teach me tvs with real time sonographic pictures and anatomical landmark
transvaginal ultrasound technique anatomical landmarks sonographic images tutorial
https://www.pocus101.com/gynecology-pelvic-ultrasound-made-e…
transvaginal ultrasound sonographic images uterus ovary sagittal transverse landmarks site:pocus101.com OR site:radiologykey.com
https://www.ncbi.nlm.nih.gov/books/NBK572084
transvaginal ultrasound endometrium cervix ovary follicles sonogram labeled anatomy
Transvaginal Sonography (TVS) - Complete Teaching Guide
What is TVS and Why Use It?
| Feature | TVS | TAS |
|---|---|---|
| Probe frequency | 5-10 MHz (high res) | 3-5 MHz |
| Bladder needed | Empty | Full (acoustic window) |
| Field of view | Narrow, close | Wide, distant |
| Resolution | Superior | Limited |
| Best for | Uterus, endometrium, ovaries | Broad pelvic survey, large masses |
Patient Preparation and Setup
- Position: Dorsal lithotomy (like a pelvic exam), with hips slightly elevated on a pillow or padded stirrups
- Bladder: Should be empty (full bladder displaces and compresses pelvic organs, degrading the TVS image)
- Probe cover: Always use a sterile condom/glove with coupling gel inside and outside the cover
- Chaperone: Required; document consent and the chaperone's presence
The Probe and Probe Orientation
- Sagittal (longitudinal) view: Marker at 12 o'clock (pointing toward the ceiling) - cephalad structures appear on the left side of the screen
- Transverse (coronal) view: Rotate probe 90° counterclockwise - marker at 9 o'clock (patient's right), so the patient's right appears on the left of the screen
Tip: Keep your thumb aligned with the probe indicator throughout the exam - this lets you track probe orientation no matter how much you manipulate it.
Probe Movements - The Four Maneuvers
| Maneuver | Motion | What it does |
|---|---|---|
| Tilt / Fan | Angle the shaft up-down or left-right | Sweeps the beam across structures |
| Advance / Retract | Move probe in/out of vaginal canal | Changes depth and target structure |
| Rotate | Turn around longitudinal axis | Switches between sagittal and transverse planes |
| Press | Firm pressure against vaginal wall | Displaces bowel, brings ovary into view |
Step-by-Step Scanning Protocol
Step 1 - Sagittal View of the Uterus
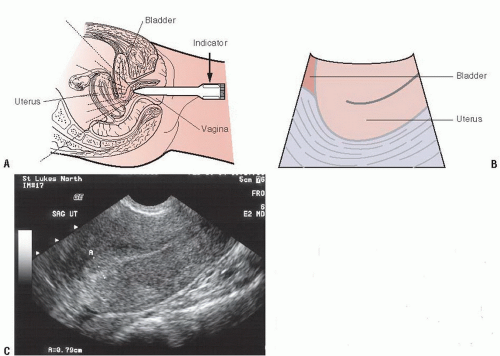
| Landmark | Sonographic Appearance |
|---|---|
| Bladder | Anechoic (black), anterior - may be partially visible even when empty |
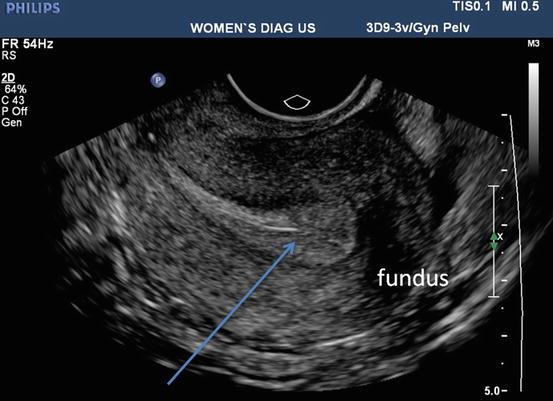
| Uterine fundus | Rounded, homogeneous echogenicity - most superior part |
| Myometrium | Intermediate echogenicity, surrounds the endometrium |
