Invasive arterial blood pressure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive content from two authoritative textbooks. Here is the complete answer:
Invasive Arterial Blood Pressure (IABP) Monitoring
Definition and Principle
Invasive arterial blood pressure monitoring involves the placement of an intra-arterial catheter connected via fluid-filled, low-compliance tubing to an external strain-gauge transducer. The transducer converts mechanical pressure waves into electrical signals that are amplified and displayed as a continuous waveform on a monitor, with digital readouts for systolic, diastolic, and mean arterial pressure (MAP).
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 163
- Schwartz's Principles of Surgery, 11e
Indications
- Current or anticipated hypotension or wide blood pressure swings
- End-organ disease requiring beat-to-beat blood pressure regulation
- Need for repeated arterial blood gas (ABG) sampling or other blood analyses
- Hemodynamic instability in critically ill patients
Contraindications
- Smaller end arteries without collateral blood flow
- Extremities with known or suspected vascular insufficiency
Arterial Sites for Cannulation
| Site | Notes |
|---|---|
| Radial artery (most common) | Superficial, good collateral via ulnar artery and palmar arches; ~5% of patients have incomplete palmar arches |
| Ulnar artery | Deeper, more tortuous; avoid if ipsilateral radial artery has been punctured |
| Brachial artery | Large, close to aorta (less waveform distortion), but prone to kinking at elbow |
| Femoral artery | Excellent access; higher risk of atheroma, pseudoaneurysm, infection, and thrombosis |
| Axillary artery | Risk of nerve damage (axillary plexus); retrograde cerebral embolism possible; useful in burn patients |
| Dorsalis pedis / posterior tibial | Most distal; highest waveform distortion |
Peripheral vs. central pressure: Systolic pressure is higher and diastolic is lower in peripheral arteries compared to the aorta, but MAP is approximately the same.
Allen Test and Collateral Flow Assessment
Before radial artery cannulation, collateral flow should be confirmed:
- Modified Allen test: Compress radial and ulnar arteries while the patient makes a fist. Release ulnar pressure - normal flushing of the thumb within 5 seconds confirms adequate collateral flow. >10 seconds indicates poor collateral circulation.
- Limitation: The Allen test is of questionable reliability; many practitioners prefer Doppler probe, plethysmography, or pulse oximetry over the radial artery occlusion, which do not require patient cooperation.
Radial Artery Cannulation Technique
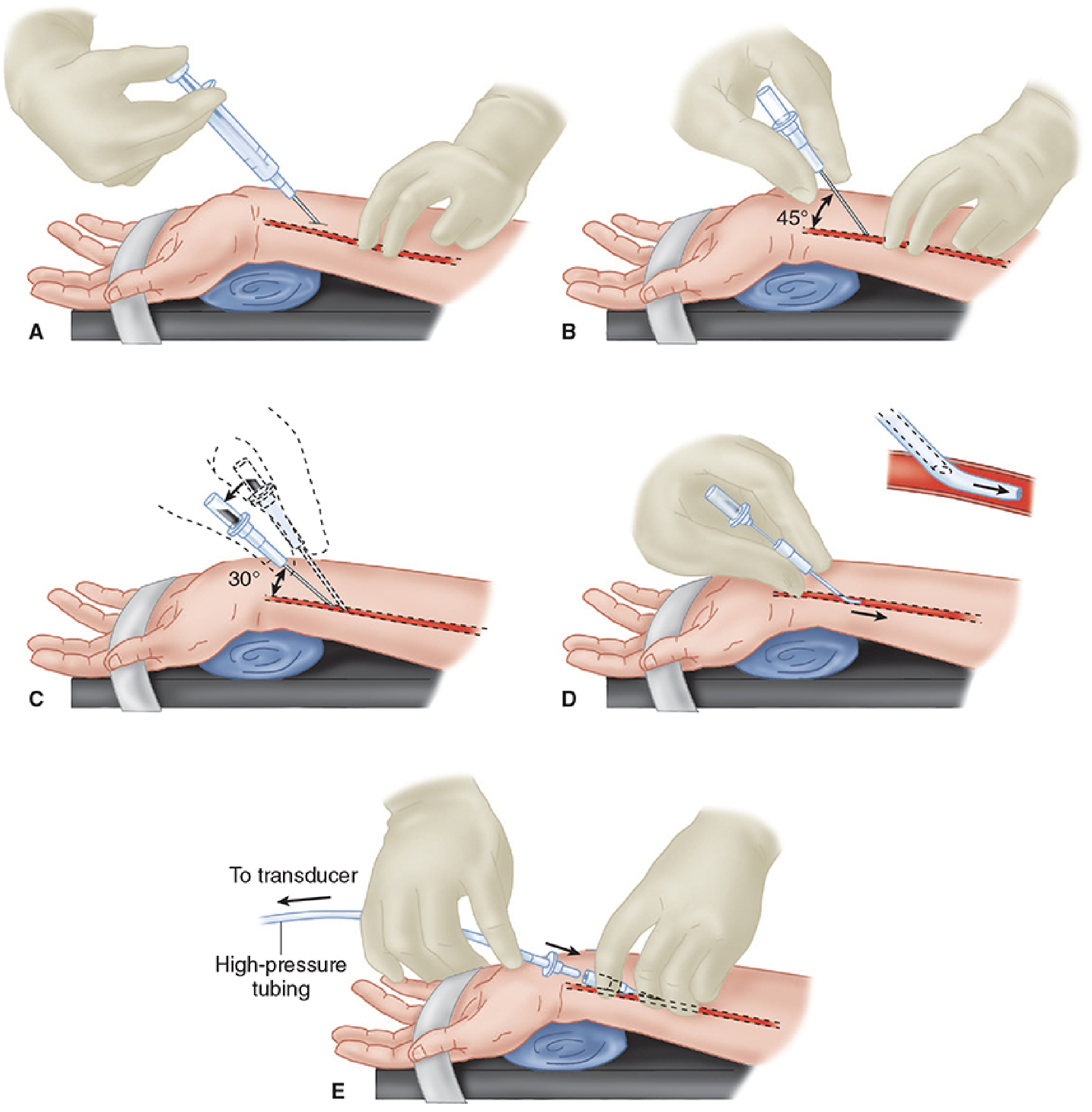
Steps: (A) Supinate and extend wrist; palpate radial pulse; prep skin and infiltrate lidocaine. (B) Insert 20- or 22-gauge catheter at 45° angle. (C) On blood flashback, lower to 30° and advance 1-2 mm to confirm intraluminal position. (D) Advance catheter over needle; withdraw needle. (E) Apply proximal pressure to prevent blood loss; connect high-pressure tubing to transducer.
