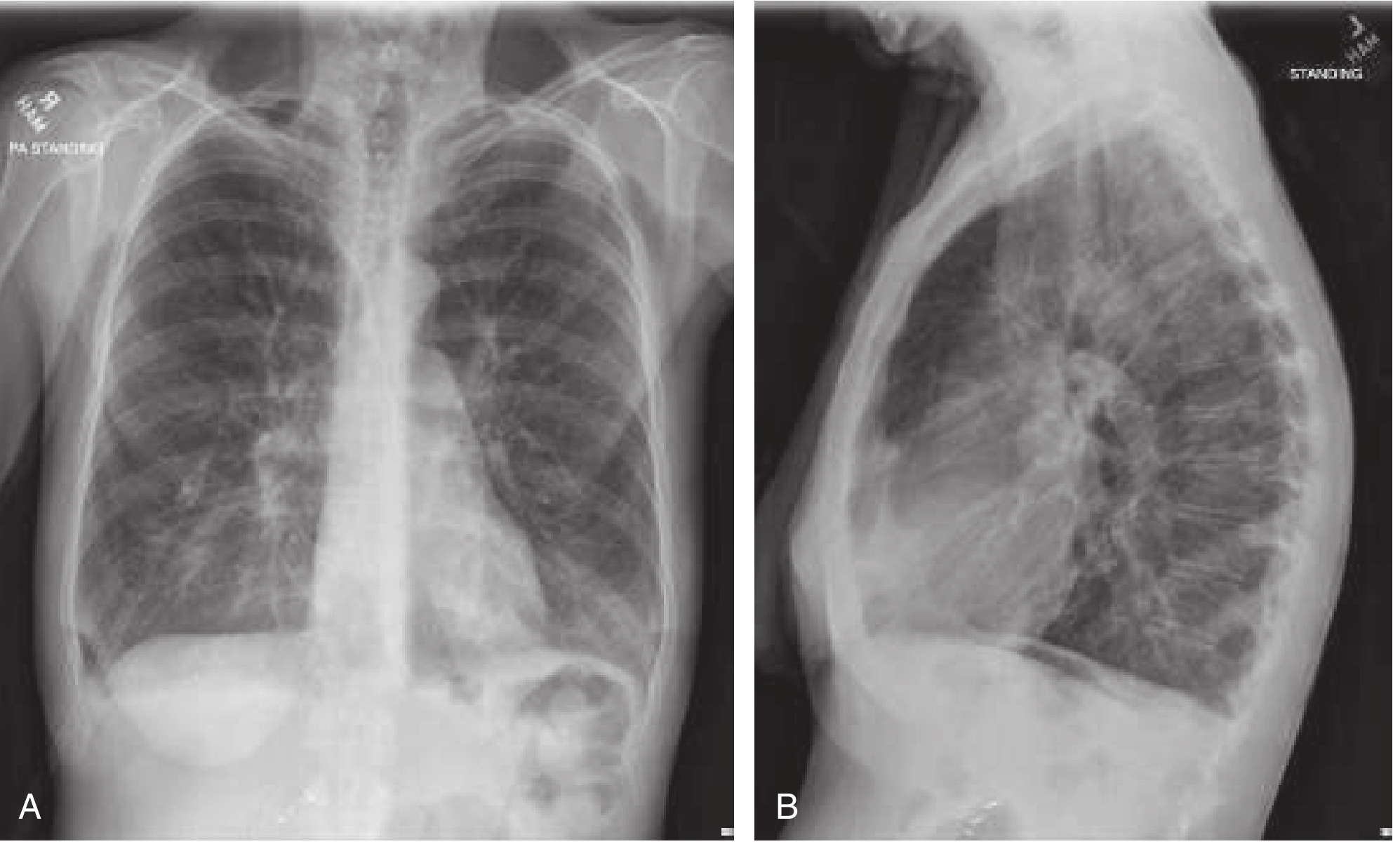
PA view (A): hyperinflated lungs, flattened diaphragm, decreased vascular markings. Lateral (B): flattened diaphragm and increased AP diameter - Rosen's Emergency Medicine
6. Diagnosis
Key Diagnostic Test: Spirometry
- COPD is diagnosed by post-bronchodilator FEV1/FVC < 0.70
- Unlike asthma, airflow limitation in COPD is not fully reversible (< 12% improvement with bronchodilator)
- Patients with normal spirometry but symptoms + CT emphysema are NOT classified as COPD
Key PFT Pattern in COPD:
- ↓ FEV1
- ↓ FEV1/FVC ratio (< 0.70)
- ↑ RV and TLC (air trapping)
- ↓ DLCO (in emphysema - destruction of gas exchange surface)
- Normal or near-normal FVC
GOLD Classification (Severity by FEV1 post-bronchodilator, with FEV1/FVC < 0.70)
| GOLD Grade | Severity | FEV1 (% predicted) |
|---|---|---|
| GOLD 1 | Mild | ≥ 80% |
| GOLD 2 | Moderate | 50-79% |
| GOLD 3 | Severe | 30-49% |
| GOLD 4 | Very Severe | < 30% |
GOLD ABCD Assessment Tool (Beyond Spirometry)
In addition to grading, patients are categorized A-D based on:
- Symptom burden: assessed by mMRC (≥2 = more symptomatic) or CAT score (≥10 = high symptoms)
- Exacerbation history: ≥2 moderate exacerbations/year, or ≥1 requiring hospitalization = high risk
| Group | Exacerbations | Symptoms |
|---|---|---|
| A | Low risk | Few |
| B | Low risk | More |
| E (formerly C/D) | High risk | Variable |
Other Investigations
- ABG: hypoxemia (PaO2 < 60 mmHg), possible hypercapnia (PaCO2 > 45 mmHg), A-a gradient elevated
- CXR: hyperinflation, flat diaphragms, bullae, increased AP diameter
- HRCT chest: best for identifying emphysema pattern, extent; also detects bronchiectasis
- ECG: right ventricular strain pattern (P pulmonale, right axis deviation) in cor pulmonale; arrhythmias in up to 35%
- A1AT level: screen if young onset or no smoking history
- CBC: polycythemia (secondary, due to chronic hypoxia)
- 6-minute walk test: distance < 149 m = severe functional limitation
7. Complications