| Endometrial stripe | Central hyperechoic (bright) line/zone - varies with menstrual cycle |
| Cervix | Posterior to uterine body, connects downward; fibrous, slightly hyperechoic |
| Endocervical canal | Thin bright line within the cervix |
| Pouch of Douglas (POD) | Posterior to the uterus - look for anechoic free fluid here |
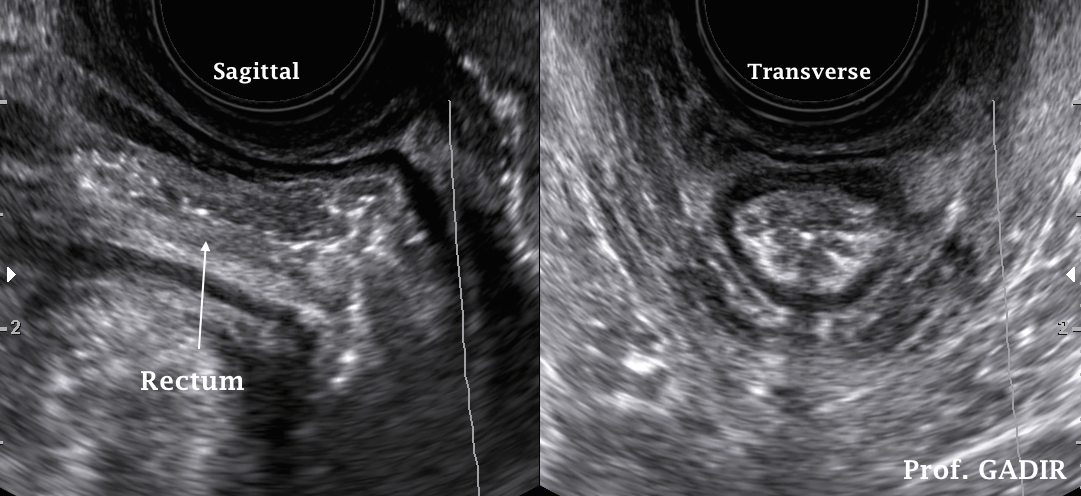
| Rectum | Posterior; bowel wall layers visible |
- Anteverted/anteflexed (most common, ~80%): Fundus tips forward toward bladder; on sagittal TVS you see the fundus at the top-left of the image
- Retroverted/retroflexed (~20%): Fundus tips backward; the cervix appears first and you follow it posteriorly to the fundus; repositioning the probe into the posterior fornix helps
| Phase | Appearance | Thickness |
|---|---|---|
| Early proliferative | Thin, single bright line | 4-8 mm |
| Late proliferative | Triple-line / trilaminar (two outer bright lines + central line with hypoechoic zone between) | 8-12 mm |
| Secretory | Thick, uniformly echogenic (bright) | 10-16 mm |
| Postmenopausal (normal) | Thin, bright line | ≤ 4-5 mm |
- Length: fundus to external cervical os (normal 6-10 cm in reproductive age)
- Anteroposterior diameter: widest AP dimension of the uterine body
- Endometrial thickness: measured bilayer (both layers together) at widest point, excluding fluid
Step 2 - Transverse (Coronal) View of the Uterus
- A round/oval cross-section of the uterus
- The bright endometrial echo in the center
- Both cornua visible when angled superiorly (fundal transverse)
- The "owl face" appearance: two round cornua flanking the central echo
Step 3 - Cervix View
- The cervical stroma (fibrous, intermediate-to-high echogenicity)
- The endocervical canal as a central bright line
- The anterior lip and posterior lip of the cervix
- The external os (V-shaped notch at the bottom)
- The posterior vaginal fornix (inferior to posterior lip)
- Nabothian cysts: small, round, anechoic - benign retention cysts in the cervical stroma
Step 4 - Ovaries
- Start in the transverse plane (indicator at 9 o'clock)
- Fan/tilt the probe toward the right iliac fossa (rock the handle to the patient's left to see the right ovary)
- Follow the ovarian ligament or use the iliac vessels as a guide - the ovary lies just medial to the internal iliac vein

| Feature | Normal value |
|---|---|
| Size | 2-3 cm (length), volume 5-15 mL reproductive age |
| Echogenicity | Slightly less echogenic than myometrium |
| Texture | Homogeneous stroma with anechoic follicles |
| Follicles | Multiple small anechoic peripheral follicles (antral follicles, 2-10 mm each) |
| Dominant follicle | Up to ~20-25 mm at ovulation (anechoic, thin-walled) |
