Explain me 10 heart disease with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Searching the Web
ECG changes 10 heart diseases electrocardiogram patterns STEMI atrial fibrillation heart block
Finding Sources
Reading Web Page
https://mesimedical.com/insights/frequently-diagnosed-condit…
Finding Sources
Searching the Web
ECG images STEMI atrial fibrillation complete heart block WPW hypertrophic cardiomyopathy pericarditis
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Searching the Web
ECG images atrial fibrillation complete heart block Brugada syndrome long QT Wolff-Parkinson-White pulmonary embolism
Finding Sources
Searching the Web
site:wikimedia.org OR site:ecgwaves.com ECG atrial fibrillation complete heart block ventricular tachycardia pulmonary embolism S1Q3T3
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Searching the Web
ECG images atrial fibrillation ventricular fibrillation complete heart block long QT Brugada hypertrophic cardiomyopathy site:ecgwaves.com OR site:litfl.com
Loading Image
Here is a thorough guide to 10 heart diseases with their ECG changes and ECG images sourced from authoritative medical textbooks and literature.
10 Heart Diseases with ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Disease: Complete occlusion of a coronary artery causes transmural (full-thickness) ischemia and necrosis of the myocardium.
ECG Changes:
- Hyperacute T waves - tall, broad, symmetric T waves are the earliest finding (minutes)
- ST-segment elevation - ≥1 mm in ≥2 contiguous leads (≥2 mm in V2-V3 for men, ≥1.5 mm in women)
- Reciprocal ST depression - in leads facing away from the infarct zone
- Pathological Q waves - develop within hours as necrosis sets in (≥40 ms wide, ≥25% of R wave height)
- T wave inversion - develops as the infarct evolves
- Localization: anterior STEMI (V1-V4), inferior STEMI (II, III, aVF), lateral STEMI (I, aVL, V5-V6)
ECG - Anterior Wall STEMI (V1-V4 elevation):
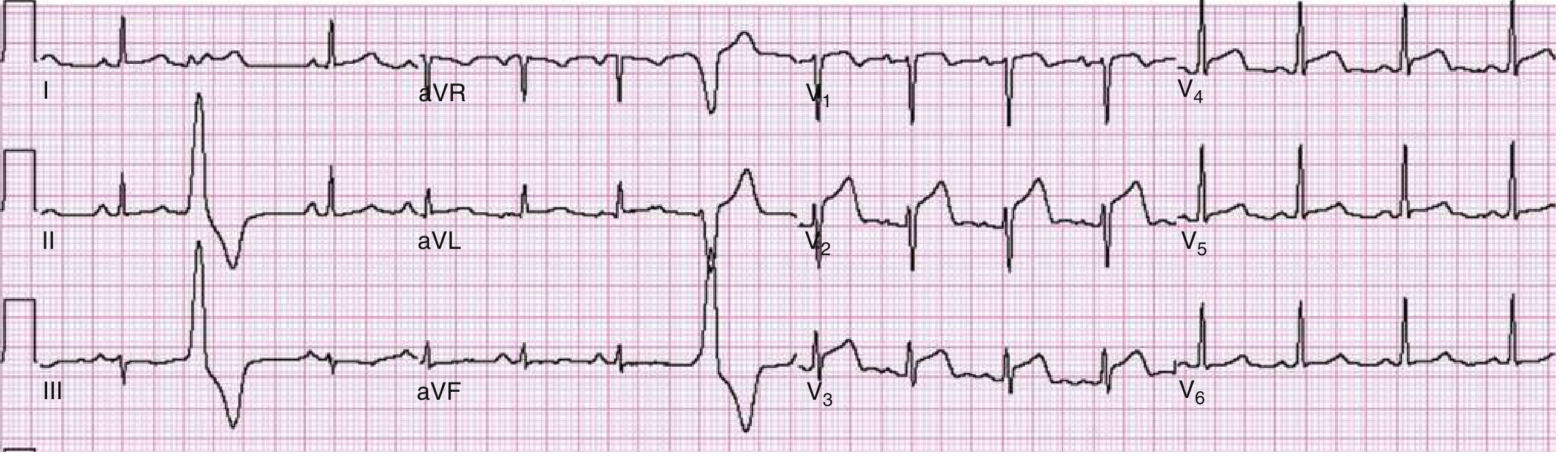
