Closing volume and residual volume full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material from authoritative sources. Let me compile the full MD exam answer.
Closing Volume (CV) and Residual Volume (RV) — Full Detail (15-Mark Answer)
RESIDUAL VOLUME (RV)
Definition
Residual volume is the volume of air remaining in the lungs after a maximal forced expiratory effort. It is the lowest lung volume achievable. Normal value in a healthy young adult male: ~1.2–1.5 L (approximately 20–25% of TLC).
Why RV Exists — Physiological Basis
RV exists because expiratory airflow ceases before the thoracic cage can reach its minimum volume. Two mechanisms operate:
- Airway closure and gas trapping: At low lung volumes, pleural pressure at the lung bases exceeds airway pressure, causing terminal airways to close. Gas trapped distal to these closed airways cannot be expelled.
- Chest wall elastic recoil: The chest wall's outward recoil limits further inward movement beyond a certain point, even with maximal expiratory muscle effort. The balance between expiratory muscle force and outward chest wall recoil sets the RV.
Normal Values and Relationships
| Parameter | Normal Adult |
|---|---|
| RV | ~1.2–1.5 L |
| RV/TLC ratio | ~20–25% |
| FRC = RV + ERV | ~2.5–3.0 L |
| TLC = RV + VC | ~5.0–6.5 L |
Measurement of RV — Cannot Be Measured by Spirometry Alone
Since a spirometer can only measure volumes that move in and out of the mouth, RV must be inferred from measurements of FRC or TLC using three indirect methods:
1. Body Plethysmography (Gold Standard)
- Patient sits in an airtight box and pants against a closed shutter at FRC.
- Based on Boyle's Law: P₁ × V₁ = P₂ × V₂
- Pressure changes at the mouth (= alveolar pressure) vs. box pressure changes allow calculation of thoracic gas volume.
- RV = FRC − ERV (ERV measured separately by spirometry)
- Advantage: Most accurate; measures ALL intrathoracic gas including trapped gas
- Disadvantage: May overestimate if panting maneuver is too rapid (compresses abdominal gas)
2. Helium Dilution / Inert Gas Dilution
- Patient breathes from a closed circuit containing a known volume (V₁) and concentration (C₁) of helium from FRC.
- Helium equilibrates with alveolar gas: C₁ × V₁ = C₂ × (V₁ + FRC)
- FRC = [(C₁ × V₁)/C₂] − V₁; then RV = FRC − ERV
- Disadvantage: Underestimates RV in patients with obstructive lung disease where trapped gas behind closed airways does not communicate with the breathing circuit (bullae, severe COPD)
3. Nitrogen Washout
- Patient breathes 100% O₂ from FRC until exhaled N₂ reaches a plateau (~<1.5%).
- Knowing initial N₂ concentration (~75%) and total N₂ washed out, FRC is calculated.
- RV = FRC − ERV
- Same underestimation limitation as helium dilution in obstruction
Clinical Significance of RV
| Condition | RV Change | Mechanism |
|---|---|---|
| Emphysema/COPD | ↑↑ | Airway collapse due to ↓ elastic recoil; air trapping |
| Asthma (acute) | ↑ | Bronchospasm causing air trapping |
| Restrictive lung disease | ↓ | Reduced lung/chest wall compliance |
| Neuromuscular disease | ↑ | Weak expiratory muscles cannot expel air; chest wall limitation |
| Normal aging | ↑ | Progressive ↓ elastic recoil; earlier airway closure |
- RV/TLC ratio > 35% suggests air trapping (obstructive pattern)
- An elevated RV (>150% predicted) confirms hyperinflation
- In restrictive disease, RV may be reduced along with TLC
— Goldman-Cecil Medicine, Fishman's Pulmonary Diseases & Disorders, Murray & Nadel's Textbook of Respiratory Medicine
CLOSING VOLUME (CV)
Definition
Closing volume is the lung volume above RV at which airway closure begins in the dependent (basal) lung zones during a slow expiration. It is measured by the single-breath nitrogen (SBN₂) washout test.