The Catheter-Tubing-Transducer System
Frequency Response and Damping
- The arterial pulse waveform is a complex signal with a natural frequency of approximately 16-24 Hz
- The measuring system's natural frequency must exceed the pulse frequency for accurate reproduction
- Disposable transducers have frequencies >200 Hz, but tubing, stopcocks, and air bubbles all lower this
- The optimal damping coefficient (β) is 0.6 to 0.7
| System State | Systolic | Diastolic | MAP |
|---|---|---|---|
| Underdamped | Overestimated (overshoot) | Underestimated | Accurate |
| Overdamped | Underestimated | Overestimated | Accurate |
| Optimal | Accurate | Accurate | Accurate |
Key clinical point: Even in poorly damped systems, MAP remains accurately measured as long as the system is properly calibrated. Clinical decisions should be based on MAP.
To optimize the system: minimize tubing length, eliminate unnecessary stopcocks, remove air bubbles, and use low-compliance tubing.
Transducer Mechanism
The transducer diaphragm is distorted by pressure waves, converting mechanical energy into electrical signal. Sensing elements are arranged as a Wheatstone bridge circuit - stretching a wire or silicone crystal changes its electrical resistance, and the resulting voltage differential is proportional to the applied pressure.
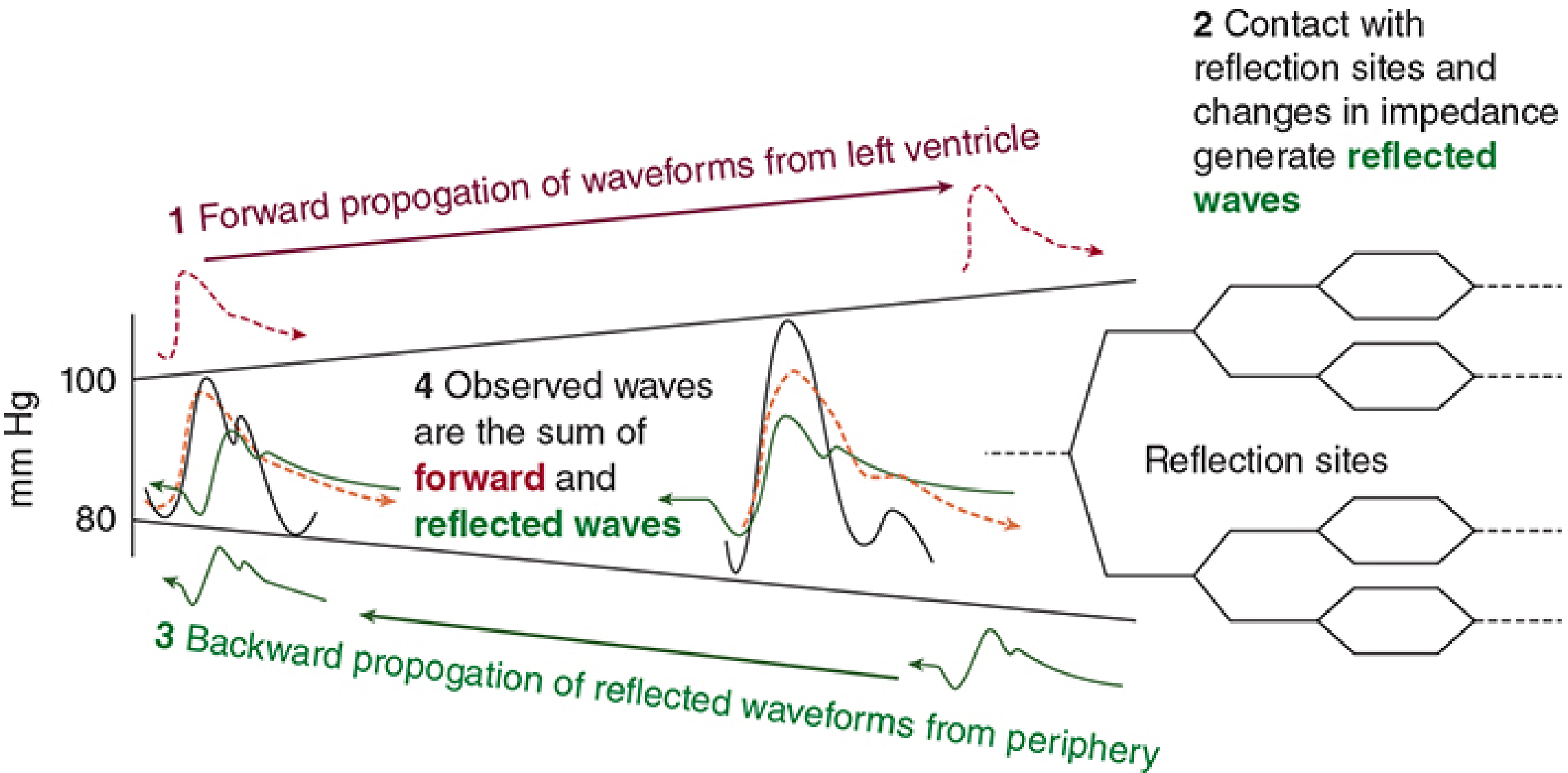
Waveform Interpretation
The arterial waveform is the summation of forward-traveling waves (from the LV) and reflected waves from the periphery:
Clinically useful waveform features:
| Feature | Clinical Significance |
|---|---|
| Rate of upstroke | Reflects myocardial contractility |
| Rate of downstroke | Reflects peripheral vascular resistance |
| Exaggerated respiratory variation in pulse pressure | Suggests hypovolemia or excessive tidal volumes |
| Pulse pressure increases toward periphery | Normal physiological phenomenon (mean pressure decreases) |
Zeroing and Calibration
- Open a stopcock at the level of the desired measurement point (usually the midaxillary line) to atmosphere, then activate the zero trigger
- If the table is repositioned, the transducer must be moved in tandem or re-zeroed
- In seated patients (e.g., craniotomy), zero at the level of the ear (circle of Willis) to reflect cerebral perfusion pressure
- Re-zero regularly as transducer readings can drift
Complications
| Complication | Notes |
|---|---|
| Hematoma | Most common |
| Arterial thrombosis | Increased with large catheters, prolonged cannulation; minimize with 20-gauge or smaller |
| Distal ischemia / digit necrosis | Ensure adequate collateral flow pre-insertion |
| Retrograde embolization (air/thrombi) | Avoid flushing when air is present; especially risky at axillary site |
| Pseudoaneurysm | More common at femoral site |
| Infection | Higher at femoral site |
| Nerve damage | Risk at axillary site (axillary plexus) |
| Bleeding / disconnection | Continuous waveform monitoring helps detect |
| Unintentional intraarterial drug injection | Risk if line is confused for IV |
Factors increasing complication risk: prolonged cannulation, repeated insertion attempts, extracorporeal circulation, large catheters in small vessels, vasopressors, and hyperlipidemia.
