Teach me ecg from basic to clinical with changes in it so it can help me to save life of patients in emergencies also attach example and clinical symptoms of emergencies
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Searching the Web
ECG emergency patterns STEMI arrhythmia hyperkalemia PE clinical interpretation 2024
Here is your complete ECG guide - from the very basics to life-saving emergency recognition - built from Goldman-Cecil Medicine, Costanzo Physiology, Morgan & Mikhail's Clinical Anesthesiology, Fuster and Hurst's The Heart, and Tintinalli's Emergency Medicine.
ECG: From Basics to Clinical Emergencies
PART 1 - THE ELECTRICAL FOUNDATION
How the Heart's Electricity Works
The heart generates its own electricity through specialized cells. Understanding this is the foundation of every ECG you will ever read.
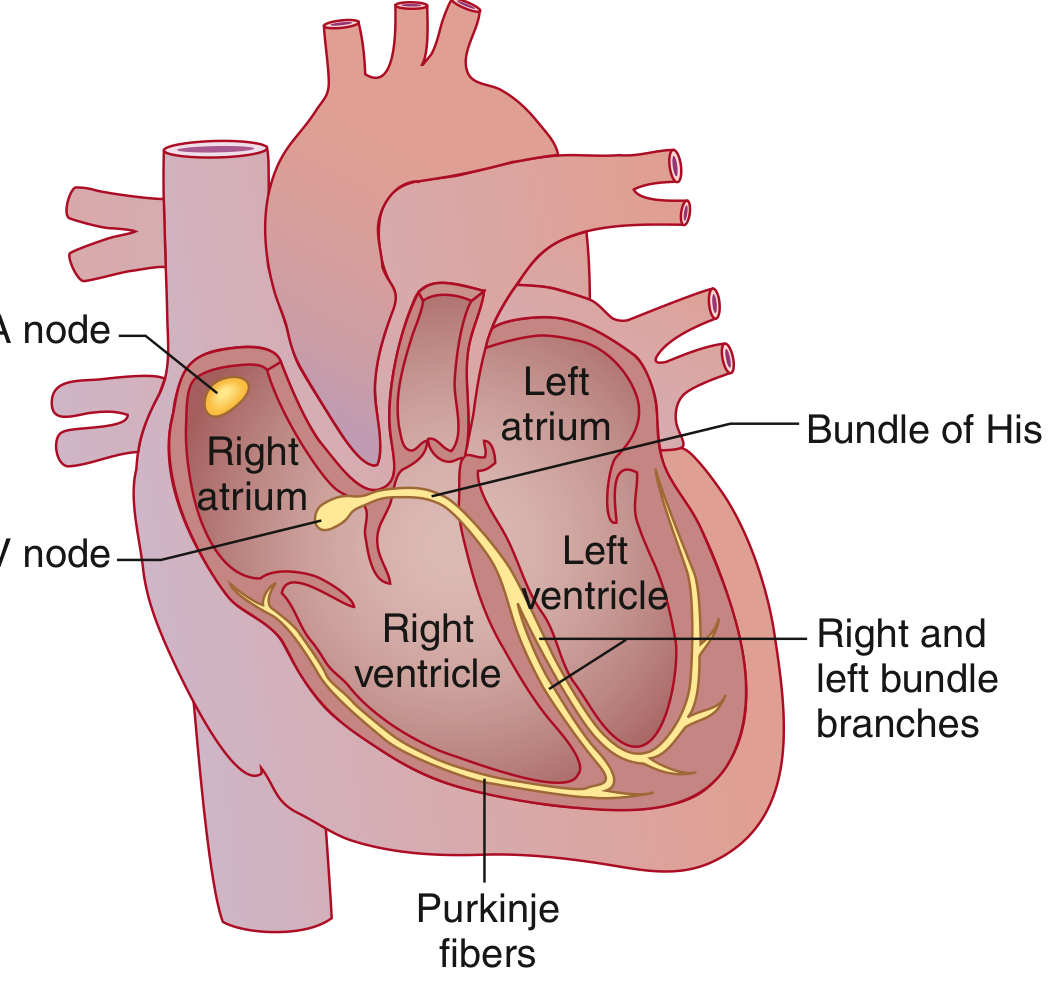
Goldman-Cecil Medicine - Cardiac conduction system: SA node (high right atrium) → Bachmann bundle → AV node → Bundle of His → Right and Left bundle branches → Purkinje fibers → ventricular muscle.