Anterior wall STEMI: ST-segment elevation evident in leads V1 to V4 with obliquely straight morphology. Catheterization revealed 90% stenosis of the LAD artery. (ROSEN's Emergency Medicine)
ECG - Anterolateral STEMI (V2-V6, I, aVL):
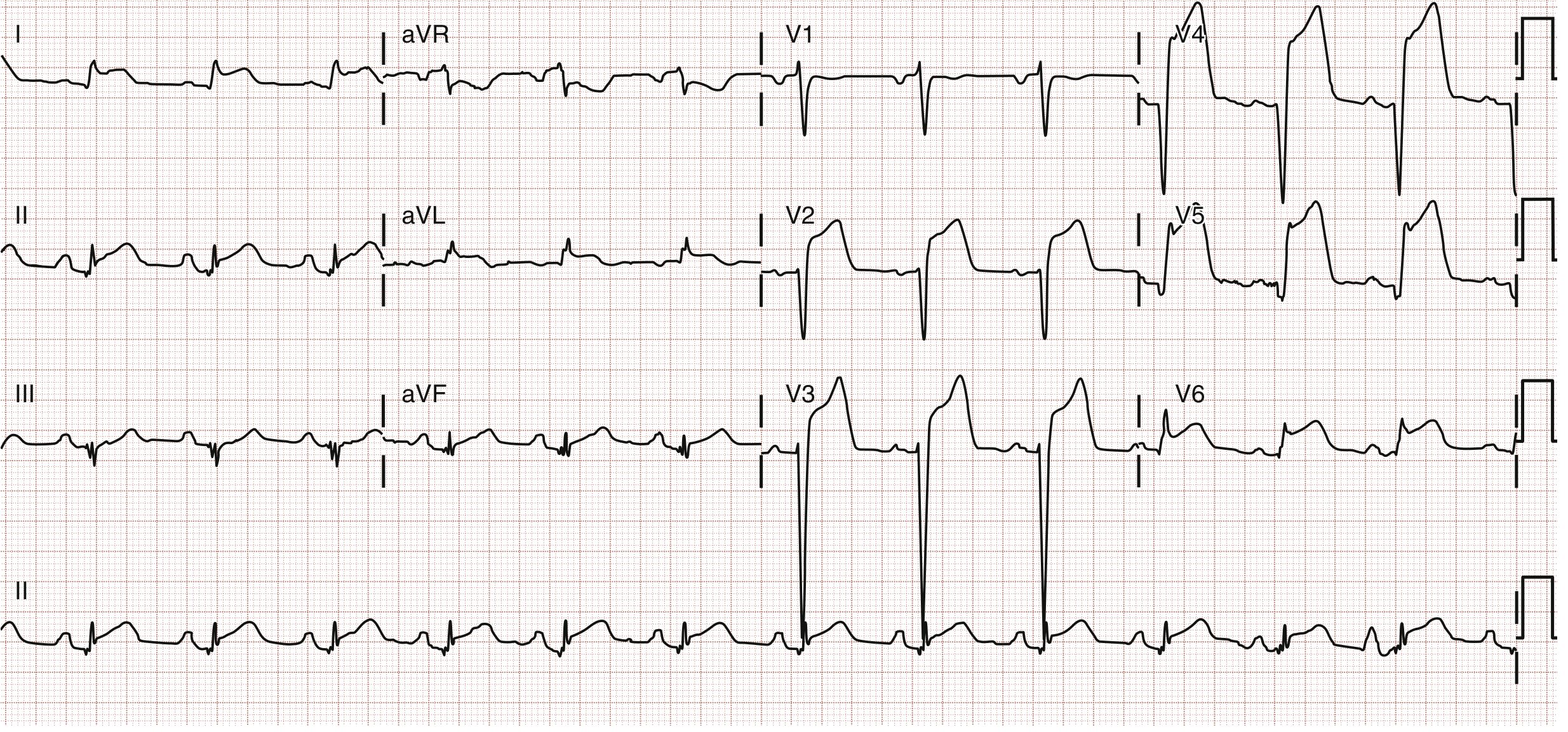
Anterolateral STEMI: STE in leads V2-V6, I, and aVL. Patient had prior LAD stent with 100% in-stent thrombosis on emergency catheterization. (ROSEN's Emergency Medicine)
ECG - Left Main / aVR STEMI:
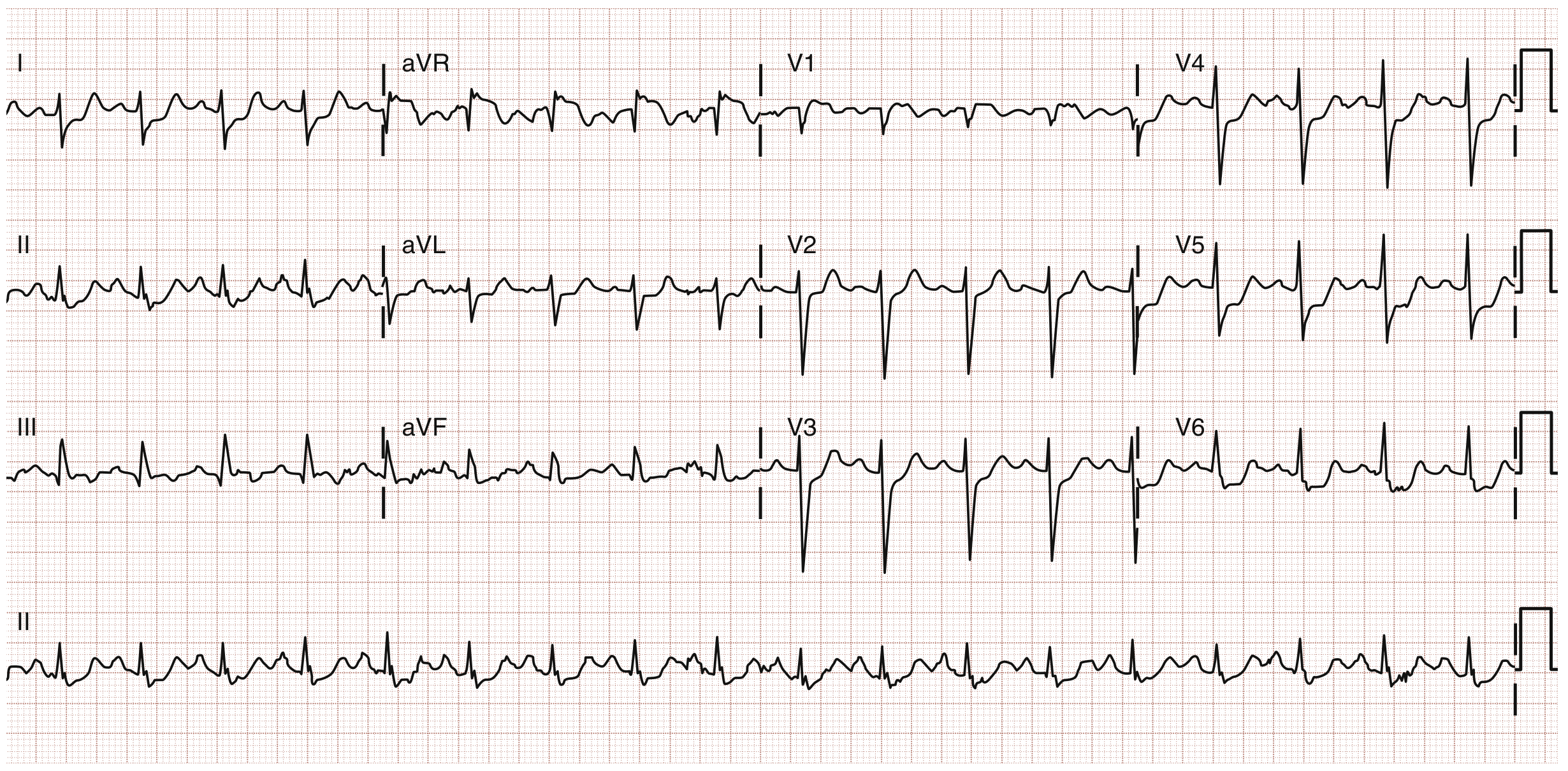
ST elevation in lead aVR with widespread ST depression - classic for left main coronary artery occlusion or severe multivessel disease. (ROSEN's Emergency Medicine)
2. Acute Pericarditis
Disease: Inflammation of the pericardial sac, most commonly viral in origin (Coxsackie B, echovirus). Presents with sharp pleuritic chest pain that improves leaning forward.
ECG Changes (4 Stages):
- Stage 1 (hours to days): Diffuse ST elevation (concave/saddle-shaped) in most leads (I, II, III, aVF, V2-V6) + PR segment depression (most evident in II and V6). aVR shows reciprocal ST depression and PR elevation.