Additional Utility
- Continuous ABG access without repeated punctures
- Cardiac output estimation via arterial waveform analysis (pulse contour/pulse power methods)
- Beat-to-beat assessment of fluid responsiveness (stroke volume variation, pulse pressure variation)
Sources: Morgan and Mikhail's Clinical Anesthesiology, 7e (pp. 163-169) | Schwartz's Principles of Surgery, 11e
Roman Urdu ma bh samjao Sath Sath he aur difficult word kki bh definition roman Urdu ma he
Invasive Arterial Blood Pressure (IABP) Monitoring
Roman Urdu Mein Mukammal Wazahat
Tareef aur Buniyadi Usool
(Definition and Basic Principle)
Invasive arterial blood pressure monitoring (seedha khoon ki nali mein daal kar blood pressure naapna) ek aisi technique hai jisme ek intra-arterial catheter (khoon ki nali ke andar daali jaane wali patli nali) lagayi jati hai. Yeh catheter fluid-filled tubing ke zariye ek strain-gauge transducer (pressure ko bijli ke signal mein badalne wala آlat) se juri hoti hai.
Transducer pressure waves ko electrical signals mein convert karta hai, jo monitor par ek continuous waveform (musalsal lahar jaisi tasveer) ke roop mein dikhti hai — saath mein systolic, diastolic, aur MAP (Mean Arterial Pressure) (ausat sharaani dabao) ke digital numbers bhi.
Indications (Zaroorat kab hoti hai?)
- Hypotension (blood pressure ka bohat zyada girna) ya iske andeshay mein
- Blood pressure mein achanak bohat zyada upar-neechay hona
- End-organ disease (dil, gurday, dimagh jaisi zaruri azao ki bimari) jisme har dhadkan par BP control zaroori ho
- Baar baar ABG (Arterial Blood Gas) (khoon mein oxygen aur CO2 ka test) lene ki zaroorat ho
- ICU mein critically ill (bohat zyada beemar) marizo mein
Contraindications (Kab nahi lagana chahiye?)
- Woh arteries (khoon ki naliyan) jo choti hon aur jinka koi collateral blood flow (alternative rasta jisse khoon aata ho) na ho
- Jis haath ya paon mein pehle se vascular insufficiency (khoon ki naliyon ki kamzori ya blockage) ho
Arterial Sites (Kahan kahan laga sakte hain?)
| Site | Roman Urdu Notes |
|---|---|
| Radial artery (kalai) | Sab se zyada use hoti hai; upar se saaf dikh ti hai; collateral flow (alternative khoon ka rasta) ulnar artery se milta hai |
| Ulnar artery (kalai ka doosra hissa) | Gehra aur tedha rasta; agar radial fail ho jaaye tab bhi is taraf nahi jaana chahiye |
| Brachial artery (kohni ke paas) | Bari nali; aorta ke qareeb hone se waveform (lahar) achi milti hai; kohni par bend hone se kink *(band) hone ka khatra |
| Femoral artery (ran ki nali) | Asaani se milti hai; magar infection aur thrombosis (khoon ka jamna) ka risk zyada |
| Axillary artery (bagal ki nali) | Nerve damage (nerve ki takleef) ka khatra; jale hue mariz mein use hoti hai |
| Dorsalis pedis / Posterior tibial (paon) | Sab se door; waveform (lahar) sabse zyada distorted (bigri hui) hoti hai |
Yaad rakho: Peripheral arteries (dorr ki naliyon) mein systolic pressure aorta se zyada hoti hai, diastolic kam hoti hai — lekin MAP (ausat dabao) dono jagah approximately barabar rehta hai.
Allen Test (Collateral Flow Check)
Radial artery mein catheter daalne se pehle yeh test karo:
- Mareed apna haath band kare (mutthi) — khoon nikaal bahar
- Aap dono arteries (radial aur ulnar) ko angliyon se dabaao
- Haath khulwaao — haath safed ho jayega
- Ulnar artery par se pressure hatao
- Agar 5 seconds mein angootha laal ho jaye — collateral flow theek hai ✓
- 10 seconds se zyada lage — collateral flow poori nahi — test negative ✗
Important: Allen test zyada reliable nahi hai. Behtar hai Doppler probe (sound waves se khoon ka flow check karna), pulse oximetry (oxygen level sensor), ya plethysmography (khoon ke volume ki measurement) use karo — inhe mareez ki cooperation bhi nahi chahiye.
Radial Artery Cannulation Technique (Tareeqa)
Step by Step:
- (A) Kalai ko seedha aur peeche ki taraf extend (kheencho) karo. Radial pulse (nabz) palpo karo. Skin saaf karo, lidocaine (dard khatam karne ki dawa) inject karo
- (B) 20- ya 22-gauge catheter ko 45° angle par skin mein daalo
- (C) Jab blood flashback (catheter mein khoon aaye) dikhe — angle 30° par lao aur 1-2 mm aur andar daalo taake catheter nali ke andar poori tarah ho
- (D) Catheter ko needle ke upar se nali mein aage push karo; needle nikaalo
- (E) Proximal *(upar wali) jagah par pressure rakho taake khoon na nikle; high-pressure tubing (mazboot nali) transducer se connect karo
Catheter-Tubing-Transducer System (Poora Setup)
Frequency Response aur Damping (Signal ki Quality)
Natural frequency (qudrati tarddud) — system ki apni vibration speed. Arterial pulse ki frequency 16-24 Hz hoti hai. System ka natural frequency is se zyada hona chahiye warna signal bigad jaata hai.
Damping (signal ka dheema hona) — Optimal damping coefficient (behtar hone ka andaza) 0.6 se 0.7 hona chahiye.
| System ki Halat | Systolic | Diastolic | MAP |
|---|---|---|---|
| Underdamped (zyada bounce) | Galat zyada (overestimated) | Galat kam (underestimated) | Sahi ✓ |
| Overdamped (zyada manda) | Galat kam (underestimated) | Galat zyada (overestimated) | Sahi ✓ |
| Optimal (bilkul theek) | Sahi ✓ | Sahi ✓ | Sahi ✓ |
Sabse ahem baat: Chahe system underdamped ho ya overdamped — MAP har haal mein sahi aata hai (jab tak calibration theek ho). Isliye clinical decisions MAP par karo, na sirf systolic par.
