What is 1st line of Drugs of treatment of Migrane
Reading File
Searching PubMed
"migraine" AND "first line treatment"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, textbook-backed answer. Here is the complete response:
First-Line Drugs for Migraine Treatment
Migraine management is divided into two strategies: acute (abortive) treatment to stop an attack, and prophylactic treatment to prevent future attacks.
A. Acute (Abortive) Treatment
1. Mild-to-Moderate Migraine - First Line: NSAIDs / Analgesics
- Aspirin, ibuprofen, naproxen, paracetamol (acetaminophen) are first-line for mild-to-moderate attacks
- A popular OTC combination is aspirin + acetaminophen + caffeine (e.g., Excedrin)
- Try two or three NSAID preparations across successive attacks; moderately high doses may be needed
- Caution: overuse can cause "medication overuse headache" (rebound headache)
Adams and Victor's Principles of Neurology, 12th Ed. - "If the headaches are mild, aspirin, acetaminophen, or another NSAID will suffice and are considered first-line therapy."
2. Moderate-to-Severe Migraine - First Line: Triptans ✦
Triptans are the gold standard and definitive first-line therapy for moderate-to-severe migraine, effective in ~70% of patients.
| Triptan | Route | Notes |
|---|---|---|
| Sumatriptan (prototype) | SC, IN, oral | Fastest SC onset (~20 min); gold standard |
| Zolmitriptan | Oral, nasal | Also available as nasal spray |
| Rizatriptan | Oral | 5 or 10 mg, repeat in 2 h if needed |
| Naratriptan | Oral | Slower onset, fewer side effects |
| Frovatriptan | Oral | Longest half-life (>24 h); good for menstrual migraine |
| Almotriptan, eletriptan | Oral | Alternatives if first triptan fails |
Mechanism: 5-HT1B/1D receptor agonists - cause vasoconstriction of intracranial vessels + inhibit release of proinflammatory neuropeptides from the trigeminal nerve system.
Key points:
- Best given early (during aura or at headache onset); oral forms may be ineffective if given too late
- Subcutaneous sumatriptan: fastest onset, ideal when vomiting prevents oral intake
- If one triptan fails, try another or a different route
- Contraindicated in patients with cardiovascular disease, coronary artery disease, uncontrolled hypertension
Lippincott Illustrated Reviews: Pharmacology - "Sumatriptan was the first available triptan and is the prototype of this class. These agents are first-line agents in the treatment of acute migraine."
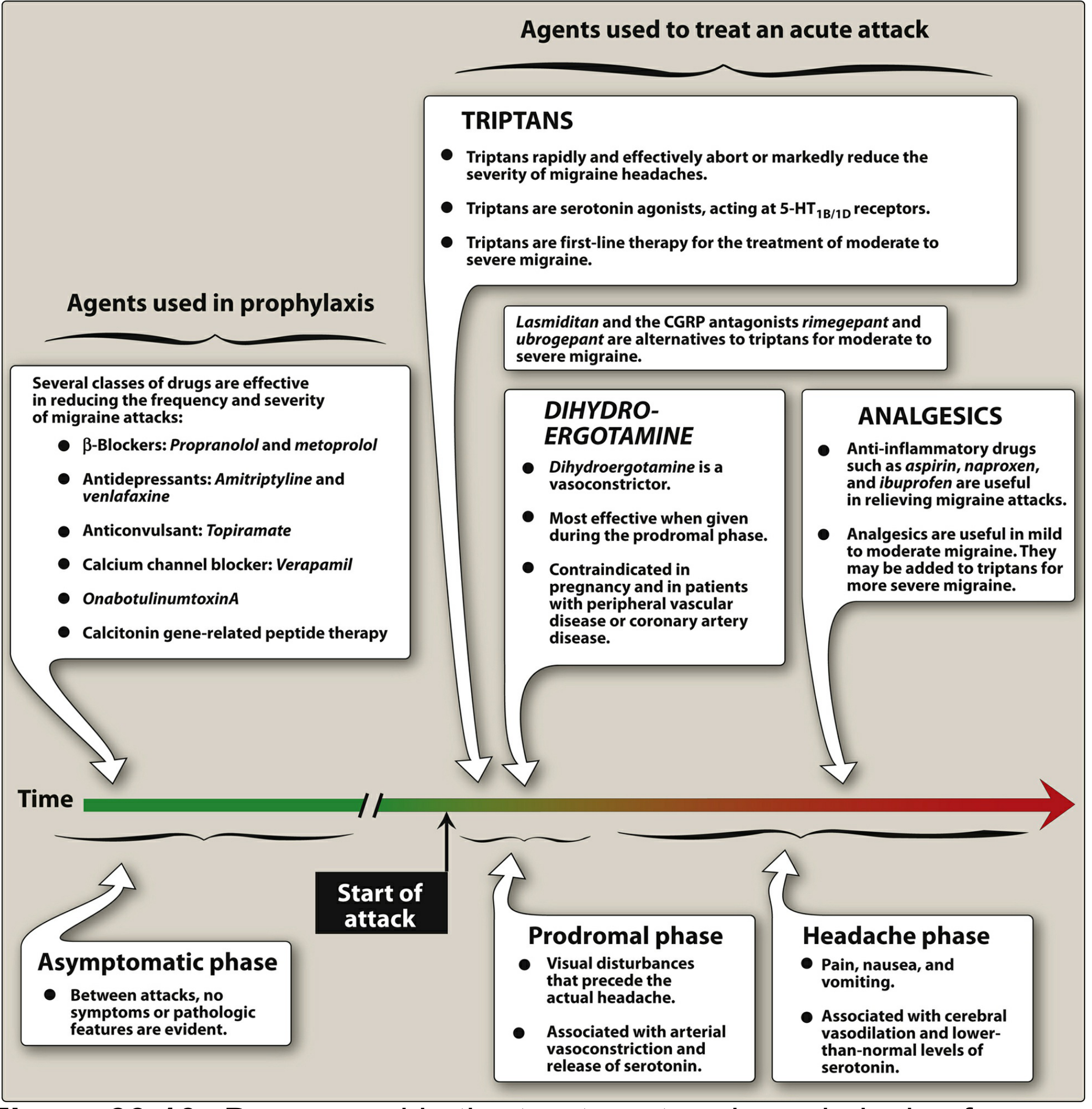
Visual Summary (from Lippincott Pharmacology):
3. Second-Line Acute Agents
| Drug | Notes |
|---|---|
| Dihydroergotamine (DHE) | IV or intranasal; effective but vasoconstrictive side effects; contraindicated in pregnancy and vascular disease |
| Ergotamine tartrate | Sublingual/oral; older agent, risk of dependence and rebound |