The sequence, in order:
| Step | Structure | ECG Result |
|---|---|---|
| 1 | SA node fires (60-100/min) | Triggers P wave |
| 2 | Atria depolarize | P wave on ECG |
| 3 | Delay at AV node (physiologic) | PR segment (flat line) |
| 4 | Spreads via Bundle of His + bundle branches + Purkinje | QRS complex |
| 5 | Ventricles repolarize | T wave |
Key rule: The AV node is the only electrical bridge between atria and ventricles. Anything blocking it = heart block.
PART 2 - ECG PAPER AND LEADS
ECG Paper - Reading the Grid

Costanzo Physiology, Fig 4.17 - The standard ECG from lead II showing all waves, intervals, and segments.
- Small box (1 mm) = 0.04 seconds (40 ms) in time | 0.1 mV in voltage
- Large box (5 mm) = 0.2 seconds (200 ms) | 0.5 mV
- Standard speed: 25 mm/sec
- Standard gain: 10 mm = 1 mV
The 12 Leads - What They "See"
Think of each lead as a camera angle looking at the heart from a different direction:
| Lead Group | Leads | Territory They Watch |
|---|---|---|
| Inferior | II, III, aVF | Bottom (inferior) wall - RCA territory |
| Lateral | I, aVL, V5, V6 | Left side - LCX territory |
| Anterior/Septal | V1, V2 | Septum - LAD territory |
| Anterior | V3, V4 | Anterior wall - LAD territory |
| Right-sided | aVR | Looks into the cavity - often inverted |
Memory aid for STEMI localization: Changes in those leads = occlusion in that artery.
PART 3 - THE WAVES, INTERVALS, AND SEGMENTS
P Wave
- Represents: Atrial depolarization (atria squeezing)
- Normal: Upright in lead II, biphasic in V1, duration < 0.12 sec, amplitude < 2.5 mm
- Abnormal:
- Absent P waves = atrial fibrillation, junctional rhythm, severe hyperkalemia
- Tall peaked P (> 2.5 mm in II) = P pulmonale (right atrial enlargement)
- Broad notched P = P mitrale (left atrial enlargement)
PR Interval
- Represents: Time from atrial depolarization to start of ventricular depolarization (includes AV node delay)
- Normal: 0.12-0.20 sec (3-5 small boxes)
- Short PR (< 0.12 sec): Pre-excitation (WPW syndrome) - accessory pathway bypasses AV node
- Long PR (> 0.20 sec): First-degree heart block - AV node conduction slowed
QRS Complex
- Represents: Ventricular depolarization
- Normal duration: 0.06-0.10 sec (< 3 small boxes)
- Normal morphology: Q wave < 0.04 sec wide and < 25% of R height
- Wide QRS (> 0.12 sec): Bundle branch block, ventricular rhythm, hyperkalemia, drug toxicity
Naming convention: If first deflection is DOWN = Q wave. Then UP = R wave. Then DOWN again = S wave.
ST Segment
- Represents: Early ventricular repolarization (ventricles in "plateau" phase)
- Normal: Isoelectric (flat, at baseline)
- ST Elevation: Injury (STEMI, pericarditis, Brugada, early repolarization)
- ST Depression: Ischemia (NSTEMI, demand ischemia), reciprocal changes
T Wave
- Represents: Ventricular repolarization
- Normal: Upright in most leads (I, II, V3-V6), may be inverted in aVR, V1
- Tall/peaked T: Hyperkalemia, hyperacute STEMI
- Inverted T: Ischemia, right heart strain (PE), bundle branch block, LVH
QT Interval
- Represents: Total ventricular depolarization + repolarization
- Normal corrected (QTc): < 440 ms (men), < 460 ms (women)
- Prolonged QTc: Risk of torsades de pointes (dangerous VT)
- Causes: Drugs (amiodarone, haloperidol, azithromycin, quinolones), hypokalemia, hypomagnesemia, congenital long QT
PART 4 - A SYSTEMATIC APPROACH (DO THIS EVERY TIME)
Use this 8-step method for every ECG:
1. RATE → Count R-R intervals. 300/large boxes between R waves.
Normal: 60-100. <60 = bradycardia. >100 = tachycardia.