- Closing Capacity (CC) = CV + RV
- Normal CV in healthy young adults: ~10% of VC
- CC is therefore a more commonly reported value because it is independent of airway closure position relative to RV
Physiological Basis — Why Airways Close
In the upright lung, a gradient of pleural pressure exists from apex to base (~0.25 cmH₂O per cm vertical distance). Pleural pressure is less negative (more positive) at the base than at the apex.
- At high lung volumes (near TLC): Basal alveoli are on the lower, steep part of their pressure-volume curve → more compliant → better ventilated
- As lung volume falls toward RV: Pleural pressure at the lung bases exceeds airway pressure → terminal bronchioles (non-cartilaginous airways, <2 mm) in the dependent zones collapse and close
- Gas trapped beyond these closed airways cannot be expelled
The elastic recoil of lung parenchyma keeps small airways open. When elastic recoil decreases (aging, emphysema), airways close at higher lung volumes.
Measurement: Single-Breath Nitrogen Washout Test
Technique:
- Subject expires fully to RV
- Inhales a single breath of 100% oxygen to TLC
- Exhales slowly to RV while expired N₂ concentration and volume are continuously recorded
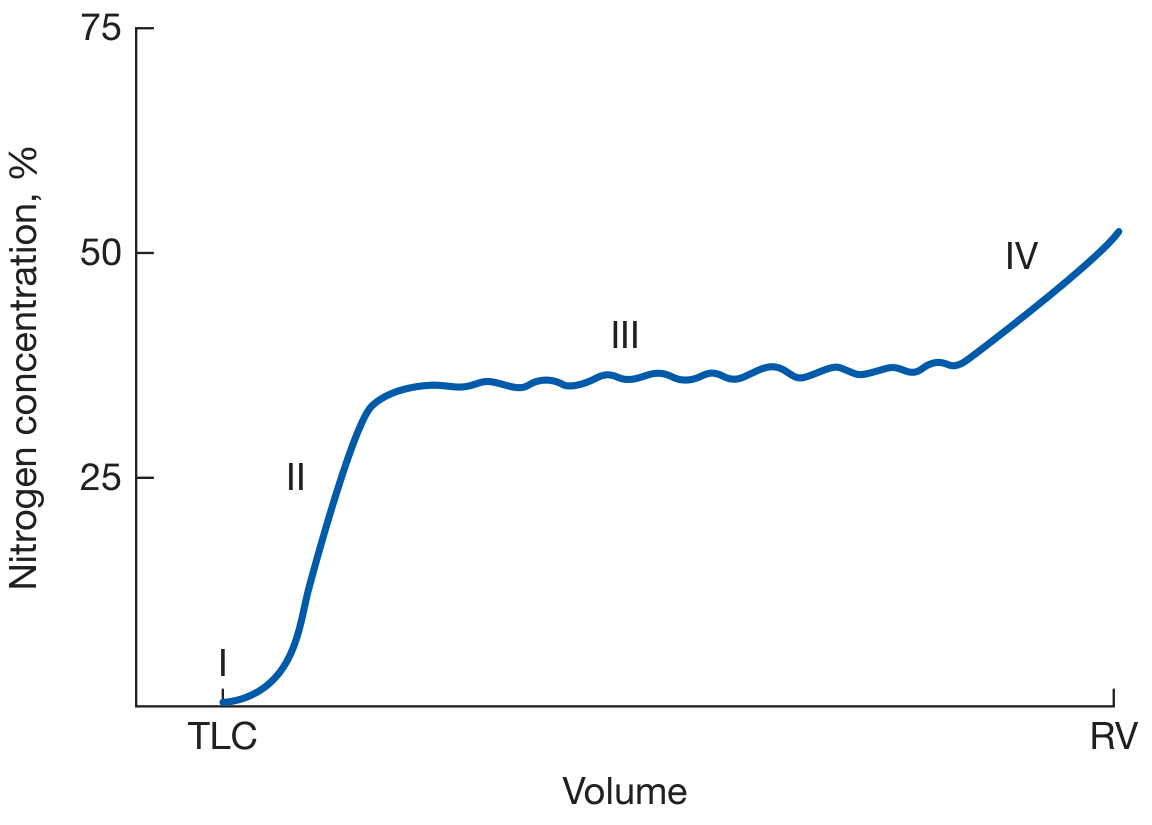
The Four Phases Explained:
| Phase | Description | N₂ Conc. |
|---|---|---|
| I | Pure dead-space O₂; no N₂ | ~0% |
| II | Mixed dead-space + alveolar gas | Rising sharply |
| III | Alveolar plateau — mixed gas from all lung zones; slight upslope in disease | Nearly flat (or gently rising) |
| IV | Abrupt upswing in N₂ due to basal airway closure | Steeply rising |
Why Phase IV occurs (Mechanism):
- At the start of the O₂ inspiration (from RV), basal airways are already closed. The O₂ breath thus enters preferentially to the upper (apical) zones, diluting N₂ there more than at the bases.