| Lasmiditan (ditan) | Oral 5-HT1F agonist; no vasoconstriction; alternative if triptans are contraindicated; controlled substance (driving impairment risk) |
| Gepants (CGRP antagonists) - Rimegepant, Ubrogepant | Oral; for triptan-intolerant patients; no vasoconstriction |
Antiemetics (metoclopramide, prochlorperazine, domperidone) are often added as adjuncts to control nausea and enhance oral drug absorption.
Opioids/butalbital: NOT recommended for routine use.
Tintinalli's Emergency Medicine - "Opiates and barbiturate-containing compounds should not be used routinely for abortive migraine therapy unless other standard treatments fail."
B. Prophylactic (Preventive) Treatment
Indicated when: attacks occur ≥2 times/month, or are severe/disabling, or are complicated by neurologic signs.
First-Line Preventive Drugs
| Class | Drug | Notes |
|---|---|---|
| Beta-blockers (DOC) | Propranolol, metoprolol, timolol, atenolol | Drugs of choice; propranolol 10-20 mg TID, up to 240 mg/day |
| Anticonvulsants | Topiramate, valproate (divalproex) | Avoid valproate in pregnancy |
| Tricyclic antidepressants | Amitriptyline | 25-125 mg nightly; preferred if headaches are very frequent |
| SNRIs | Venlafaxine | Alternative antidepressant |
| Calcium channel blockers | Verapamil | 320-480 mg/day |
Newer Preventive Options
| Drug | Class | Route |
|---|---|---|
| Erenumab, Galcanezumab, Fremanezumab, Eptinezumab | Anti-CGRP monoclonal antibodies | Injectable |
| Rimegepant, Atogepant | Oral CGRP antagonists | Oral |
| OnabotulinumtoxinA | Botox | Injection (chronic migraine) |
Adams and Victor's Principles of Neurology - "The most used agents have been beta-adrenergic blockers, antiepileptic drugs, and tricyclic antidepressants. Often, comorbidities such as depression, hypertension, epilepsy, or coronary artery disease guide the choice among these three classes."
Quick Summary Table
| Situation | First-Line Drug |
|---|---|
| Mild-to-moderate migraine | NSAIDs (ibuprofen, naproxen, aspirin) |
| Moderate-to-severe migraine | Triptans (sumatriptan, rizatriptan, etc.) |
| Vomiting present | SC or intranasal sumatriptan |
| Triptan contraindicated | Lasmiditan or gepants (rimegepant/ubrogepant) |
| Prevention (1st line) | Propranolol or topiramate |
| Prevention + depression | Amitriptyline |
| Prevention + HTN | Propranolol or metoprolol |
| Chronic migraine prevention | OnabotulinumtoxinA |
Recent evidence note: A 2025 Practice Guideline from the French Headache Society (PMID 39406556) and 2025 Saudi CPG (PMID 40199542) are consistent with the above framework - triptans remain first-line for acute moderate-to-severe migraine, with gepants and ditans as alternatives for triptan-intolerant patients. A 2025 systematic review (PMID 39601097) specifically examined patients unsuitable for triptans, highlighting the growing role of CGRP-based therapies in this group.
This is a shared conversation. Sign in to Orris to start your own chat.