System behtar banane ke liye:
- Tubing (nali) ki lambai kam karo
- Faaltu stopcocks (band/khulne wale valves) hatao
- Air bubbles (hawa ke bulbule) bilkul nahi hone chahiye
- Low-compliance tubing (sakht, kam kheenchne wali nali) use karo
Transducer ka Kaam (Kaise Kaam Karta Hai?)
Transducer ke andar ek diaphragm (patli jhilli) hoti hai jo pressure se hilti hai. Yeh hilna Wheatstone bridge circuit (ek khaas bijli ka circuit jo pressure measure karta hai) ke zariye voltage (bijli ka dabao) mein badal jaata hai — jitna zyada pressure, utna zyada voltage signal.
Waveform Interpretation (Lahar ko Samajhna)
Arterial waveform do cheezon ka jod hai:
- Forward waves (seedhi lehrein) — LV (left ventricle / dil ka baayaan kamra) se aane wali
- Reflected waves (wapas aane wali lehrein) — periphery (door ke hisson) se palat kar aane wali
| Waveform ki Khasiyat | Kya Batata Hai? |
|---|---|
| Upstroke ki speed (upar jaane ki tezi) | Dil ki contractility (dhadhakne ki taaqat) |
| Downstroke ki speed (neechay aane ki tezi) | Peripheral vascular resistance (door ki naliyon mein resistance/rukawat) |
| Saans ke saath zyada upar-neechay hona | Hypovolemia (khoon/pani ki kami) ya zyada bari saans (tidal volume) |
| Pulse pressure (systolic minus diastolic) periphery mein zyada | Yeh normal hai — mean pressure wahan thoda kam hota hai |
Zeroing aur Calibration (Sifar par Laana)
- Transducer ko midaxillary line (baazu ke beech ki line) ke level par rakho — stopcock kholo aur zero trigger dabao
- Agar table upar neechay ho — transducer bhi saath mein hilao ya dubara zero karo
- Baithe hue mareed mein (maslan brain surgery) — transducer ko kaan ke level par zero karo — yeh circle of Willis (dimagh ki khoon ki naliyon ka gol chakkar) ke barabar hai
- Waqt ke saath drift (readings ka khud ba khud badalna) ho sakta hai — isliye baar baar zero verify karo
Complications (Kya Masaail Aa Sakte Hain?)
| Masla | Roman Urdu Wazahat |
|---|---|
| Hematoma (khoon ka jama hua dhair) | Sab se aam masla |
| Arterial thrombosis (nali mein khoon ka jamna) | Badi catheter ya zyada waqt tak lagay rakhne se |
| Distal ischemia (aage ke hisson mein khoon na pahunchna) | Haath ya ungliyan kaali pad sakti hain |
| Retrograde embolization (hawa ya khoon ka chhota tukda wapas dimagh ki taraf jaana) | Hawa hone par flush mat karo |
| Pseudoaneurysm (nakli gilthi — nali ki dewar mein sourag) | Femoral site par zyada |
| Infection (jrasoomat) | Femoral site par zyada khatra |
| Nerve damage (nerve ko nuqsan) | Axillary site par zyada |
| Accidental intra-arterial drug injection (galti se nali mein dawa) | Line ko IV samajh lene par |
Khatra zyada in mareezon mein:
- Zyada waqt tak catheter laga rahe
- Baar baar try kiya jaaye
- Bari catheter choti nali mein
- Vasopressors (blood pressure barhane wali dawaen) use ho rahi hon
- Hyperlipidemia (khoon mein zyada charbi) ho
Fayde (Extra Clinical Uses)
- Baar baar ABG lena bina needle chubhaye
- Cardiac output (dil kitna khoon pump karta hai) ka andaza waveform se lagana
- Pulse pressure variation / Stroke volume variation (saans ke saath khoon ke waali mein farq) dekh kar fluid responsiveness (pani dene se faida hoga ya nahi) janchhna — ICU mein bohat kaam aata hai
Summary ek line mein: Invasive arterial BP monitoring ICU aur OT mein sab se reliable, continuous, beat-to-beat blood pressure monitor hai — radial artery sab se zyada use hoti hai, MAP sab se bharosemand reading hai, aur transducer ko sahi level par zero karna sab se zaroori step hai.
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Schwartz's Principles of Surgery, 11e

1000550862.png
Isko samjao aur related cheezen bh batana aur important exam tips bh aur phely English ma phr roman Urdu phr difficult words ki definition thk hai
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Ab mere paas saari zaruri malumat hai. Chalo poora jawab likhte hain:
Arterial Catheterization Techniques
(Khoon Ki Nali Mein Catheter Daalne ke Tarikey)
PART 1 — ENGLISH EXPLANATION
1. Catheter-Over-Wire Technique
(Primary / Main Approach)
This is the main method used for arterial catheterization. It has two sub-types:
A. Seldinger Technique
Uses separate, individual components one by one:
| Step | Action |
|---|---|
| 1 | Insert needle into the artery |
| 2 | Pass guidewire through the needle's hub into the artery |
| 3 | Remove the needle, leaving the guidewire in place |
| 4 | Slide the catheter over the guidewire into the artery |
| 5 | Remove the guidewire; catheter stays in artery |
- Best for central vessels (deeper arteries like femoral, axillary) that run deep into the body
- All components (needle, guidewire, catheter) are separate items
B. Modified Seldinger Technique
Uses an integrated needle-catheter-wire system — everything is combined in one device:
| Step | Action |
|---|---|
| 1 | Insert introducer needle (which already has a fine catheter over it) |
| 2 | Remove the introducer needle |
| 3 | Push the fine catheter forward |
| 4 | Pass the guidewire through the fine catheter |
| 5 | Remove the fine catheter |
| 6 | Slide the final arterial catheter over the guidewire |
- More streamlined because the needle and catheter are pre-assembled
- Reduces the number of loose components
2. Catheter-Over-Needle Technique
This is similar to how a regular IV cannula (drip) is inserted in peripheral veins:
| Step | Action |
|---|---|
| 1 | Localize the artery by palpation or ultrasound |
| 2 | Directly puncture the artery with catheter-over-needle device at 30-45° |
| 3 | Blood flashback seen in needle hub = artery confirmed |
| 4 | Lower angle to 30°, advance 2 mm to ensure tip is inside lumen |
| 5 | Slide catheter forward over the needle into the artery |
| 6 | Remove needle; attach pressure tubing |
- Most effective for superficial arteries — especially the radial artery at the wrist
- Simple, fast, no guidewire needed
- Same concept as inserting a standard IV cannula
3. Arterial Cutdown
A surgical procedure where the artery is physically cut open and exposed:
- Skin and subcutaneous tissue are incised to visually expose the artery