Step 5 - Adnexa and Pouch of Douglas
Summary Image Checklist for a Complete TVS Exam
- Cervix - sagittal (with endocervical canal)
- Uterus midline - sagittal (full length with endometrial measurement)
- Uterine fundus - transverse (with cornua)
- Right ovary - long axis (with 3-plane measurements)
- Right adnexa - any abnormality
- Left ovary - long axis (with 3-plane measurements)
- Left adnexa - any abnormality
- Pouch of Douglas - free fluid assessment
Echogenicity Quick Reference
| Structure | Appearance on TVS |
|---|---|
| Fluid (follicle, cyst, free fluid, blood) | Anechoic (black) |
| Endometrium (secretory phase) | Hyperechoic (bright white) |
| Myometrium | Intermediate gray |
| Bowel gas | Hyperechoic with posterior shadowing |
| Bone/calcification | Hyperechoic with posterior shadow |
| Endometrial triple line | Two bright outer lines + dark middle zone |
Common TVS Findings and What They Look Like
| Pathology | Key Sonographic Feature |
|---|---|
| Endometrial polyp | Focal hyperechoic endometrial thickening; vascular pedicle on Doppler |
| Fibroid (submucosal) | Hypoechoic mass distorting the endometrial echo |
| Ovarian cyst (simple) | Thin-walled, anechoic, posterior acoustic enhancement |
| Ectopic pregnancy | Adnexal ring sign outside the uterus; empty uterine cavity; free fluid in POD |
| PCOS | Multiple small peripheral follicles (≥12 follicles per ovary, 2-9 mm) - "string of pearls"; increased stroma echogenicity |
| Endometrioma | "Ground glass" appearance - homogeneous low-level internal echoes |
| Hydrosalpinx | Tortuous, fluid-filled tubular adnexal structure |
Key Points to Remember
- Always do TAS first, then TVS - they are complementary; TAS gives the big picture, TVS gives the detail.
- Empty bladder for TVS - a full bladder compresses and displaces structures.
- Probe indicator orientation is everything - lose track of it and your anatomy orientation collapses.
- Internal iliac vessels are your ovary GPS - find the hypogastric vessels, and the ovary will be nearby.
- Endometrial thickness changes with the cycle - always correlate with menstrual history.
- A little free fluid in the POD is normal - especially in the luteal phase; complex or large-volume fluid is not.
- Normal fallopian tubes are invisible on TVS - if you see a tube, it's pathological.
Generate a quick reference poster comparing normal vs abnormal TVS findings
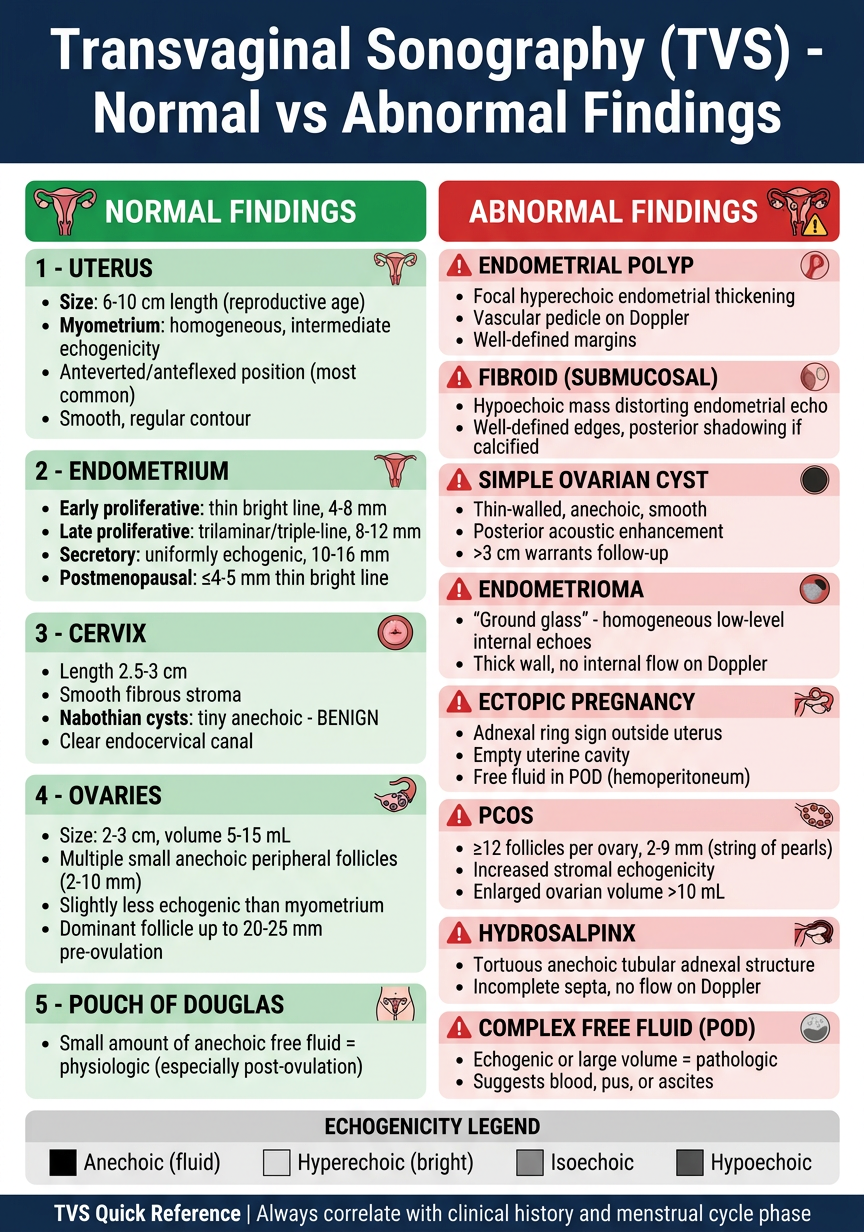