2. RHYTHM → Regular or irregular? Is every QRS preceded by P wave?
Irregular = AF, multifocal AT, sinus arrhythmia
3. AXIS → Look at leads I and aVF:
Both upright = Normal axis
I up, aVF down = Left axis deviation (LAD, LBBB, inferior MI)
I down, aVF up = Right axis deviation (RVH, PE, lateral MI)
4. P WAVE → Present? Morphology normal? One P before each QRS?
5. PR INTERVAL → 0.12-0.20 sec? Consistent?
6. QRS → Width < 0.12 sec? Q waves? R progression in V1-V6?
7. ST SEGMENT → Elevation or depression? Which leads? How many mm?
8. T WAVE → Upright? Peaked? Inverted? Biphasic?
PART 5 - LIFE-THREATENING ECG EMERGENCIES
This section can save a life. Learn these patterns cold.
EMERGENCY 1 - STEMI (ST-Elevation Myocardial Infarction)
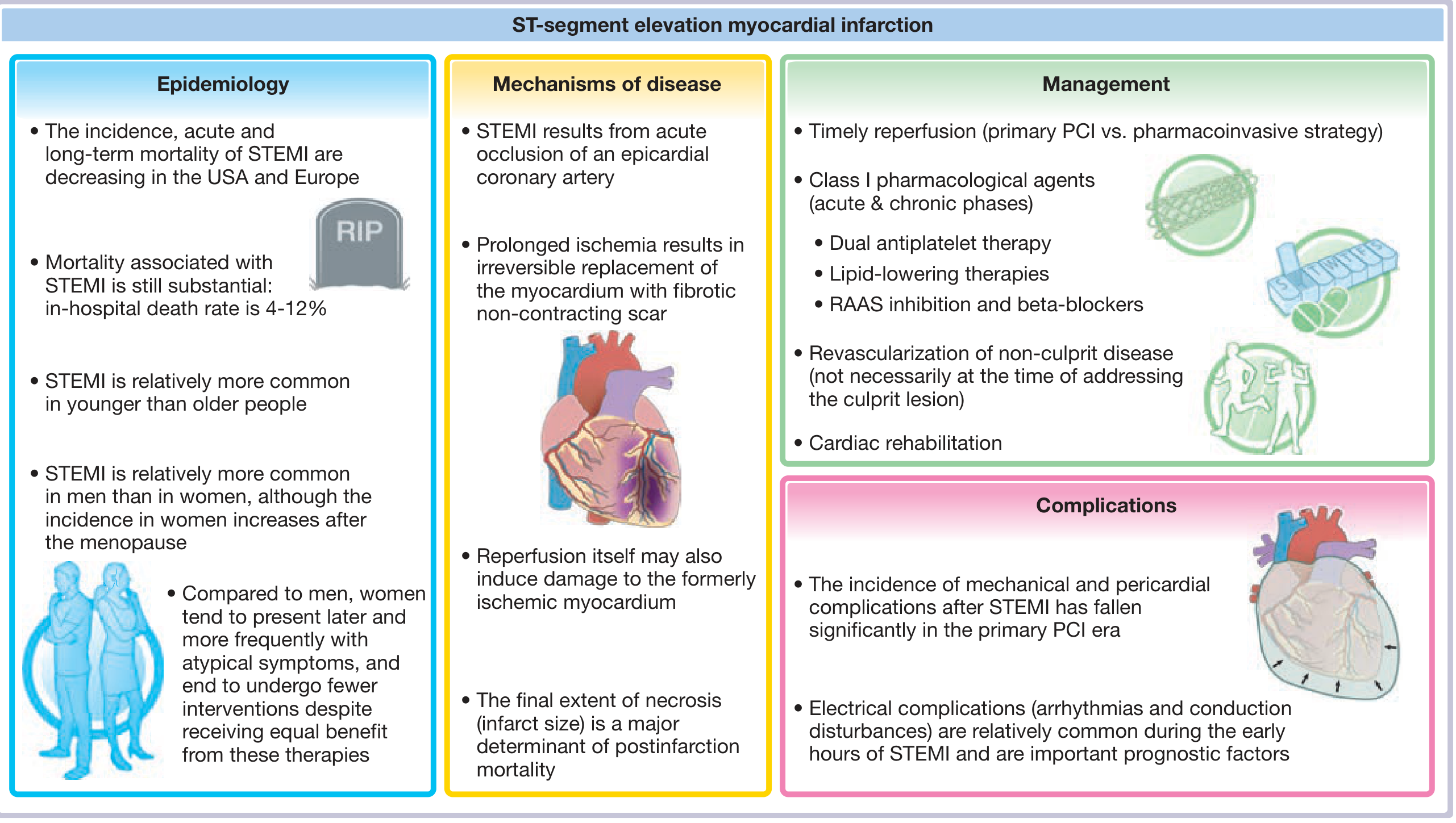
Fuster and Hurst's The Heart, 15th Ed - STEMI epidemiology, mechanism, management, complications.