- Stage 2 (days): ST and PR segments normalize
- Stage 3 (1-3 weeks): Diffuse T wave inversions
- Stage 4 (weeks-months): ECG returns to baseline
Key distinguishing features from STEMI: diffuse (not territorial) ST elevation, PR depression, absence of reciprocal ST depression (except aVR/V1), concave morphology, no Q waves.
ECG - Acute Pericarditis (Stage I):
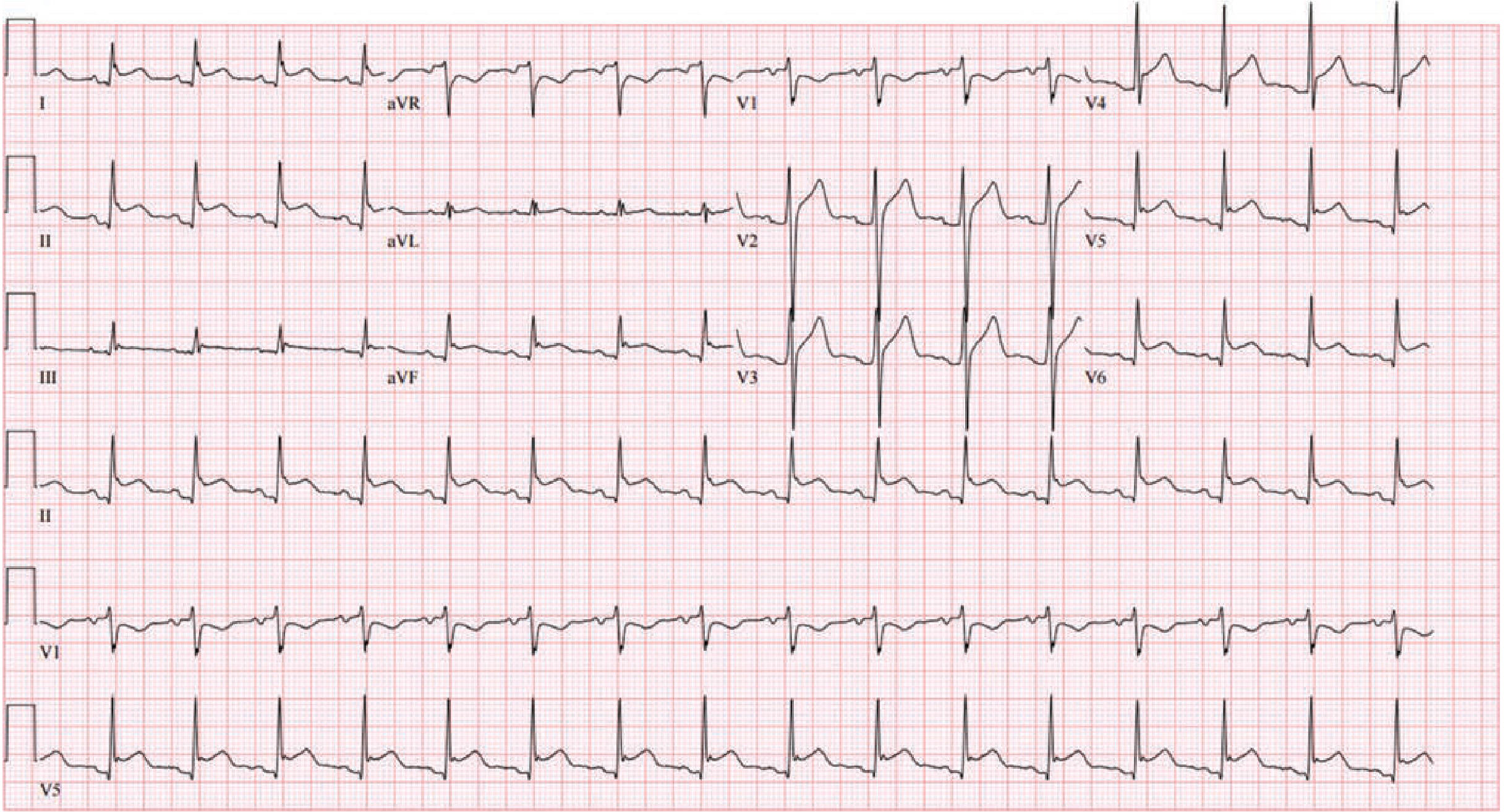