A professional medical quick reference poster titled "Transvaginal Sonography (TVS) - Normal vs Abnormal Findings" designed for clinical use. The poster has a clean dark navy blue header with white title text. Below the header, the poster is divided into two main columns side by side: LEFT COLUMN with a green header "NORMAL FINDINGS" and RIGHT COLUMN with a red header "ABNORMAL FINDINGS". LEFT COLUMN - NORMAL FINDINGS (green accents): Section 1 - UTERUS: • Size: 6-10 cm length (reproductive age) • Myometrium: homogeneous, intermediate echogenicity • Anteverted/anteflexed position (most common) • Smooth, regular contour Section 2 - ENDOMETRIUM: • Early proliferative: thin bright line, 4-8 mm • Late proliferative: trilaminar/triple-line, 8-12 mm • Secretory: uniformly echogenic, 10-16 mm • Postmenopausal: ≤4-5 mm thin bright line Section 3 - CERVIX: • Length 2.5-3 cm • Smooth fibrous stroma • Nabothian cysts: tiny anechoic - BENIGN • Clear endocervical canal Section 4 - OVARIES: • Size: 2-3 cm, volume 5-15 mL • Multiple small anechoic peripheral follicles (2-10 mm) • Slightly less echogenic than myometrium • Dominant follicle up to 20-25 mm pre-ovulation Section 5 - POUCH OF DOUGLAS: • Small amount of anechoic free fluid = physiologic (especially post-ovulation) RIGHT COLUMN - ABNORMAL FINDINGS (red accents), each with a small colored warning icon: Row 1: ENDOMETRIAL POLYP • Focal hyperechoic endometrial thickening • Vascular pedicle on Doppler • Well-defined margins Row 2: FIBROID (SUBMUCOSAL) • Hypoechoic mass distorting endometrial echo • Well-defined edges, posterior shadowing if calcified Row 3: SIMPLE OVARIAN CYST • Thin-walled, anechoic, smooth • Posterior acoustic enhancement • >3 cm warrants follow-up Row 4: ENDOMETRIOMA • "Ground glass" - homogeneous low-level internal echoes • Thick wall, no internal flow on Doppler Row 5: ECTOPIC PREGNANCY • Adnexal ring sign outside uterus • Empty uterine cavity • Free fluid in POD (hemoperitoneum) Row 6: PCOS • ≥12 follicles per ovary, 2-9 mm (string of pearls) • Increased stromal echogenicity • Enlarged ovarian volume >10 mL Row 7: HYDROSALPINX • Tortuous anechoic tubular adnexal structure • Incomplete septa, no flow on Doppler Row 8: COMPLEX FREE FLUID (POD) • Echogenic or large volume = pathologic • Suggests blood, pus, or ascites At the bottom of the poster, a thin gray section shows a "ECHOGENICITY LEGEND" with colored squares: Black square = Anechoic (fluid), Light gray = Hyperechoic (bright), Medium gray = Isoechoic, Dark gray = Hypoechoic. Footer text: "TVS Quick Reference | Always correlate with clinical history and menstrual cycle phase" The overall design is clean, professional, medical-grade with good spacing, readable fonts, color-coded sections, and small anatomical diagram icons next to each section header. The poster is portrait orientation, approximately A3 size proportions.