- Net result: After the full O₂ inspiration and mixing, basal alveoli have higher N₂ concentration than apical alveoli (because they received proportionally less O₂).
- During expiration, as lung volume approaches CV, basal airways close again. Only apical units (with higher N₂) continue to empty — hence the abrupt rise in expired N₂ concentration = Phase IV.
- The lung volume at which Phase IV begins = CV (volume above RV); adding RV gives CC.
Normal Values and Age Changes
| Group | CV (% VC) | Clinical Implication |
|---|---|---|
| Healthy young adult | ~10% VC | CC well below FRC; no airway closure during tidal breathing |
| Age 50 | ~25% VC | CC approaches FRC |
| Elderly | CC > FRC | Airway closure occurs DURING tidal breathing → V/Q mismatch |
| Infants/neonates | Very high CV | Basal airways close within tidal breathing range |
Key age-related graph:
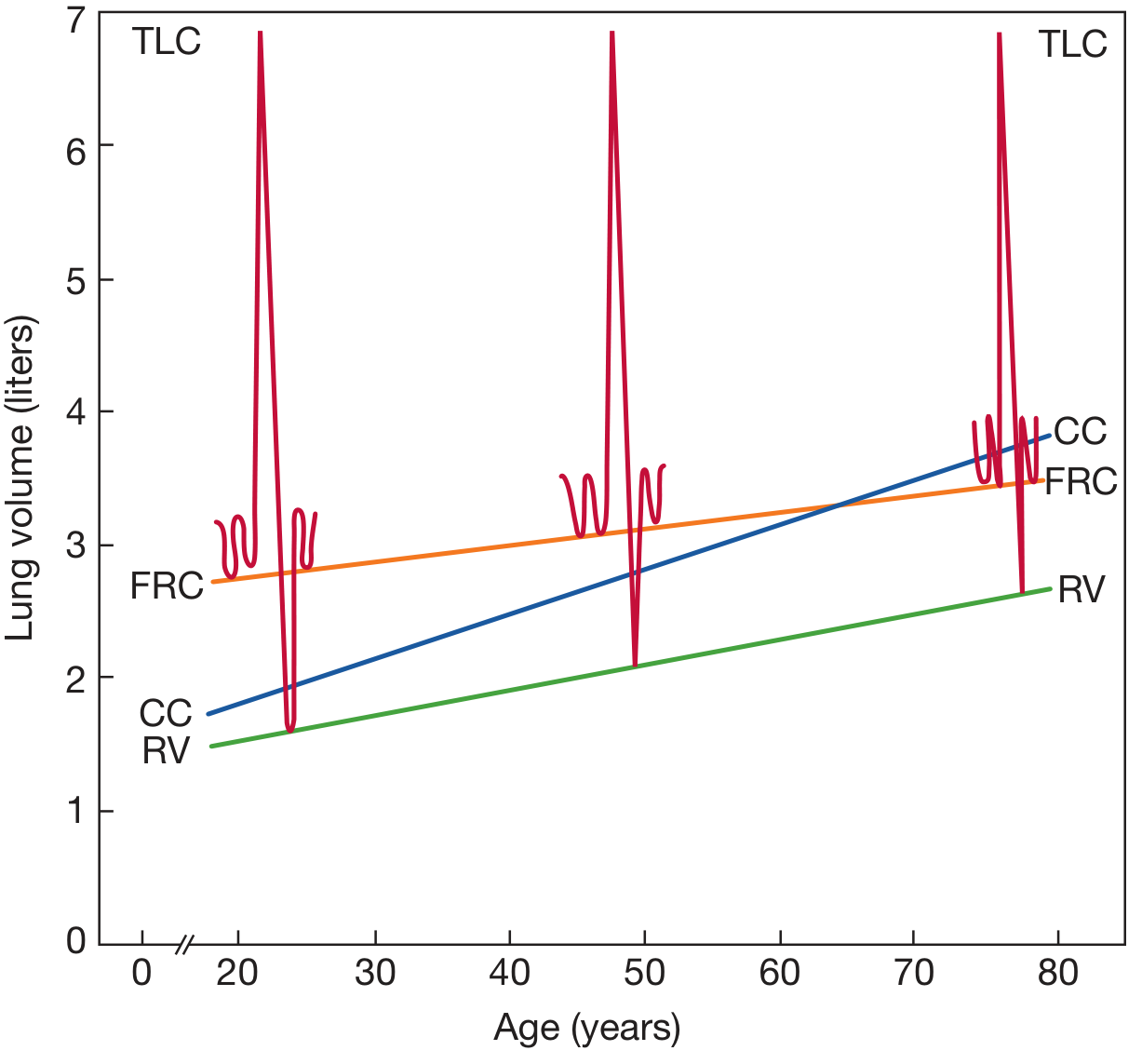
When CV > FRC: Clinical Consequence
- If CC rises above FRC, airways close during normal tidal breathing (not just at RV)
- The closed lung units are still perfused but not ventilated → V/Q mismatch → arterial hypoxemia
- This is the principal cause of the age-related fall in PaO₂
- Supine position: FRC falls by ~0.5–1 L; CC does not change → threshold crossed earlier (explains why supine elderly patients and post-operative patients desaturate more easily)
Factors Increasing CV
| Factor | Mechanism |
|---|---|