What is happening: A coronary artery is completely blocked. Myocardium is dying right now. Every minute of delay = ~2 million dead cardiomyocytes.
ECG Changes (in order of evolution):
| Timeframe | ECG Finding |
|---|---|
| Minutes (hyperacute) | Tall, broad, peaked "hyperacute" T waves |
| 30 min - hours | ST elevation (tombstone pattern in severe cases) |
| Hours | Pathologic Q waves develop (dead tissue) |
| Days | ST normalizes; T waves invert |
| Weeks-months | Persistent Q waves (scar); T waves normalize by ~1 year |
STEMI Diagnosis Criteria:
- ST elevation in 2 or more contiguous leads:
- ≥ 2 mm in V1-V4 (anterior leads)
- ≥ 1 mm in limb leads (inferior or lateral)
Localization (which artery is blocked):
| ECG Leads Showing Changes | Wall | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| V1-V2 | Septal | LAD (proximal) |
| I, aVL, V5-V6 | Lateral | LCX |
| II, III, aVF | Inferior | RCA (usually) |
| Inferior + posterior (tall R/ST depression V1-V2) | Inferior + posterior | RCA |
Clinical Presentation:
- Crushing, pressure-like chest pain radiating to left arm/jaw (may be absent in diabetics, elderly, women)
- Diaphoresis (cold sweating)
- Nausea, vomiting
- Dyspnea, sense of impending doom
- In women: atypical - fatigue, jaw pain, nausea without chest pain
What to Do - STEMI Protocol:
- Give aspirin 325 mg immediately (chewed)
- Call for primary PCI (cath lab activation) - target door-to-balloon < 90 minutes
- If PCI unavailable within 120 min: give thrombolytics (tPA, streptokinase)
- Dual antiplatelet (add P2Y12 inhibitor: clopidogrel, ticagrelor, prasugrel)
- Anticoagulation (heparin)
- Beta-blocker + nitrates for pain (avoid nitrates if inferior STEMI + hypotension - could be RV infarct)
STEMI Equivalent alert: The De Winter pattern (upsloping ST depression V1-V6 + tall symmetric T + ST elevation in aVR) = proximal LAD occlusion WITHOUT classic ST elevation. Treat as STEMI.
EMERGENCY 2 - Ventricular Fibrillation (VF) / Pulseless Ventricular Tachycardia (pVT)
What is happening: Chaotic, disorganized ventricular electrical activity. No effective cardiac output. Patient is dead without immediate action.