real time tvs scan for better undertanding
transvaginal ultrasound real time scan video tutorial normal anatomy uterus ovary site:youtube.com
transvaginal sonography live scan demonstration educational video uterus endometrium ovary
sonographic anatomy uterus ovaries transvaginal real time annotated video SONO LEARNING OR Zedu OR ultrasoundpaedia
transvaginal ultrasound GIF animated scan uterus ovary real time image series
https://ultrasoundpaedia.com/uterus-normal
Real-Time TVS Scan - Frame-by-Frame Walkthrough
Important note: I can't embed live video here, but I've compiled the best real-time video resources + a detailed frame-by-frame simulation with real sonographic images below. Watch the videos alongside this guide for maximum learning.
Best Free Real-Time TVS Video Resources
| Video | Channel | What it covers |
|---|---|---|
| Real-Time TVS - Normal Anatomy | YouTube | Live probe insertion to final images |
| How to Perform TVS (Technique) | SONO Learning | Step-by-step probe movements |
| TVS - How to Find the Ovaries | Zedu Ultrasound | The hardest part - ovary localization |
| POCUS TVS Scanning Sequence | POCUS Training | Full systematic sequence |
| Annotated Gynae US Anatomy | Dr Sam's Imaging Library | Labeled real-time images |
| TVS Exam Part 1 | Sonosite | Fundals, endometrium, adnexa |
| TVS Exam Part 2 | Zedu/Coaching Corner | Endometrium + adnexa deep dive |
Real-Time Scan Simulation - Frame by Frame
FRAME 1 - Probe Insertion and First Image

- (a) Probe enters vaginal canal with indicator at 12 o'clock - red arrow shows direction of beam
- (b) Probe rotated 90° (green arrow) for transverse view
- (c) First sagittal TVS image - label: ENDOMETRIUM visible centrally. ANT = anterior, POST = posterior. The bright central stripe is the endometrium. Red arrow = probe artifact at screen bottom
- (d) Transverse view - RT = right, LT = left. Red arrow = probe shadow
- The first thing you see when inserting the probe is the probe itself (bright artifact at the near field/top of image)
- The uterus "falls into view" as a gray pear-shaped structure
- Fan left-right to center the endometrial stripe
FRAME 2 - Sagittal Uterus (The Establishing Shot)
SCREEN LAYOUT - SAGITTAL TVS:
┌─────────────────────────────────────┐
│ PROBE ARTIFACT (near field, top) │
│─────────────────────────────────────│
│ ┌──────────┐ │
│ BLADDER│ (black) │ │
│ └────┬─────┘ │
│ ┌────▼──────────────┐ │
│ │ UTERINE FUNDUS │ │
│ │ ┌─────────────┐ │ │
│MYOMETRIUM│ │ENDOMETRIUM │ │ │