Stage I pericarditis: Diffuse ST-segment elevation with concordant PR-segment depression in a non-territory-specific distribution. aVR shows simultaneous ST depression with PR elevation. (Fuster and Hurst's The Heart, 15th Edition)
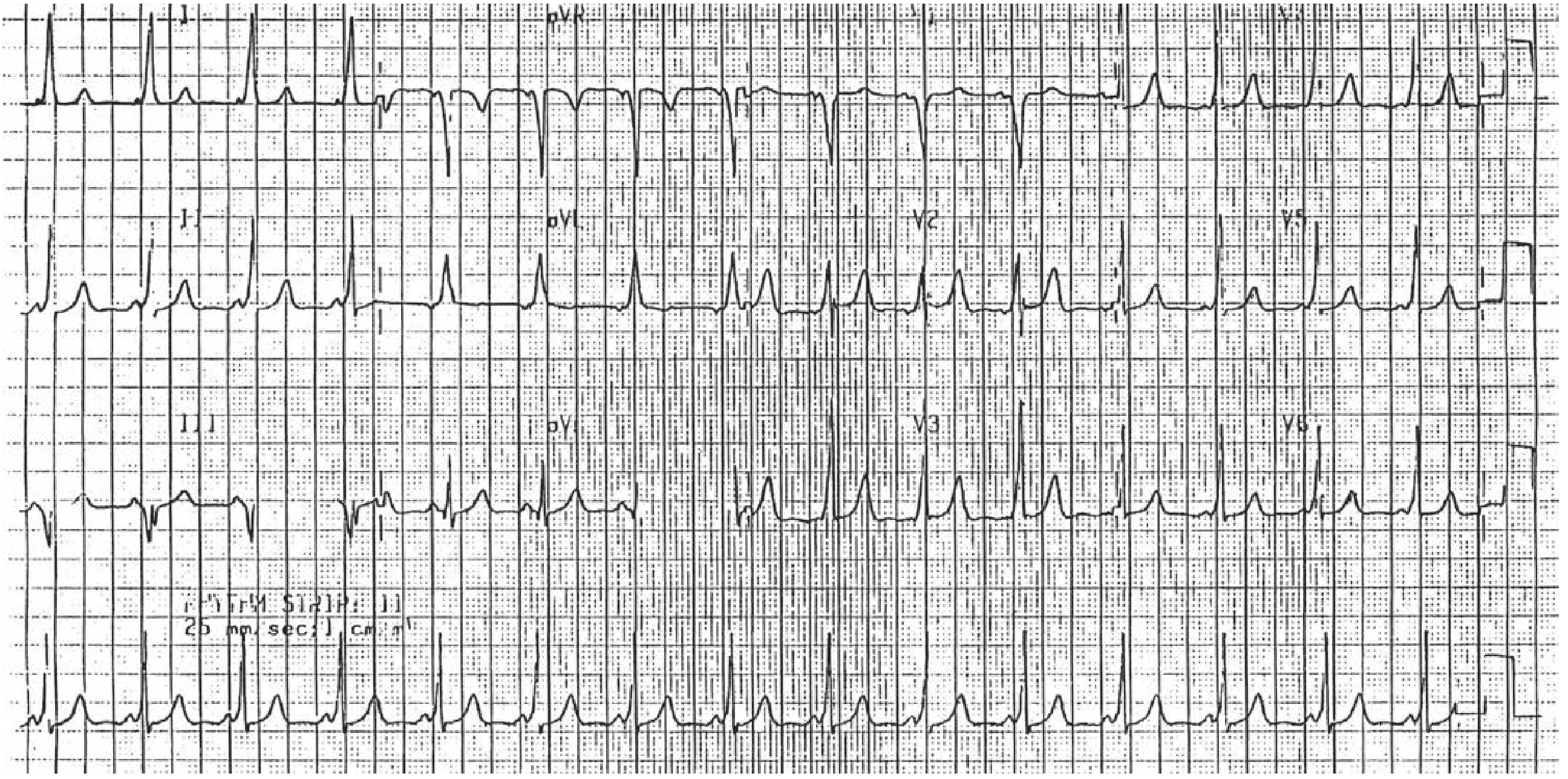
3. Atrial Fibrillation (AF)
Disease: Chaotic, disorganized electrical activity in the atria. Most common sustained cardiac arrhythmia. Associated with hypertension, valvular disease, heart failure, hyperthyroidism, and alcohol.