ECG Pattern:
- VF: Completely chaotic, irregular, varying amplitude waveforms - no recognizable QRS complexes whatsoever
- VT (Ventricular Tachycardia): Wide QRS (> 0.12 sec), rate 100-250 bpm, regular, often with AV dissociation (P waves "march through" independently)
Clinical Presentation:
- Sudden collapse, unresponsive
- No pulse (check femoral or carotid)
- No breathing or gasping only
- Can be preceded by: palpitations, dizziness, syncope, chest pain
What to Do - VF/pVT Protocol:
- CALL CODE, start CPR immediately
- Defibrillate as fast as possible - every minute without defibrillation reduces survival by 7-10%
- Continue CPR immediately after shock (2 min cycles)
- IV/IO access - Adrenaline (epinephrine) 1 mg IV every 3-5 min
- Amiodarone 300 mg IV for refractory VF (after 2nd or 3rd shock)
- Address reversible causes (4 H's and 4 T's)
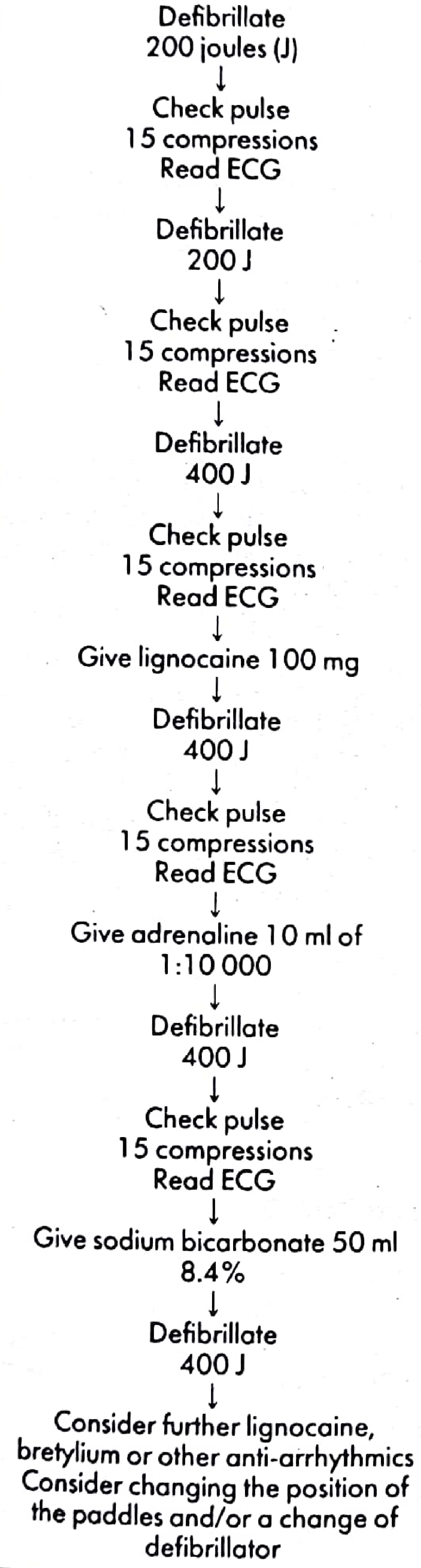
Pye's Surgical Handbook - VF management flowchart: escalating defibrillation 200J → 200J → 400J + adrenaline + sodium bicarbonate.
The 4 H's and 4 T's (reversible causes of cardiac arrest):
| 4 H's | 4 T's |
|---|---|
| Hypoxia | Tension pneumothorax |
| Hypovolemia | Tamponade (cardiac) |
| Hypo/Hyperkalemia | Toxins/drugs |
| Hypothermia | Thrombosis (PE or MI) |
EMERGENCY 3 - Complete (Third-Degree) Heart Block
What is happening: No electrical impulse gets from atria to ventricles. Atria and ventricles beat independently (AV dissociation). Ventricles fire on their own at a very slow escape rate.
ECG Pattern:
- P waves present at normal rate (~75 bpm)
- QRS complexes present but at slow rate (~30-40 bpm)
- No relationship between P waves and QRS - they "march through" each other
- QRS may be wide (ventricular escape) or narrow (junctional escape)
Clinical Presentation:
- Syncope (Stokes-Adams attacks)
- Severe bradycardia
- Dizziness, pre-syncope
- Hypotension, heart failure
- Can present with cardiac arrest
What to Do:
- Transcutaneous pacing immediately if hemodynamically unstable
- Atropine 0.5-1 mg IV (may not work in complete block - try anyway)
- Dopamine or adrenaline infusion as bridge
- Definitive: Permanent pacemaker insertion
Second-degree blocks:
- Mobitz I (Wenckebach): Progressive PR lengthening until a beat is dropped. Usually benign, nodal level.