- Cor pulmonale (right heart failure): from chronic hypoxia → pulmonary vasoconstriction → pulmonary hypertension → right ventricular hypertrophy and failure
- Pulmonary hypertension
- Acute exacerbations (major driver of morbidity and mortality)
- Recurrent respiratory tract infections (H. influenzae, S. pneumoniae, M. catarrhalis; viral most common)
- Respiratory failure (hypoxic and/or hypercapnic)
- Pneumothorax (especially with bullous disease/paraseptal emphysema)
- Secondary polycythemia (compensatory erythrocytosis)
- Cardiovascular disease: increased risk of coronary artery disease, arrhythmias, heart failure (major comorbidity)
- Lung cancer: significantly elevated risk
- Malnutrition, cachexia, and muscle wasting
- Obstructive sleep apnea (overlap syndrome)
- Depression and anxiety (very common, often undertreated)
8. Management
8a. Non-Pharmacological (All Patients)
| Intervention | Notes |
|---|---|
| Smoking cessation | Single most effective intervention - slows rate of FEV1 decline |
| Vaccinations | Influenza (annual), pneumococcal, COVID-19, tdap |
| Pulmonary rehabilitation | Improves exercise tolerance, dyspnea, quality of life |
| Nutritional support | Small frequent meals; avoid gas-forming foods (worsens dyspnea) |
| Oxygen therapy | Long-term O2 (LTOT) if PaO2 ≤ 55 mmHg or SaO2 ≤ 88% (only treatment shown to improve mortality in hypoxemic COPD) |
| Activity/exercise | 6-min walk test to guide |
8b. Pharmacological - Stable COPD
Step-wise approach based on GOLD ABCD group:
Bronchodilators are the cornerstone of stable COPD management:
| Drug Class | Examples | Mechanism | Use |
|---|---|---|---|
| SABA (Short-acting beta2-agonist) | Albuterol (salbutamol) | Bronchodilation (acute) | Rescue - all groups |
| SAMA (Short-acting muscarinic antagonist) | Ipratropium | Bronchodilation, reduces secretions | Rescue/adjunct |
| LABA (Long-acting beta2-agonist) | Salmeterol, Formoterol, Indacaterol | Sustained bronchodilation | Maintenance: Group B/E |