ECG Changes:
- Absent P waves - replaced by irregular fibrillatory (f) waves (best seen in V1 and II), rate 350-600/min
- Irregularly irregular RR intervals - hallmark finding
- Variable QRS morphology due to aberrant conduction
- Atrial rate 350-600/min, ventricular rate typically 100-180/min (uncontrolled)
- QRS complexes are narrow unless aberrant conduction or pre-existing bundle branch block present
Key ECG Pattern: No discernible P waves + chaotic baseline + irregular rhythm = AF until proven otherwise.
(Textbook source: Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine 22E)
4. Complete (Third-Degree) AV Heart Block
Disease: Complete interruption of conduction between atria and ventricles. The atria and ventricles beat independently. Causes include ischemia (especially inferior MI - RCA occlusion), fibrosis/sclerosis, myocarditis, drugs.
ECG Changes:
- AV dissociation - P waves and QRS complexes bear no relationship to each other
- Atrial rate > Ventricular rate (atrial rate ~60-100/min, ventricular escape rate 20-40/min)
- Regular P-P intervals and regular R-R intervals - but they march independently
- Escape rhythm: Narrow QRS if block is in the AV node (junctional escape, rate 40-60/min); Wide QRS if block is in the His-Purkinje system (ventricular escape, rate 20-40/min, less reliable)
- The PR interval varies completely - there is no consistent PR relationship
(Source: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine)
5. Wolff-Parkinson-White (WPW) Syndrome
Disease: Accessory bypass tract (Bundle of Kent) connects atria to ventricles, bypassing the AV node. Allows antegrade pre-excitation of the ventricles. Presents with SVT, palpitations, and risk of sudden death if AF develops.
ECG Triad During Sinus Rhythm:
- Short PR interval (<120 ms) - due to rapid conduction via accessory pathway
- Delta wave - slurred upstroke of the QRS complex (pre-excitation of part of the ventricle)
- Widened QRS complex (>120 ms) - fusion of normal conduction + pre-excitation
- Pseudo-ST and T wave changes (secondary repolarization abnormalities)
During AF with WPW: Wide, bizarre, irregular QRS complexes with delta waves at rates >200 bpm - a life-threatening emergency. AV-blocking drugs (adenosine, beta-blockers, CCBs, digoxin) are contraindicated.
ECG - WPW (Short PR + Delta Waves):
WPW syndrome: Short PR interval and widened QRS with delta waves (slurred initial QRS upstroke). (Tintinalli's Emergency Medicine)
6. Brugada Syndrome
Disease: Inherited sodium channelopathy (SCN5A mutation in ~25% of cases). Causes ventricular fibrillation at rest/sleep in structurally normal hearts. Predominantly affects young Asian males. Associated with sudden unexplained nocturnal death syndrome (SUNDS).
ECG Changes:
- Type 1 (Coved pattern) - diagnostic: ≥2 mm coved-type ST elevation (downsloping) followed by a negative T wave in ≥1 of V1-V2. This is the only pattern diagnostic of Brugada.