- Two vessel loops (sutures) are passed under the artery to control and stabilize it
- Then the artery is directly cannulated under direct vision
- Strongly discouraged - only a last resort when all other methods have failed
- Must only be done by trained physicians/surgeons
- Most commonly demonstrated at the brachial artery in the antecubital fossa (inner elbow)
- Risk of damage to nearby structures: median nerve, brachial vein, ulnar nerve
Comparison Table: All Three Techniques
| Feature | Seldinger | Modified Seldinger | Catheter-over-Needle | Arterial Cutdown |
|---|---|---|---|---|
| Components | Separate | Integrated (one unit) | Single device | Surgical kit |
| Guidewire used? | Yes | Yes | No | No |
| Best for | Deep vessels | Deep vessels | Superficial (radial) | Last resort only |
| Complexity | Moderate | Moderate | Simple | Most complex |
| Training needed | Moderate | Moderate | Basic | Advanced surgical |
| Speed | Moderate | Moderate | Fastest | Slowest |
Related Important Concepts
Ultrasound Guidance
- Now the preferred method for artery localization
- Reduces failed attempts and complications
- Can be used with any of the above techniques
Why Guidewire Technique is Superior
- Studies show guidewire-directed (Seldinger) techniques have higher overall success rates than direct over-the-needle cannulation
- Especially useful when direct cannulation has already failed - Modified Seldinger can "rescue" a failed attempt
Arterial Cutdown Anatomy (from diagram)
The diagram shows brachial artery cutdown at the antecubital fossa with 4 panels:
- Panel A: Surface anatomy showing brachial artery path in the arm
- Panel B: After skin incision - brachial artery and median nerve exposed
- Panel C: Vessel loops placed under brachial artery (also showing brachial vein and ulnar nerve)
- Panel D: Artery fully elevated and ready for direct cannulation
⭐ EXAM TIPS
- "Primary approach" = Catheter-over-wire technique - this is the standard/default method
- Seldinger = SEPARATE components; Modified Seldinger = INTEGRATED system - this distinction is a common MCQ trap
- Catheter-over-needle = best for radial artery (superficial) - same principle as a peripheral IV
- Arterial cutdown = last resort only - if MCQ says "all else has failed" or "last resort" → answer is cutdown
- Seldinger technique order: Needle → Guidewire → Remove needle → Catheter over wire → Remove wire
- Modified Seldinger order: Needle+fine catheter → Remove needle → Push fine catheter → Guidewire → Remove fine catheter → Arterial catheter
- Cutdown = surgeon only - if MCQ asks who performs it → physician with adequate/surgical training
- Guidewire success rates > direct cannulation (Roberts & Hedges)
- Never force a catheter - if it doesn't thread easily, it's not in the lumen
- Ultrasound = preferred guidance for difficult arterial access
PART 2 — ROMAN URDU WAZAHAT
1. Catheter-Over-Wire Technique
(Taar ke Upar Catheter Daalney ka Tareeqa)
Yeh arterial catheterization ka sabse pehla aur aam tareeqa hai. Iske do qism hain:
A. Seldinger Technique
Isme sab cheezein alag alag istemal hoti hain, ek ke baad ek:
| Qadam | Kya Karo |
|---|---|
| 1 | Needle ko artery mein daalo |
| 2 | Needle ke andar se guidewire (patla taar) artery mein dhakailo |
| 3 | Needle nikaalo — taar andar rehta hai |
| 4 | Catheter (patli nali) ko taar ke upar se nali mein dhakailo |
| 5 | Taar nikaalo — catheter artery mein reh jaata hai ✓ |
- Central vessels (gehra wali badi naliyan — jaise femoral, axillary) ke liye best hai
- Har cheez alag alag hoti hai
B. Modified Seldinger Technique
Isme sab kuch ek hi device mein hota hai:
| Qadam | Kya Karo |
|---|---|
| 1 | Introducer needle (shuru karne wali sui) daalo — iske upar already ek fine catheter (bohat patli nali) hoti hai |
| 2 | Needle nikaalo |
| 3 | Fine catheter aage badhao |
| 4 | Guidewire (taar) fine catheter ke zariye andar bhejo |
| 5 | Fine catheter nikaalo |
| 6 | Asli badi arterial catheter taar ke upar se andar daalo |
- Sab ek saath integrated (juda hua) hota hai
- Loose cheezein kam hoti hain
2. Catheter-Over-Needle Technique
(Needle ke Upar Catheter Wala Tareeqa)
Yeh bilkul normal drip lagane jaisa hai — jaise hospital mein haath mein pani ki nali lagate hain:
| Qadam | Kya Karo |
|---|---|
| 1 | Artery dhoondhon — hath se ya ultrasound (sound waves wala machine) se |
| 2 | Catheter-over-needle device ko 30-45 degree angle par skin mein ghusao |
| 3 | Needle ke sar mein khoon aaye (blood flashback) = artery confirm |
| 4 | Angle 30° karo aur 2mm aur andar jao |
| 5 | Catheter ko needle ke upar se artery mein aage dhakailo |
| 6 | Needle nikaalo; tubing lagao |
- Radial artery (kalai ki nali — jo upar se saaf dikh ti hai) ke liye sab se best
- Koi taar nahi chahiye — seedha simple
- Agar catheter aasaani se nahi jaata — zorr mat karo — matlab andar sahi nahi hai
3. Arterial Cutdown
(Surgery Karke Nali Kholna)
Yeh ek surgical procedure (operation wala tareeqa) hai jisme artery ko physically kaat kar khola jaata hai:
- Skin aur neechay ki tissue kaati jaati hai taake artery aankh se dikh sake
- Artery ke neechay se do vessel loops (suture ki loop — artery ko pakarne ke liye) daalay jaate hain
- Artery ko upar uthaaya jaata hai, phir seedha nazar ke saamne catheter daalte hain
- Bohat discouraged hai — sirf tab karo jab koi aur tareeqa kaam na kare (last resort)
- Sirf trained surgeon/doctor hi kar sakta hai
- Brachial artery (kohni ke andar wali nali) par aksar dikhaya jaata hai
- Khatre: median nerve (ek nerve), brachial vein (nali ke paas khoon ki ragein), ulnar nerve (doosri nerve) ko nuqsan ho sakta hai
Teeno Ka Comparison (Farq Samajhna)
| Cheez | Seldinger | Modified Seldinger | Catheter-over-Needle | Cutdown |
|---|---|---|---|---|
| Parts | Alag alag | Sab ek mein | Ek hi piece | Surgical set |
| Taar (guidewire)? | Haan | Haan | Nahi | Nahi |
| Kis ke liye best | Gehra nali | Gehra nali | Kalai (radial) | Aakhri chaara |
| Mushkil? | Darmiyaana | Darmiyaana | Aasaan | Sabse mushkil |
| Teez? | Darmiyaana | Darmiyaana | Sabse teez | Sabse slow |