- Mobitz II: Constant PR, sudden dropped beat without warning. More dangerous - can progress to complete block. Often needs pacing.
EMERGENCY 4 - Hyperkalemia ECG Changes
What is happening: High potassium reduces the resting membrane potential, making the heart unstable. Can progress to fatal arrhythmias.
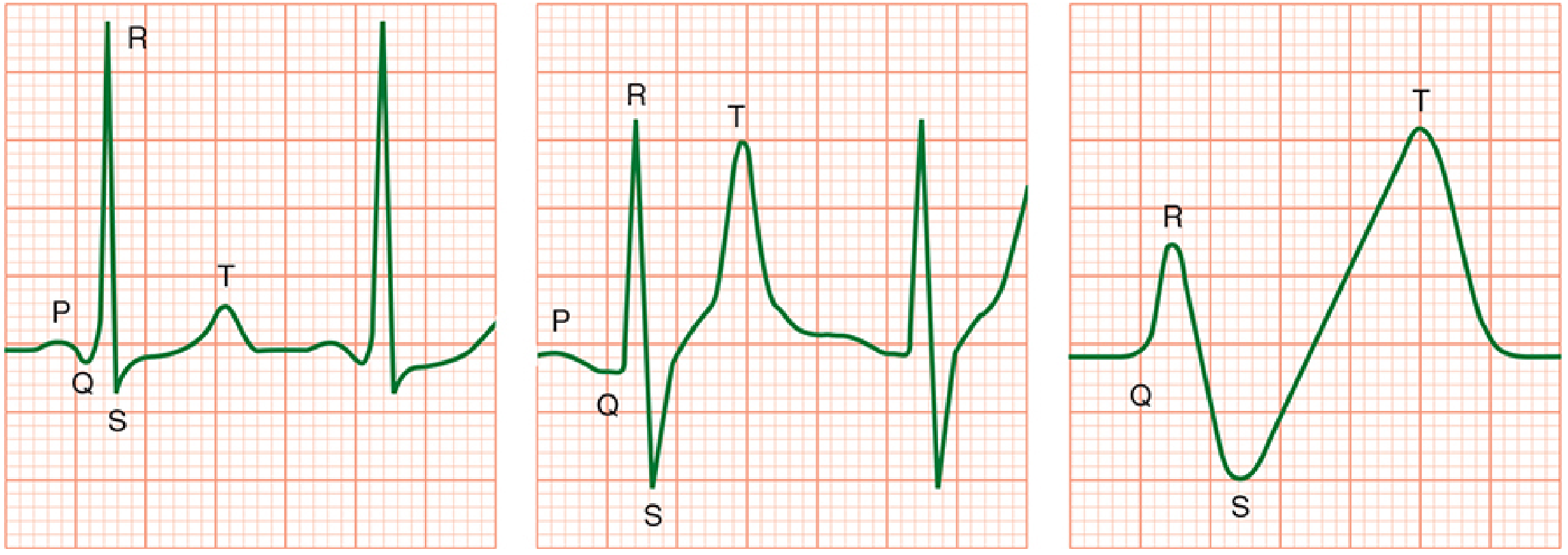
Morgan & Mikhail's Clinical Anesthesiology - Progression of hyperkalemia ECG changes: (Left) normal; (Middle) peaked T waves + wide QRS; (Right) sine wave pattern = imminent arrest.