| Increasing age | ↓ elastic recoil → airways close at higher volumes |
| Cigarette smoking | Peripheral airway disease; ↓ recoil |
| Emphysema | Destruction of alveolar walls → loss of elastic recoil, airway tethering |
| Small airway disease (early COPD) | Airway wall thickening → closure at higher volumes |
| Obesity | Mechanical compression of lower lobe airways |
| Supine position | ↓ FRC brings CV into tidal range |
| Congestive heart failure | Peribronchial edema; increased CV |
| Neonates/infants | High chest wall compliance → unstable airways |
CV as a Test of Early Small Airway Disease
CV is a sensitive test for peripheral (small) airway dysfunction, detecting disease even before changes appear in conventional spirometry (FEV₁, FVC). An elevated CV/VC% or CC/TLC% suggests early small airway narrowing.
- CV/VC > 20% (age-adjusted): abnormal
- CC/TLC > 30%: abnormal
- Also measured alongside Phase III slope (ΔN₂): normal ΔN₂ <1.5% per 750–1250 mL exhaled
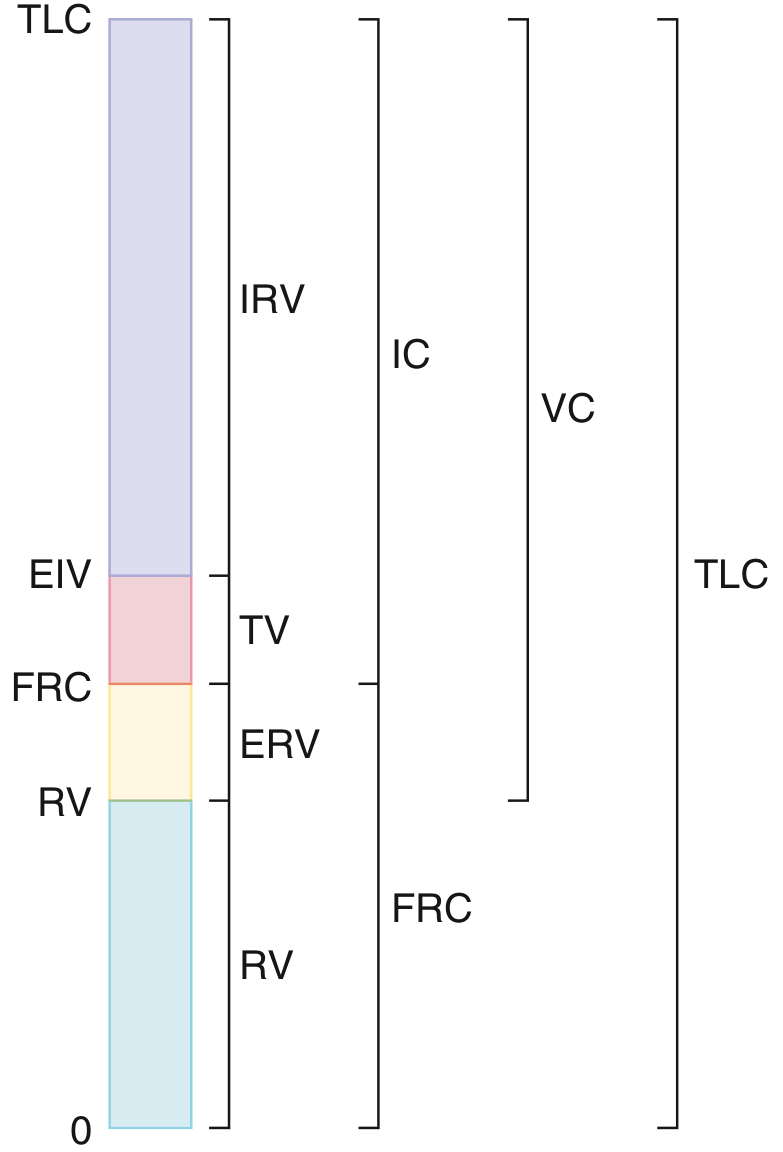
RELATIONSHIP BETWEEN RV, CV, FRC, AND CC — Summary Diagram
TLC ──────────────────
↑
IRV
↑
EIV (end-inspiration of tidal breath)
↑
TV (tidal volume)
FRC ─────────────────── ← CV threshold crosses FRC in aging/disease
↑
ERV
↑
CC ─────────────────── ← (CV + RV): onset of airway closure
↑
CV (above RV)
RV ─────────────────── ← maximal expiration; airways already closed
Key relationships:
- CC = CV + RV
- When CC > FRC → airway closure during tidal breathing → hypoxemia