⭐ EXAM TIPS — Roman Urdu Mein
- "Primary approach" = Catheter-over-wire — yeh standard tareeqa hai, yaad rakho
- Seldinger = ALAG parts; Modified Seldinger = INTEGRATED (juda hua) ek system — MCQ mein yahi farq poochhte hain
- Catheter-over-needle = radial artery ke liye best — wajah: yeh superficial (upar se dikh ti) hai
- Cutdown = SIRF last resort — MCQ mein "jab sab fail ho jaaye" → answer = cutdown
- Seldinger ka order yaad karo: Needle → Taar andar → Needle bahar → Catheter taar par → Taar bahar
- Modified Seldinger ka order: Needle+thin catheter → Needle bahar → Thin catheter aage → Taar andar → Thin catheter bahar → Badi catheter
- Cutdown = sirf surgeon — MCQ mein "kaun karta hai" → trained physician/surgeon
- Taar (guidewire) wala tareeqa seedha needle wale se zyada successful hota hai
- Catheter nahi ghus raha → zorr mat karo — matlab nali ke andar sahi nahi
- Ultrasound = mushkil access mein preferred tareeqa
PART 3 — DIFFICULT WORDS KI DEFINITIONS
(Roman Urdu Mein)
| Mushkil Lafz | Roman Urdu Definition |
|---|---|
| Catheterization | Khoon ki nali ya kisi nali mein patli tube (catheter) daalne ka amal |
| Arterial | Artery se mutalliq — artery woh nali hai jisme dil se saaf khoon jaata hai |
| Catheter | Ek patli, lachkili nali jo khoon ki nali, masaana, ya kisi aur jagah mein daali jaati hai |
| Guidewire | Ek bohat patla, lachkila taar jiske upar catheter daala jaata hai — raasta guide karta hai |
| Seldinger | Ek Swedish doctor ka naam jisne yeh technique 1953 mein ijaad ki — taar ke zariye catheter daalna |
| Integrated | Sab kuch ek hi cheez mein milaya hua — alag alag nahi |
| Introducer needle | Woh pehli sui jo shuru mein artery mein daali jaati hai — raasta kholne ke liye |
| Superficial | Jild (skin) ke qareeb — upar wala — asaani se nazar aane wala |
| Surgical procedure | Operation wala kaam — surgeon karta hai — skin kaatna padta hai |
| Last resort | Aakhri chaara — tab karo jab koi aur kaam na kare |
| Arterial cutdown | Surgery karke artery ko ankhon ke saamne expose (kholna) karna — phir catheter daalna |
| Vessel loops | Suture ya loop jo artery ke neechay daali jaati hai — artery ko pakarne aur control karne ke liye |
| Antecubital fossa | Kohni ke andar wali jagah — jahan aap BP cuff lagate hain — brachial artery yahan hoti hai |
| Median nerve | Haath ki ek ahem nerve jo antecubital fossa mein hoti hai — cutdown mein isko nuqsan hone ka khatra |
| Brachial artery | Baazu ki badi artery jo kohni ke paas se guzarti hai |
| Cannulation | Kisi nali (artery/vein) mein catheter daalne ka amal |
| Lumen | Nali ke andar ka khali hissa — jahan se khoon guzarta hai |
| Blood flashback | Jab needle sahi jagah (artery/vein mein) jaaye to khoon needle ke sar mein aata hai — confirm karti hai |
| Proximal | Dil ki taraf — jism ke markaz ki taraf |
| Distal | Door wala hissa — haath, paon ki taraf |
| Peripheral | Jism ke kinaray wala — door ki naliyan |
| Percutaneous | Skin ke zariye — bina kaat ke — seedha skin mein se ghusana |
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine | Morgan & Mikhail's Clinical Anesthesiology, 7e | Tintinalli's Emergency Medicine

1000550875.png
Ye bh same aise he samja do jiase phely waly samjain hain
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Ab mere paas saari zaruri details hain. Poora jawab likhte hain:
Basic Principle, Catheter-Tubing Transducer System & Zeroing
(Buniyadi Usool, Setup aur Zero Karna)
PART 1 — ENGLISH EXPLANATION
Slide 1: Basic Principle
How Does the Whole System Work?
The core idea is a signal conversion chain — pressure → fluid → electrical signal → visual display:
Artery (pressure wave)
↓
Fluid column in tubing
↓
Pressure Transducer (converts pressure → electrical signal)
↓
Microprocessor (processes, amplifies)
↓
Monitor (visual waveform + numbers)
Step by step:
- The heart beats → creates a pressure waveform (a wave of pressure) in the artery
- This pressure wave travels through the fluid inside the tubing (fluid is incompressible, so it transmits the wave perfectly)
- The fluid pushes against the transducer diaphragm (a thin membrane inside the transducer)
- The transducer converts this mechanical pressure into an electrical signal
- The microprocessor processes and amplifies (makes stronger) this signal
- The monitor displays a visual waveform + digital numbers for systolic, diastolic, and MAP
Two things that determine accuracy:
| Factor | Why it matters |
|---|---|
| Transducer's precise positioning | If placed too high or too low, readings will be wrong (gravity affects fluid pressure) |
| System's effective dampening | Controls how faithfully the wave is reproduced — too much or too little dampening = false readings |
Slide 2: Catheter-Tubing Transducer System
The Complete Setup — Components from Left to Right:
![Full arterial line setup diagram]
| Component | What it is | Function |
|---|---|---|
| Catheter | Thin tube inside patient's artery | Senses arterial pressure directly |
| Stopcock | 3-way valve with a lever | Controls fluid flow; used to draw blood samples (ABG) |
| High-pressure tubing | Thick, rigid, non-stretchy tubing | Transmits pressure waves without absorbing or distorting them |
| Dome | Clear plastic fluid-filled chamber | Sits on top of transducer; fluid-filled interface between tubing and sensor |
| Transducer | Cylindrical sensor device | Converts pressure → electrical signal (Wheatstone bridge inside) |
| Flush pigtail | Small pull-tab on the dome | Used to flush the system with saline to clear air/blood clots |
| To pressurized flush solution | Tube going down to saline bag | Keeps fluid flowing at ~3 mL/hr to prevent catheter clotting |
| To monitor | Electrical cable | Carries electrical signal from transducer to bedside monitor |
Why must tubing be HIGH-pressure and non-compressible?
- Regular soft IV tubing would absorb the pressure wave instead of transmitting it
- This would cause overdamping → falsely low systolic, falsely high diastolic
- Rigid tubing faithfully transmits every pressure change
Why is the pressure bag needed?