| LAMA (Long-acting muscarinic antagonist) | Tiotropium, Umeclidinium, Aclidinium | Sustained bronchodilation + reduces dynamic hyperinflation | Maintenance: preferred in Group B/E |
| ICS (Inhaled corticosteroid) | Fluticasone, Budesonide | Anti-inflammatory | Add-on: Group E with blood eosinophils ≥100/µL; NOT first-line |
| LABA + LAMA (dual bronchodilator) | Umeclidinium/vilanterol | Superior to either alone | Moderate-severe COPD |
| LABA + ICS | Salmeterol/fluticasone | Group E (high exacerbation risk, eosinophilic) | |
| Triple therapy (LABA+LAMA+ICS) | Budesonide/glycopyrrolate/formoterol | Very severe, frequent exacerbations | |
| PDE4 inhibitor | Roflumilast | Reduces inflammation; improves lung function, reduces exacerbation frequency | Add-on: chronic bronchitis phenotype, frequent exacerbations, GOLD 3-4 |
| Azithromycin (chronic) | Prophylactic | Anti-inflammatory + antibacterial | Reduce exacerbations (former smokers, frequent exacerbations) |
| N-acetylcysteine | Mucolytic | Reduces sputum viscosity | Adjunct for mucus hypersecretion |
Key note on ICS: Recommended ONLY for severe airflow obstruction, frequent exacerbations, or blood eosinophils ≥ 100-300/µL. Avoid in patients with low eosinophils due to higher bacterial pneumonia risk and limited benefit. Blood eosinophil count now guides ICS decision-making in COPD.
Theophylline: A recent large placebo-controlled RCT found low-dose theophylline did NOT reduce exacerbation frequency - no longer recommended.
8c. Surgical Options (Severe COPD)
- Lung volume reduction surgery (LVRS): for upper-lobe predominant emphysema with poor exercise capacity; improves survival in selected patients
- Bullectomy: for giant bullae compressing normal lung tissue
- Lung transplantation: for end-stage COPD (GOLD 4), especially A1AT deficiency-related
- Bronchoscopic lung volume reduction: endobronchial valves (Zephyr) as less invasive alternative
9. Acute Exacerbation of COPD (AECOPD)
An exacerbation is an acute worsening of respiratory symptoms beyond day-to-day variation, requiring additional therapy.