- Type 2 (Saddle-back pattern): ≥2 mm ST elevation with a saddle-back morphology and a positive T wave - this is not diagnostic alone
- Best seen with leads placed at 2nd-3rd intercostal space
- ECG may be dynamic - can be unmasked/exaggerated by fever, sodium channel blockers (ajmaline, flecainide), cocaine
- Sinus bradycardia, first-degree AV block, and RBBB pattern also common
(Source: Braunwald's Heart Disease 2-Vol Set; Fuster and Hurst's The Heart 15th Edition)
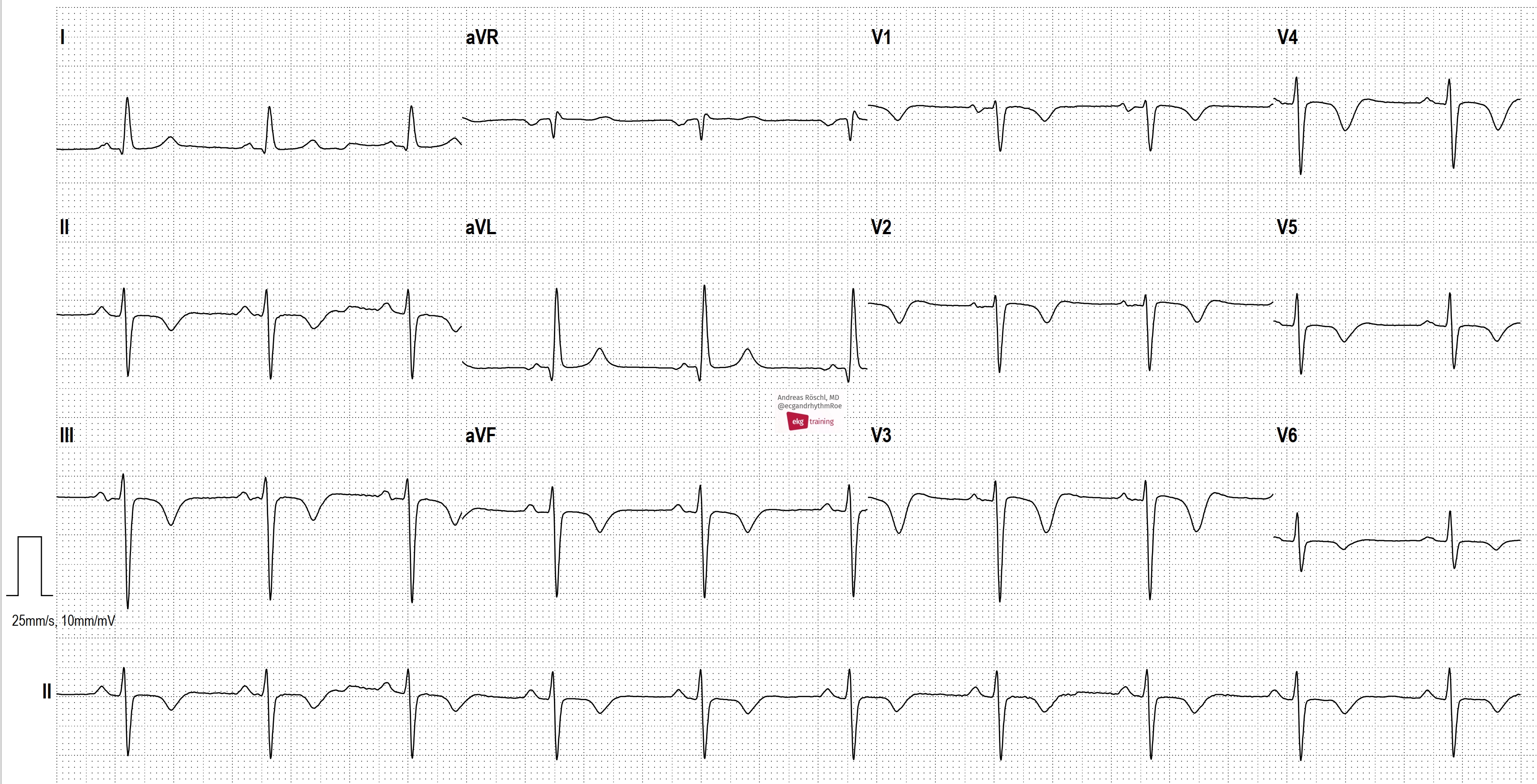
7. Hypertrophic Cardiomyopathy (HCM)
Disease: Genetic disorder of sarcomere proteins causing asymmetric left ventricular hypertrophy (usually the septum). Most common cause of sudden cardiac death in young athletes. Obstructive form (HOCM) causes dynamic LVOT obstruction.
ECG Changes (abnormal in >90% of patients):
- Left ventricular hypertrophy (LVH) criteria: Sokolow-Lyon (S in V1 + R in V5/V6 >35 mm); Cornell criteria
- Deep, narrow Q waves ("dagger" or "septal" Q waves) in lateral leads (I, aVL, V5-V6) and inferior leads - due to abnormal septal depolarization
- ST-segment depression and T wave inversions - especially in lateral leads
- Giant T wave inversions in apical HCM (Yamaguchi syndrome) - prominent in V3-V5
- Left axis deviation
- Left atrial enlargement (broad notched P waves in II, deep negative component in V1)
(Source: Tintinalli's Emergency Medicine; Goldman-Cecil Medicine)
8. Pulmonary Embolism (PE)
Disease: Thrombus obstructing the pulmonary vasculature causing acute right heart strain. Large PE causes sudden RV pressure overload, dilation, and ischemia.