- A pressure bag inflated to 300 mmHg surrounds the saline bag
- This maintains a constant slow flush (~3 mL/hr) through the catheter
- Prevents blood from backing up into the tubing and clotting the catheter
Slide 3: Zeroing the Stopcock for Lying Down (Supine) Position
What is "Zeroing"?
Zeroing means telling the monitor: "This is zero pressure (atmospheric pressure)" — so all readings are relative to this reference point.
If you don't zero correctly, every reading will be shifted up or down by the error.
The Phlebostatic Axis — Your Reference Point
The phlebostatic axis is the anatomical reference point that represents the level of the right atrium (the heart's right upper chamber):
Location: Intersection of the 4th intercostal space (4th rib gap) and the mid-axillary line (midpoint of the armpit line) on the side of the chest
This point is used because blood pressure is measured relative to the heart — not relative to the floor or the bed.
How to Zero Correctly (Supine Patient):
- Place the air-fluid interface (the zeroing stopcock port) at the exact level of the phlebostatic axis
- Use a Carpenter's level (a bubble-level tool) to confirm they are perfectly horizontal
- Open the stopcock to atmosphere (air)
- Press the "zero" button on the monitor
What Happens if Transducer is in Wrong Position?
| Error | Effect on Reading |
|---|---|
| Transducer too LOW (below heart level) | Reads falsely HIGH (extra fluid column weight adds to reading) |
| Transducer too HIGH (above heart level) | Reads falsely LOW (fluid column weight subtracts from reading) |
| Rule: Every 1 cm error = ~0.74 mmHg error |
The Complete System Diagram (Bottom Panel):
The full setup from top to bottom:
- Pressure bag (300 mmHg, on IV pole) → keeps flush flowing
- → Pressure transducer + flushing system (mounted on IV pole bracket)
- → Colour-coded non-compressible tubing (rigid, colour-coded so you don't confuse it with IV lines)
- → Sample port (red stopcock — for drawing ABG blood)
- → Arterial line catheter (in patient's radial artery at wrist)
- Transducer → cable → Monitor (shows waveform on screen)
⭐ EXAM TIPS
- Signal path order (very common MCQ): Artery → Fluid → Transducer → Electrical signal → Microprocessor → Monitor display
- Accuracy depends on TWO things: Transducer position + Effective dampening
- Phlebostatic axis = 4th ICS + mid-axillary line = level of right atrium — memorize this exactly
- Zeroing is always at phlebostatic axis for supine patients
- Transducer too low = falsely HIGH reading; transducer too high = falsely LOW reading
- High-pressure tubing = non-compressible — regular soft tubing causes overdamping
- Pressure bag inflated to 300 mmHg — maintains ~3 mL/hr slow flush
- Stopcock = used for blood sampling (ABG) — NOT for changing pressure settings
- Overdamping causes: underestimated systolic + overestimated diastolic (but MAP stays correct)
- Underdamping causes: overestimated systolic + underestimated diastolic (but MAP stays correct)
- MAP is always accurate regardless of damping — use MAP for clinical decisions
- Air bubbles in tubing → overdamping → must be removed immediately
- Flush pigtail = clears air/blood from dome — pull briefly, not continuously
PART 2 — ROMAN URDU WAZAHAT
Slide 1: Buniyadi Usool (Basic Principle)
Poora System Kaise Kaam Karta Hai?
Seedhi baat — yeh ek signal ka safar hai pressure se picture tak:
Artery (dil ki dhadkan se pressure)
↓
Tubing mein fluid (pani ka column)
↓
Transducer (pressure ko bijli ke signal mein badalta hai)
↓
Microprocessor (signal ko process aur amplify karta hai)
↓
Monitor (screen par waveform aur numbers)
Qadam ba qadam:
- Dil dhadhakta hai → artery mein ek pressure wave (dabao ki lahar) banti hai
- Yeh lahar tubing ke andar fluid (pani) ke zariye aage chalti hai — pani press nahi hota, isliye wave seedhi pahunchti hai
- Pani transducer diaphragm (patli jhilli) ko dhaka deta hai
- Transducer yeh mechanical dabao ko electrical signal (bijli ka ishara) mein badal deta hai
- Microprocessor (chhota computer) is signal ko process karke mazboot banata hai
- Monitor par visual waveform (lahron ki tasveer) + systolic, diastolic, MAP ke numbers dikhte hain
Sahi reading ke liye 2 cheezein zaruri hain:
| Cheez | Kyun Zaroori? |
|---|---|
| Transducer ki sahi jagah (precise positioning) | Agar upar ya neechay ho to reading galat aayegi |
| System ka sahi dampening | Wave theek se pohnche — zyada ya kam dampening = galat reading |
Slide 2: Catheter-Tubing Transducer System (Poora Setup)
Left se Right — Har Part ka Kaam:
| Part | Kya Hai | Kya Kaam Karta Hai |
|---|---|---|
| Catheter | Artery ke andar patli nali | Seedha artery ka pressure feel karta hai |
| Stopcock | Teen rasta wala valve (band/khulne wala) | Fluid control karta hai; khoon (ABG) nikalne ke liye use hota hai |
| High-pressure tubing | Mota, sakht, kam kheenchne wali nali | Pressure wave ko bina bigaade aage pahunchata hai |
| Dome | Saaf plastic ka fluid-bhra gumbad | Transducer ke upar baithta hai; fluid aur sensor ke beech ka waasta |
| Transducer | Sensor wala cylindrical (gol) aala | Pressure → Bijli ka signal banata hai |
| Flush pigtail | Dome par chota pull-tab | System ko saline se saaf karne ke liye — hawa ya khoon ki gaath hatata hai |
| To pressurized flush solution | Saline bag wali nali | Lagatar thodi thodi saline aati rehti hai — nali band na ho |
| To monitor | Bijli ki taar | Transducer se signal monitor tak pahunchati hai |
High-pressure tubing kyun zaruri hai?
- Aam naram IV nali pressure wave ko absorb (choos) kar leti hai
- Isse overdamping (zyada manda hona) hota hai → systolic galat kam, diastolic galat zyada
- Sakht nali wave ko seedha aur bina bigarey pahunchati hai
Pressure bag kyun lagaate hain?
- Pressure bag ko 300 mmHg tak inflate (phula) karte hain
- Isse saline lagatar ~3 mL/hr ki raftaar se catheter mein jaata rehta hai
- Isse catheter mein khoon wapas nahi aata aur clot (gaath) nahi banti
Slide 3: Zeroing (Sifar par Laana) — Leyte hue Mareed ke liye
Zeroing kya hoti hai?
Zeroing matlab monitor ko batana: "Yeh hai zero pressure" — taake baad ki saari readings is base se naapi jayein.