Triggers
- Viral respiratory infections (most common - ~50-70%)
- Bacterial infections (30-50%): H. influenzae, S. pneumoniae, M. catarrhalis (Pseudomonas in severe/bronchiectatic disease)
- Environmental pollutants, particulate matter
- Temperature changes, pulmonary embolism
Severity Assessment - Indications for Hospitalization
- Severe dyspnea not responding to initial therapy
- Change in mental status (confusion, lethargy)
- PaO2 < 40 mmHg or SaO2 < 90%
- PaCO2 > 60 mmHg or pH ≤ 7.25
- Hemodynamic instability
- Failure of outpatient treatment
- Significant comorbidities (CHF, arrhythmias, electrolyte imbalance)
Treatment of AECOPD
1. Bronchodilators (first-line)
- SABA ± SAMA via nebulizer or MDI with spacer
- Combining ipratropium + albuterol is more effective than either alone
2. Corticosteroids
- Oral prednisone 40 mg for 5 days (5-day = as effective as longer courses)
- Decrease recovery time, improve oxygenation, improve lung function, decrease hospital stay
- IV methylprednisolone if patient cannot take oral
3. Antibiotics (when indicated)
- Indicated if: increased sputum purulence PLUS increased dyspnea OR increased sputum volume (Anthonisen criteria)
- First-line: amoxicillin/clavulanate, macrolides (azithromycin), or tetracyclines (doxycycline)
- Coverage for Pseudomonas if: severe airflow limitation, known bronchiectasis, or requiring mechanical ventilation
- Duration: 5 days macrolides; 7 days amoxicillin/clavulanate or tetracyclines
4. Oxygen Therapy
- Target SpO2: 88-92% (not higher - avoids hypercapnia from altered V/Q and loss of hypoxic vasoconstriction)
- Titrate carefully - both hypoxemia AND hyperoxemia are harmful
5. Non-invasive Ventilation (NIV/BiPAP)
- Indicated for: moderate to severe respiratory failure with pH < 7.35 and PaCO2 > 45
- Reduces risk of intubation by 65%, in-hospital mortality by 55%, hospital stay by 1.9 days
- Requires: normal mental status, hemodynamic stability, no high aspiration risk
- ~80% of appropriate patients improve within 4 hours
6. Invasive Mechanical Ventilation
- For patients who fail NIV or have contraindications
- Worsening mental status, respiratory arrest, hemodynamic instability
7. Adjunctive Measures
- DVT prophylaxis (subcutaneous heparin)
- Cardiac monitoring (arrhythmias in up to 35% of exacerbations)
- Electrolyte monitoring and correction
- Vitamin D supplementation if deficient (< 25 nmol/L)
- Smoking cessation counseling
- Ensure up-to-date vaccinations
10. Differential Diagnosis of COPD
| Condition | Key Distinguishing Features |
|---|---|
| Asthma | Early onset, reversible obstruction, allergic history, night/morning symptoms |
| Congestive heart failure | Fine basilar crackles, volume restriction on PFTs, cardiomegaly on CXR |
| Bronchiectasis | Copious purulent sputum, clubbing, coarse crackles, CT shows dilated bronchi |
| Tuberculosis | Upper lobe infiltrates, microbiologic confirmation, high-prevalence setting |
| Obliterative bronchiolitis | Non-smoker, younger patient, history of RA or fume exposure, mosaic pattern on HRCT |
| Diffuse panbronchiolitis | Asian males, chronic sinusitis, centrilobular nodules on HRCT |
11. Summary Table - "Pink Puffer vs Blue Bloater" Physiology (from Costanzo Physiology)
From the clinical case in Costanzo's Physiology: a 65-year-old 2-pack/day smoker shows a low PaO2 (60 mmHg) but the calculated PAO2 is 113 mmHg - indicating a large A-a gradient from V/Q mismatch. The low FEV1/FVC confirms obstructive disease, and the barrel chest reflects chronic hyperinflation. The mild respiratory alkalosis (pH 7.47, low PaCO2 of 30) reflects compensatory hyperventilation driven by hypoxemia stimulating peripheral chemoreceptors.
12. Recent Evidence (2024-2026)
- AECOPD risk prediction (2024) - A 2024 systematic review/meta-analysis in Respiratory Research analyzed prognostic risk prediction models for acute exacerbations (PMID: 39543648)
- Digital health for COPD (2025) - A 2025 meta-analysis in J Med Internet Res found digital health interventions improve COPD outcomes (PMID: 40418567)
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Goldman-Cecil Medicine
- Murray & Nadel's Textbook of Respiratory Medicine
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Costanzo Physiology, 7th Edition
- Textbook of Family Medicine, 9th Edition
This is a shared conversation. Sign in to Orris to start your own chat.