- Normal: CC < FRC (airways remain open throughout tidal breathing)
- In normal young adults: CV ≈ 10% VC; CC ≈ RV + 0.5 L
SUMMARY TABLE FOR EXAM
| Feature | Residual Volume (RV) | Closing Volume (CV) |
|---|---|---|
| Definition | Volume remaining after maximal expiration | Volume above RV at which basal airway closure begins |
| Normal value | ~1.2–1.5 L (≈20–25% TLC) | ~10% VC in young adults |
| Why it exists | Airway closure + chest wall elastic recoil | ↓ pleural pressure support at lung bases at low volumes |
| Measurement | Body plethysmography, He-dilution, N₂ washout | Single-breath N₂ washout (Phase IV onset) |
| Cannot be measured by | Spirometry alone | Spirometry alone |
| Changes with age | ↑ (airway closure earlier) | ↑ progressively |
| Increased in | Emphysema, COPD, asthma, NMD, obesity | Aging, smoking, emphysema, small airway disease |
| Decreased in | Restrictive disease, fibrosis | — |
| Clinical importance | Air trapping marker; RV/TLC > 35% = obstruction | CC > FRC → V/Q mismatch → hypoxemia; marker of early small airway disease |
| Related capacity | FRC (= RV + ERV), TLC | Closing Capacity CC (= CV + RV) |
Sources: Fishman's Pulmonary Diseases & Disorders (9781260473940); Murray & Nadel's Textbook of Respiratory Medicine (9780323655873); Goldman-Cecil Medicine (9780323930345); Miller's Anesthesia, 10e (9780323935920)
This is a shared conversation. Sign in to Orris to start your own chat.