Agar zeroing sahi nahi — har reading upar ya neechay shift ho jaayegi — galat treatment ho sakta hai!
Phlebostatic Axis — Reference Point
Phlebostatic axis woh jagah hai jo right atrium (dil ka daaya upar wala kamra) ki level daraazti hai:
Jagah: Chaathi ki 4th intercostal space (chautha ribs ka darmiyana fark) aur mid-axillary line (bagal ki bich wali line) ka mila hua muqam
Hum isi jagah use karte hain kyunki BP hamesha dil ki level par naapna chahiye.
Sahi Zeroing Kaise Karein? (Leyte hue mareed mein)
- Air-fluid interface (zeroing stopcock ka khula sar) ko phlebostatic axis ki exact level par rakho
- Carpenter's level (bubble wala level tool) se confirm karo ke dono bilkul ek seedhi line mein hain
- Stopcock ko atmosphere (hawa) ki taraf kholo
- Monitor par "Zero" button dabao
Galat Position ka Asar:
| Galti | Reading par Asar |
|---|---|
| Transducer zyada neechay (dil se neechay) | Reading galat zyada (falsely high) aayegi |
| Transducer zyada upar (dil se upar) | Reading galat kam (falsely low) aayegi |
| Rule: Har 1 cm galti = 0.74 mmHg galti |
Poora System Ek Nazar Mein (Bottom Diagram):
Pressure bag (300 mmHg) — IV pole par
↓
Pressure transducer + flushing system
↓
Colour-coded non-compressible tubing (sakht, rang wali nali)
↓
Sample port (red stopcock — ABG lene ke liye)
↓
Arterial line catheter (radial artery mein — kalai par)
Transducer → Taar → Monitor (screen par waveform dikhta hai)
- Colour-coding (rang) kyon? Taake yeh nali aam IV drip ki nali se confuse na ho — arterial line mein galti se dawa nahi daalni
- Sample port woh jagah hai jahan se bina needle ke baar baar khoon (ABG) nikalte hain
⭐ EXAM TIPS — Roman Urdu Mein
- Signal ka safar yaad karo: Artery → Fluid → Transducer → Bijli → Microprocessor → Monitor
- Accuracy ke liye 2 cheezein: Transducer ki jagah + Dampening — dono exam mein aate hain
- Phlebostatic axis = 4th ICS + mid-axillary line = Right Atrium ki level — yeh definition ratta lagao
- Zeroing = phlebostatic axis par — leyte hue mareed ke liye
- Transducer neechay = reading zyada; Transducer upar = reading kam — yeh seedha logic hai
- High-pressure tubing = sakht = overdamping nahi hogi — naram nali = overdamping = galat reading
- 300 mmHg pressure bag — slow flush ke liye — clot rokne ke liye
- Overdamping (zyada manda) → systolic kam, diastolic zyada aata hai → MAP theek rehta hai
- Underdamping (zyada bounce) → systolic zyada, diastolic kam → MAP theek rehta hai
- MAP hamesha sahi rehta hai — damping ka MAP par asar nahi padta
- Air bubbles = overdamping — tubing mein hawa bilkul nahi honi chahiye
- Flush pigtail = saaf karna — zaroorat par, hamesha nahi
PART 3 — DIFFICULT WORDS KI DEFINITIONS
(Roman Urdu Mein)
| Mushkil Lafz | Roman Urdu Definition |
|---|---|
| Pressure waveform | Dil ki har dhadkan se banne wali pressure ki lahar — monitor par ek undulating (hilti hui) line ke roop mein dikh ti hai |
| Transmitted | Ek jagah se doosri jagah pahunchaya gaya — yahan pressure wave fluid ke zariye aage jaati hai |
| Fluid column | Tubing ke andar pani ka thamb (khari lambai) — pressure is ke zariye transducer tak pahunchta hai |
| Transducer | Aik aisa aala jo ek qism ki energy ko doosri mein badalta hai — yahan pressure (mechanical) ko bijli (electrical) mein |
| Electrical signal | Bijli ka chota ishara/wave — yeh signal monitor tak jaata hai aur reading banata hai |
| Microprocessor | Ek bohat chhota computer chip jo signal ko receive, process, aur amplify karta hai |
| Amplified | Mazboot banana — kamzor signal ko zyada taqatwar banana taake monitor par saaf dikhe |
| Accuracy | Sahi hona — reading asli value ke kitni qareeb hai |
| Contingent upon | Depend karna — is cheez par mauqoof hona |
| Precise positioning | Bilkul sahi jagah par rakhna — zyada ya kam nahi |
| Effective dampening | Sahi miqdar mein signal ko slow karna — na zyada na kam |
| Stopcock | Teen rasta wala valve — ek taraf se khoon/fluid aata hai, doosri se jaata hai, teesri se band kar sakte hain |
| High-pressure tubing | Sakht, mota, non-compressible (nahi kheenchne wali) nali — pressure wave ko bina absorb kiye aage pahunchaati hai |
| Dome | Gumbad numan saaf plastic ka hissa — transducer ke upar fluid-filled chamber |
| Flush pigtail | Chota pull-tab — system ko saline se saaf karne ke liye |
| Pressurized flush solution | 300 mmHg pressure par rakha saline bag — catheter ko saaf aur open rakhta hai |
| Zeroing | Monitor ko "zero" batana — atmosphere (hawa ke pressure) ko reference point banana |
| Phlebostatic axis | 4th intercostal space aur mid-axillary line ka mila hua muqam — right atrium (dil ke kamre) ki level |
| Air-fluid interface | Stopcock ka woh hissa jahan hawa aur fluid milte hain — zeroing ke waqt yahan se zero karte hain |
| Carpenter's level | Ek aam tool jisme bubble hota hai — do cheezon ko bilkul ek hi horizontal level par confirm karne ke liye |
| Supine position | Seedha lait kar — peeth ke bal — yeh zeroing ki standard position hai |
| Colour-coded tubing | Rang se pahchani wali nali — taake arterial line ko IV line se ghalta na milayein |
| Sample port | Khoon nikalne ki jagah — yahan se ABG test ke liye baar baar sample lete hain bina needle ke |
| Right atrium | Dil ka daaya upar wala kamra — phlebostatic axis isi ki level dikhata hai |
| Non-compressible | Nahi dabne wala — pressure wave isko absorb nahi kar sakti — isliye ye tubing zyada sakht hoti hai |
| Overdamping | Signal zyada mand ho jaata hai — waveform flat — systolic galat kam aata hai |
| Underdamping | Signal zyada bounce karta hai — waveform spike wali — systolic galat zyada aata hai |
Sources: Fischer's Mastery of Surgery, 8e | Morgan & Mikhail's Clinical Anesthesiology, 7e | Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.