ECG Changes (10-25% of patients have a normal ECG):
- Sinus tachycardia - most common finding (~40-50%)
- S1Q3T3 pattern (McGinn-White sign): Deep S wave in lead I + Q wave in lead III + inverted T wave in lead III - present in ~20%, indicates acute RV strain
- T wave inversions in V1-V4 - right precordial leads reflecting RV ischemia
- New right bundle branch block (RBBB) - complete or incomplete
- Right axis deviation
- P pulmonale (tall peaked P waves >2.5 mm in lead II)
- Atrial arrhythmias - AF, atrial flutter, atrial tachycardia
- ST elevation or depression in V1-V3
(Source: ROSEN's Emergency Medicine; ecgwaves.com; PMC4613926)
9. Long QT Syndrome (LQTS)
Disease: Inherited or acquired channelopathy causing delayed ventricular repolarization. Predisposes to Torsades de Pointes (TdP) - a polymorphic VT that can degenerate to VF and sudden death. Inherited types include LQT1 (KCNQ1), LQT2 (KCNH2/hERG), LQT3 (SCN5A). Acquired causes include QT-prolonging drugs (antiarrhythmics, antibiotics, antipsychotics), hypokalemia, hypomagnesemia.
ECG Changes:
- Prolonged QTc interval: ≥440 ms in men, ≥460 ms in women (Bazett's formula: QT/√RR)
- QTc >500 ms - high risk for TdP
- T wave abnormalities vary by subtype:
- LQT1: Broad-based T waves
- LQT2: Notched or bifid T waves
- LQT3: Long flat ST segment, late-peaking narrow T wave
- U waves may be prominent (especially in hypokalemia-associated LQTS)
- Torsades de Pointes: polymorphic VT with QRS complexes that rotate around the isoelectric line - "twisting of points" pattern
(Source: Tintinalli's Emergency Medicine - Long QT Syndrome section)
10. Ventricular Fibrillation (VF)
Disease: Chaotic, uncoordinated ventricular electrical activity with no effective cardiac output. A lethal arrhythmia causing cardiac arrest. Caused by severe ischemia/STEMI, electrolyte disturbances, drugs, channelopathies (LQT, Brugada), cardiomyopathies.
ECG Changes:
- Completely chaotic, irregular waveforms with no discernible P waves, QRS complexes, or T waves
- Irregular waveforms of varying shapes and amplitudes (erratic baseline)
- No identifiable cardiac cycles
- Coarse VF: larger amplitude fibrillatory waves - more likely to respond to defibrillation
- Fine VF: smaller amplitude waves - worse prognosis, may resemble asystole
- Heart rate cannot be measured
- Clinically: pulseless, unconscious patient
Immediate management: Unsynchronized electrical defibrillation (200 J biphasic), CPR, epinephrine, amiodarone per ACLS protocol.
(Source: Tintinalli's Emergency Medicine; Guyton and Hall Textbook of Medical Physiology)
Quick Reference Summary
| # | Disease | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation ≥1 mm in ≥2 contiguous leads + reciprocal changes |
| 2 | Pericarditis | Diffuse concave ST elevation + PR depression (no reciprocal ST↓) |
| 3 | Atrial Fibrillation | No P waves + irregularly irregular rhythm |
| 4 | Complete Heart Block | AV dissociation: P waves and QRS complexes independent |
| 5 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 6 | Brugada Syndrome | Type 1 coved ST elevation ≥2 mm in V1-V2 + negative T wave |
| 7 | Hypertrophic Cardiomyopathy | LVH + deep septal Q waves + ST depression/T inversion |
| 8 | Pulmonary Embolism | Sinus tachycardia + S1Q3T3 + T inversions V1-V4 + RBBB |
| 9 | Long QT Syndrome | QTc >440 ms (men) or >460 ms (women) ± Torsades de Pointes |
| 10 | Ventricular Fibrillation | Chaotic waveforms - no P, QRS, or T waves identifiable |
Sources: ROSEN's Emergency Medicine; Tintinalli's Emergency Medicine; Fuster & Hurst's The Heart (15th Ed.); Harrison's Principles of Internal Medicine (22E); Braunwald's Heart Disease; Goldman-Cecil Medicine; ecgwaves.com; PMC literature.
This is a shared conversation. Sign in to Orris to start your own chat.