ECG Changes in Order of Severity (Harrison's Principles):
| Potassium Level | ECG Change |
|---|---|
| 5.5-6.5 mEq/L | Symmetrically peaked, narrow-based T waves |
| 6.5-7.5 mEq/L | Loss of P waves, prolonged PR |
| 7.0-8.0 mEq/L | Widened QRS complex |
| > 8.0 mEq/L | Sine wave pattern - imminent VF/asystole |
Clinical Presentation:
- Weakness, fatigue, muscle cramps
- Paralysis (ascending)
- Palpitations
- Often in: renal failure, diabetic ketoacidosis, Addison's disease, ACE inhibitor use, massive tissue destruction (rhabdomyolysis)
What to Do - Emergency Hyperkalemia:
- Calcium gluconate 10 mL of 10% IV (or calcium chloride 3-5 mL) - membrane stabilization, works in minutes
- Insulin 10 units + 50 mL 50% glucose IV - drives K into cells, peak effect ~1 hour
- Sodium bicarbonate 50 mL of 8.4% - drives K into cells (if acidotic)
- Salbutamol (albuterol) nebulizer - beta agonist drives K into cells
- Furosemide IV - eliminates K (if renal function present)
- Dialysis - definitive treatment in renal failure
Caution: Do NOT give calcium if patient is on digoxin - calcium potentiates digoxin toxicity and can trigger VF.
EMERGENCY 5 - Pulmonary Embolism (PE)
What is happening: Massive clot in pulmonary vasculature causes acute right heart strain - the right ventricle cannot pump against the blocked pulmonary tree.
ECG Pattern (classic but not always present):
- S1Q3T3: Deep S wave in lead I, Q wave and T inversion in lead III
- Sinus tachycardia (most common finding - present in ~90%)
- Right bundle branch block (RBBB): rSR' pattern in V1, S wave in V5-V6
- Right axis deviation
- T wave inversions in V1-V4 (right heart strain pattern)
- P pulmonale (tall peaked P in lead II)
Clinical Presentation:
- Sudden onset dyspnea (most common)
- Pleuritic chest pain
- Hemoptysis
- Tachycardia (HR > 100)
- Hypoxia (O2 sat drops)
- Syncope in massive PE
- Signs of DVT: unilateral leg swelling, calf tenderness
- Risk factors: immobility, recent surgery, cancer, OCP, prior DVT/PE
What to Do:
- High-flow O2
- IV heparin bolus + infusion (anticoagulation)
- If massive PE with hemodynamic collapse: systemic thrombolysis (tPA 100 mg over 2 hours) or surgical embolectomy
- CT pulmonary angiography (CTPA) to confirm - do not wait for imaging if patient crashing
EMERGENCY 6 - Atrial Fibrillation (AF) with Rapid Ventricular Rate
What is happening: Chaotic atrial electrical activity (350-600 impulses/min from multiple foci). AV node filters some through to ventricles irregularly.
ECG Pattern:
- Absent P waves (replaced by chaotic fibrillatory baseline, especially visible in V1)
- Irregularly irregular QRS rhythm (no two R-R intervals are the same)
- Narrow QRS (unless aberrant conduction or bundle branch block)
- Variable rate depending on AV node conduction
Clinical Presentation:
- Palpitations ("fluttering" or "irregular" heartbeat)
- Dyspnea
- Fatigue
- Dizziness, presyncope
- Risk of stroke (clot forms in left atrial appendage during AF)
- In rapid AF: hemodynamic instability, chest pain
What to Do:
- If unstable (hypotension, chest pain, altered consciousness): Synchronized DC cardioversion immediately (100-200 J)
- If stable: Rate control first - metoprolol IV, diltiazem IV, or digoxin (in heart failure)
- Anticoagulation (DOAC or warfarin) if AF > 48 hours to prevent stroke
- Rhythm control options: amiodarone, flecainide, electrical cardioversion
EMERGENCY 7 - Long QT / Torsades de Pointes
What is happening: Prolonged repolarization creates a window for the ventricle to be re-excited mid-repolarization, triggering a dangerous polymorphic VT called torsades.