│(gray) │ │ (bright) │ │ │
│ │ └─────────────┘ │ │
│ │ CERVIX │ │
│ └───────────────────┘ │
│ POUCH OF DOUGLAS (posterior) │
│ RECTUM (posterior) │
│─────────────────────────────────────│
│ LEFT = cephalad | RIGHT = caudal │
└─────────────────────────────────────┘
- Fan the probe toward you (handle down) → see the fundus and upper uterus
- Fan away from you (handle up) → see the cervix and lower uterine segment
- The endometrial stripe follows the uterine axis as you sweep
FRAME 3 - Endometrial Stripe Close-Up
| Phase | Live appearance |
|---|---|
| Menstrual | Thin echogenic line, sometimes broken - minimal tissue |
| Early proliferative | Single thin bright line 3-6 mm - "pencil line" |
| Late proliferative | Triple line - two bright outer lines flanking a dark zone (the most recognized appearance) |
| Secretory | Thick, uniformly bright/echogenic - "solid white slab" |
| Postmenopausal | Thin, barely visible bright line ≤4-5 mm |
FRAME 4 - Rotating to Transverse (The "Owl Face")
SCREEN LAYOUT - TRANSVERSE UTERUS:
┌─────────────────────────────────────┐
│ LEFT of screen = patient's RIGHT │
│─────────────────────────────────────│
│ │
│ ╭──────────────────╮ │
│ │ ● ENDO ● │ ← cornua │
│ │ (bright) │ │
│ ╰──────────────────╯ │
│ MYOMETRIUM (gray rim) │
│ │
│─────────────────────────────────────│
│ Fan UP = fundus | Fan DOWN = cervix│
└─────────────────────────────────────┘
FRAME 5 - Cervix View
SCREEN LAYOUT - CERVICAL SAGITTAL:
┌─────────────────────────────────────┐
│ ┌──────────────┐ │
│ │ UTERINE │ │
│ │ BODY │ │
│ └──────┬───────┘ │
│ │ internal os │
│ ┌──────▼───────┐ │
│ │ CERVIX │←─ fibrous, │
│ │ ─────────── │ intermediate │
│ │ endo canal │ echogenicity │
│ └──────┬───────┘ │
│ │ external os │
│ POSTERIOR FORNIX / VAGINA │
│ │
│ RECTUM posterior to cervix │
└─────────────────────────────────────┘
- The endocervical canal = bright central line within the cervix
- The internal os = where the cervical canal opens into the uterine cavity
- The external os = V-shaped notch at the bottom of the cervix
- Nabothian cysts = small black dots (anechoic) scattered in cervical stroma - benign, ignore
FRAME 6 - Sweeping to Find the Right Ovary
- Rock the probe handle toward the patient's LEFT (which angles the beam to the patient's RIGHT)
- Follow the ovarian ligament as it extends laterally
- Look for the internal iliac vein - a large, oval, anechoic (black) tubular structure near the pelvic sidewall
- The ovary sits just medial to this vessel
PELVIC SIDEWALL ANATOMY (what you see scanning laterally):
←── UTERUS ──── OVARY ──── ILIAC VESSELS ──── PELVIC WALL ──→
(find (your landmark -
this!) find these first)
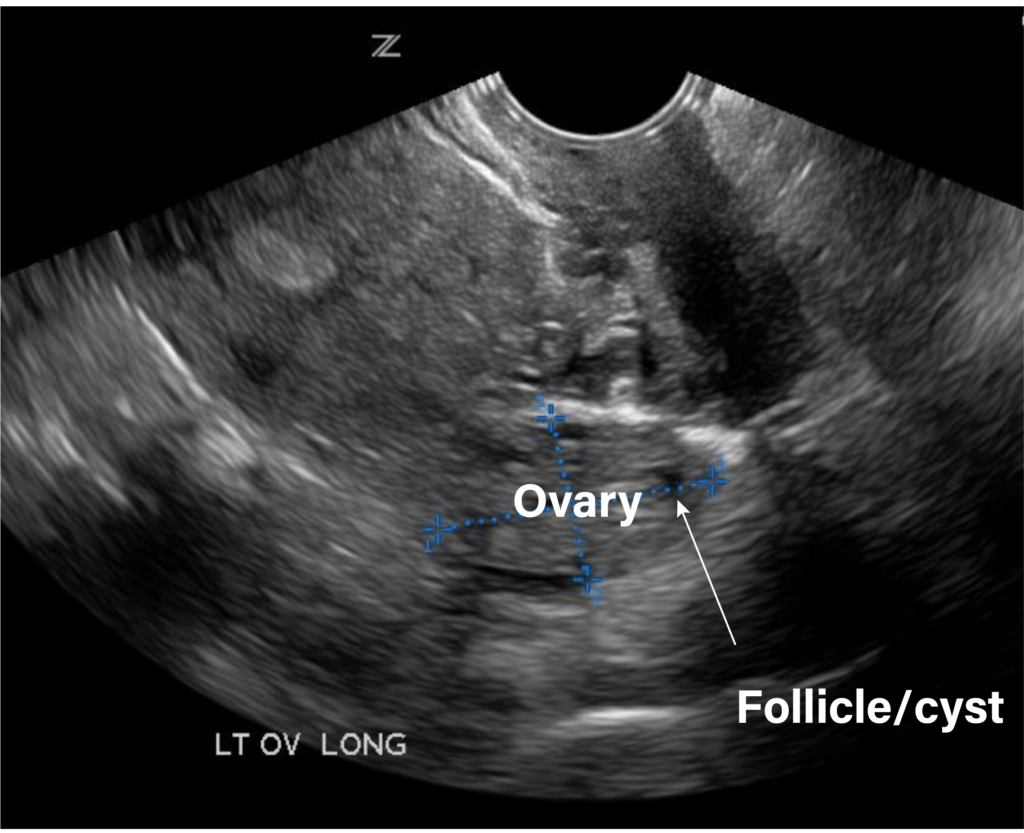
FRAME 7 - Normal Ovary on Screen
- Oval, homogeneous structure with a slightly darker (hypoechoic) texture than myometrium
- Follicles = small round black (anechoic) dots within the ovary - these are the antral follicles
- Dominant follicle = one large anechoic bubble, up to ~20-25 mm, thin-walled
- Calipers (the dotted blue measurement lines) to measure 3 dimensions: length × width × height
- Ovarian volume = L × W × H × 0.523 (prolate ellipsoid formula)
- Reproductive age: 5-15 mL
- Postmenopausal: < 3 mL
FRAME 8 - Pouch of Douglas Check
POSTERIOR CUL-DE-SAC / POUCH OF DOUGLAS:
UTERUS ──► posterior wall
↓
┌──────────────┐
│ POD space │ ← normal: small anechoic sliver of fluid
└──────────────┘ ← abnormal: large black pool, complex echoes
↓
RECTUM/BOWEL
| What you see | Meaning |
|---|---|
| No fluid | Normal (especially follicular phase) |
| Small thin sliver of anechoic fluid | Normal physiologic fluid (luteal phase/ovulation) |
| Large pool of anechoic fluid | Pathologic - ascites, ruptured cyst |
| Echogenic/complex fluid | Blood (ectopic), pus (PID/TOA), endometriosis |
Real-Time Scanning Sequence Summary (Checklist)
TVS SCAN SEQUENCE
─────────────────────────────────────────
① INSERT probe, indicator 12 o'clock
→ Sagittal uterus: identify & measure
→ Endometrial stripe measurement
→ Cervix: canal, os, nabothian cysts
② ROTATE 90° CCW → indicator 9 o'clock
→ Transverse uterus: fundus to cervix
→ "Owl face" at fundal level
③ ROCK HANDLE LEFT
→ Find right ovary (near R iliac vein)
→ Measure in 3 planes
④ ROCK HANDLE RIGHT
→ Find left ovary (near L iliac vein)
→ Measure in 3 planes
⑤ RETURN to sagittal midline
→ Pouch of Douglas: fluid assessment
→ Adnexa: tubes, masses
─────────────────────────────────────────
Total scan time: ~8-15 minutes
What NOT to Miss in Real Time
| If you see this... | Think... |
|---|---|
| Empty uterus + adnexal ring | Ectopic pregnancy until proven otherwise |
| Thick endometrium postmenopause (>5 mm) | Endometrial hyperplasia/carcinoma - refer |
| "Ground glass" ovarian cyst | Endometrioma |
| "String of pearls" - 12+ small follicles | PCOS |
| Free echogenic fluid in POD | Hemoperitoneum - urgent |
| Dilated tortuous tubular structure adnexa | Hydrosalpinx |
| Thick-walled cyst with "ring of fire" on Doppler | Corpus luteum (normal) or ectopic (correlate!) |