ECG Pattern of Torsades:
- Polymorphic VT (QRS complexes twist around the baseline - "twisting of the points")
- Preceded by prolonged QTc on baseline ECG
- Often triggered by a "short-long-short" sequence (PVC followed by pause)
Common Causes of Long QT:
- Drugs: Amiodarone, sotalol, haloperidol, methadone, quinolones, macrolides, antifungals
- Electrolytes: Hypokalemia, hypomagnesemia, hypocalcemia
- Congenital: Romano-Ward syndrome, Jervell and Lange-Nielsen syndrome
- Cardiac: Bradycardia, myocarditis, hypothyroidism
What to Do:
- Magnesium sulfate 2g IV over 5 minutes (first-line, even if Mg level is normal)
- Overdrive pacing (to keep rate > 100 and shorten QT)
- Stop all QT-prolonging drugs
- Correct electrolytes (K > 4.5 mEq/L, Mg > 2 mEq/L)
- If degenerates to VF: defibrillate
PART 6 - QUICK REFERENCE EMERGENCY RECOGNITION TABLE
| If you see this on ECG | Think | Act Now |
|---|---|---|
| ST elevation ≥ 1-2 mm in 2+ contiguous leads | STEMI | Activate cath lab, aspirin, heparin |
| Chaotic no-QRS waveform, no pulse | Ventricular Fibrillation | Defibrillate NOW |
| Wide QRS tachycardia, rate 150-250, no pulse | Pulseless VT | Defibrillate NOW |
| Peaked T waves → widening QRS → sine wave | Hyperkalemia | Calcium IV, insulin/glucose |
| P waves, QRS, no relationship between them + HR 30-40 | Complete heart block | Transcutaneous pacing |
| Absent P, irregularly irregular QRS, narrow | Atrial Fibrillation | Unstable = cardiovert; stable = rate control |
| S1Q3T3 + sinus tach + RBBB + T inversion V1-V4 | Pulmonary Embolism | Heparin, CT-PA, O2 |
| Twisted QRS "twisting the points", long QTc | Torsades de Pointes | Mg 2g IV, stop QT drugs |
| J (Osborn) waves at J-point + bradycardia | Hypothermia | Warm patient, monitor for VF |
PART 7 - ECG CHANGES IN COMMON CONDITIONS (SUMMARY)
| Condition | Key ECG Finding |
|---|---|
| Left bundle branch block (LBBB) | Wide QRS > 0.12 sec, broad notched R in V5-V6 (M shape), QS in V1 |
| Right bundle branch block (RBBB) | Wide QRS > 0.12 sec, rSR' in V1 ("rabbit ears"), wide S in I, V6 |
| Left ventricular hypertrophy | Tall R in V5 + deep S in V1 > 35 mm (Sokolow-Lyon), ST depression in lateral leads |
| Pericarditis | Diffuse saddle-shaped ST elevation in most leads, PR depression |
| Digoxin effect | Scooped ("reverse tick") ST depression, shortened QT |
| Wolff-Parkinson-White (WPW) | Short PR + delta wave (slurred QRS upstroke) |
| Hypokalemia | Flattened T wave, prominent U wave (after T wave), QT prolongation |
| Hypothermia | Osborn (J) wave, sinus bradycardia, PR and QT prolongation |
PART 8 - CLINICAL PEARLS TO REMEMBER
- "Time is muscle" in STEMI - every 30-minute delay in PCI = 7.5% more mortality.
- Normal ECG does not rule out ACS - up to 5% of STEMI patients have a normal initial ECG (posterior STEMI, early hyperacute changes).
- Always check a 12-lead, not just a monitor rhythm - rhythm strips miss ST changes.
- LBBB new or presumed new = STEMI equivalent - activate cath lab.
- The most common ECG finding in PE is sinus tachycardia, not S1Q3T3.
- VT vs. SVT with aberrancy: When in doubt, treat wide complex tachycardia as VT. Never give verapamil for wide complex tachycardia - it can precipitate VF.
- Reciprocal ST depression confirms STEMI (inferior STEMI → ST depression in I, aVL; anterior STEMI → ST depression in inferior leads).
- Peaked T in V1-V4 without chest pain - think hyperkalemia first, then hyperacute STEMI.
- In complete heart block, atropine may not work - move straight to pacing.
- QT interval must be rate-corrected (QTc) - use Bazett's formula: QTc = QT / √(RR in seconds).
Sources: Goldman-Cecil Medicine, p.421-422 | Costanzo Physiology, p.149 | Morgan & Mikhail's Clinical Anesthesiology, p.2179-2180 | Fuster and Hurst's The Heart, 15th Ed | Tintinalli's Emergency Medicine | Harrison's Principles of Internal Medicine 22E, 2025
Can u attach ecg findings of each case as it is easy to understand it
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.