Gluconeogenesis
Reading File
Finding Sources
Searching the Web
gluconeogenesis pathway steps regulation biochemistry
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete breakdown of gluconeogenesis, drawn from Lippincott's Illustrated Reviews: Biochemistry (8th ed.) and Basic Medical Biochemistry: A Clinical Approach (6th ed.).
Gluconeogenesis
Overview
Gluconeogenesis is the synthesis of glucose from non-carbohydrate precursors. It is the body's primary mechanism for maintaining blood glucose during fasting, starvation, and prolonged exercise. Tissues that absolutely depend on glucose - the brain, erythrocytes, kidney medulla, lens and cornea, testes, and exercising skeletal muscle - cannot synthesize it on their own.
- Primary site: Liver (~90% during overnight fast)
- Secondary site: Kidney cortex (~10% normally; increases to ~40% after 48+ hours of fasting)
- Minor contributor: Small intestine
After ~24 hours of fasting, hepatic glycogen stores are exhausted and gluconeogenesis becomes the sole source of blood glucose.
- Biochemistry, Lippincott Illustrated Reviews 8e, p. 353
Substrates (Gluconeogenic Precursors)
| Precursor | Source | Entry Point |
|---|---|---|
| Lactate | Anaerobic glycolysis in muscle/RBCs | Converted to pyruvate (Cori cycle) |
| Alanine & glucogenic amino acids | Muscle protein hydrolysis | Transaminated to pyruvate or TCA intermediates |
| Glycerol | TAG hydrolysis in adipose tissue | Glycerol 3-phosphate → DHAP |
| Propionate | Odd-chain fatty acid oxidation | Succinyl-CoA → OAA |
Key limitation: Acetyl-CoA and purely ketogenic amino acids (leucine and lysine) cannot serve as gluconeogenic precursors because the pyruvate dehydrogenase complex (PDH) reaction is irreversible - there is no net synthesis of OAA from acetyl-CoA.
The Three Irreversible Bypass Reactions
Gluconeogenesis uses 7 of the 10 glycolytic enzymes (running in reverse), but must bypass the 3 irreversible steps of glycolysis using 4 unique enzymes.
Bypass 1: Pyruvate → PEP (bypasses Pyruvate Kinase)
This is a two-step process spanning the mitochondria and cytosol:
Step 1 - Pyruvate Carboxylase (mitochondria)
- Pyruvate + CO₂ + ATP → Oxaloacetate (OAA)
- Cofactor: Biotin (covalently bound to enzyme)
- Allosterically activated by acetyl-CoA (signals that energy is available but TCA is saturated)
Step 2 - PEPCK - PEP Carboxykinase (cytosol)
- OAA + GTP → PEP + CO₂ + GDP
- OAA cannot cross the mitochondrial membrane, so it is first reduced to malate (by mitochondrial malate dehydrogenase), transported out, then re-oxidized to OAA in the cytosol before PEPCK acts
- This shuttle also transfers NADH (reducing equivalents) from mitochondria to cytosol, which is needed for a later step
Bypass 2: Fructose 1,6-bisphosphate → Fructose 6-phosphate (bypasses PFK-1)
- Fructose 1,6-bisphosphatase (FBPase-1)
- Fructose 1,6-bisphosphate + H₂O → Fructose 6-phosphate + Pᵢ
- Inhibited by: AMP, fructose 2,6-bisphosphate
- Activated by: citrate
Bypass 3: Glucose 6-phosphate → Glucose (bypasses Hexokinase/Glucokinase)
- Glucose 6-phosphatase (ER membrane enzyme)
- Glucose 6-phosphate + H₂O → Glucose + Pᵢ
- Present in liver and kidney only (not muscle or brain, which is why they cannot export glucose)
Pathway Diagram
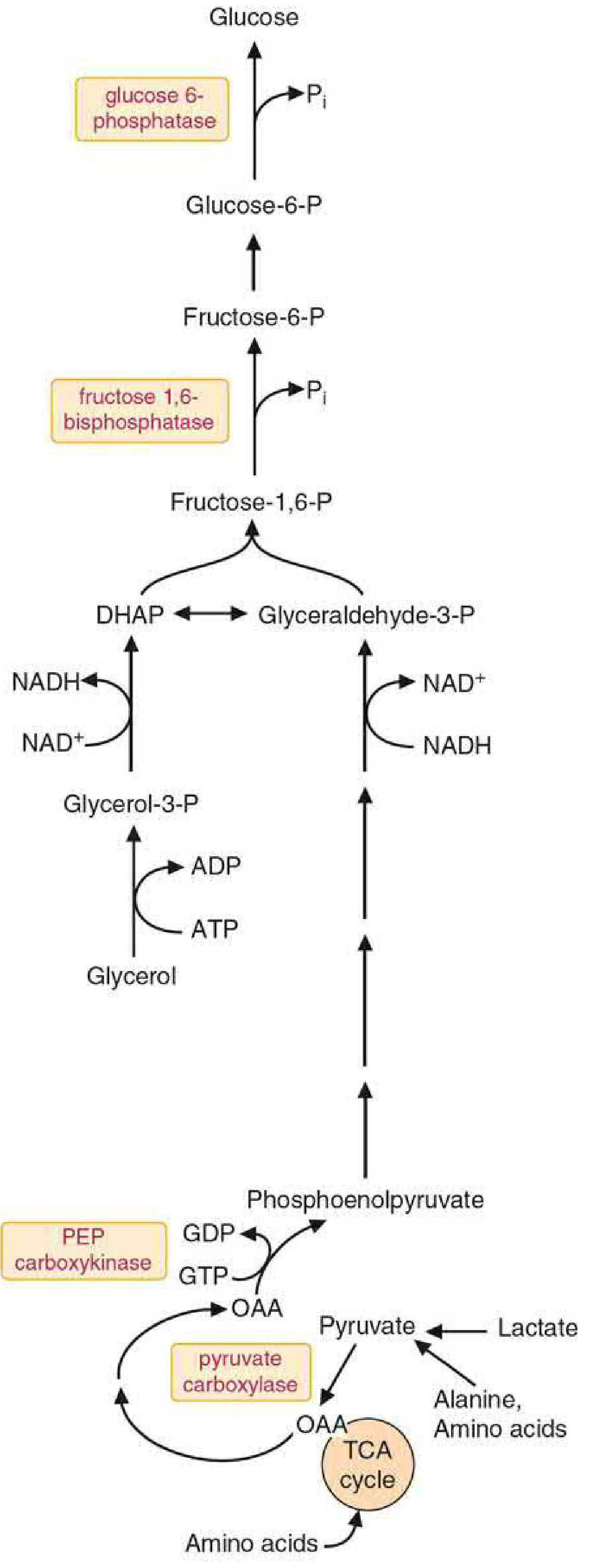
Gluconeogenesis pathway - the 4 unique enzymes (pyruvate carboxylase, PEPCK, FBPase-1, glucose 6-phosphatase) are highlighted in boxes. - Basic Medical Biochemistry, 6e, Fig. 28.3
Energy Cost of Gluconeogenesis
Synthesizing 1 molecule of glucose from 2 pyruvate costs:
4 ATP + 2 GTP + 2 NADH (compared to glycolysis, which yields 2 ATP)
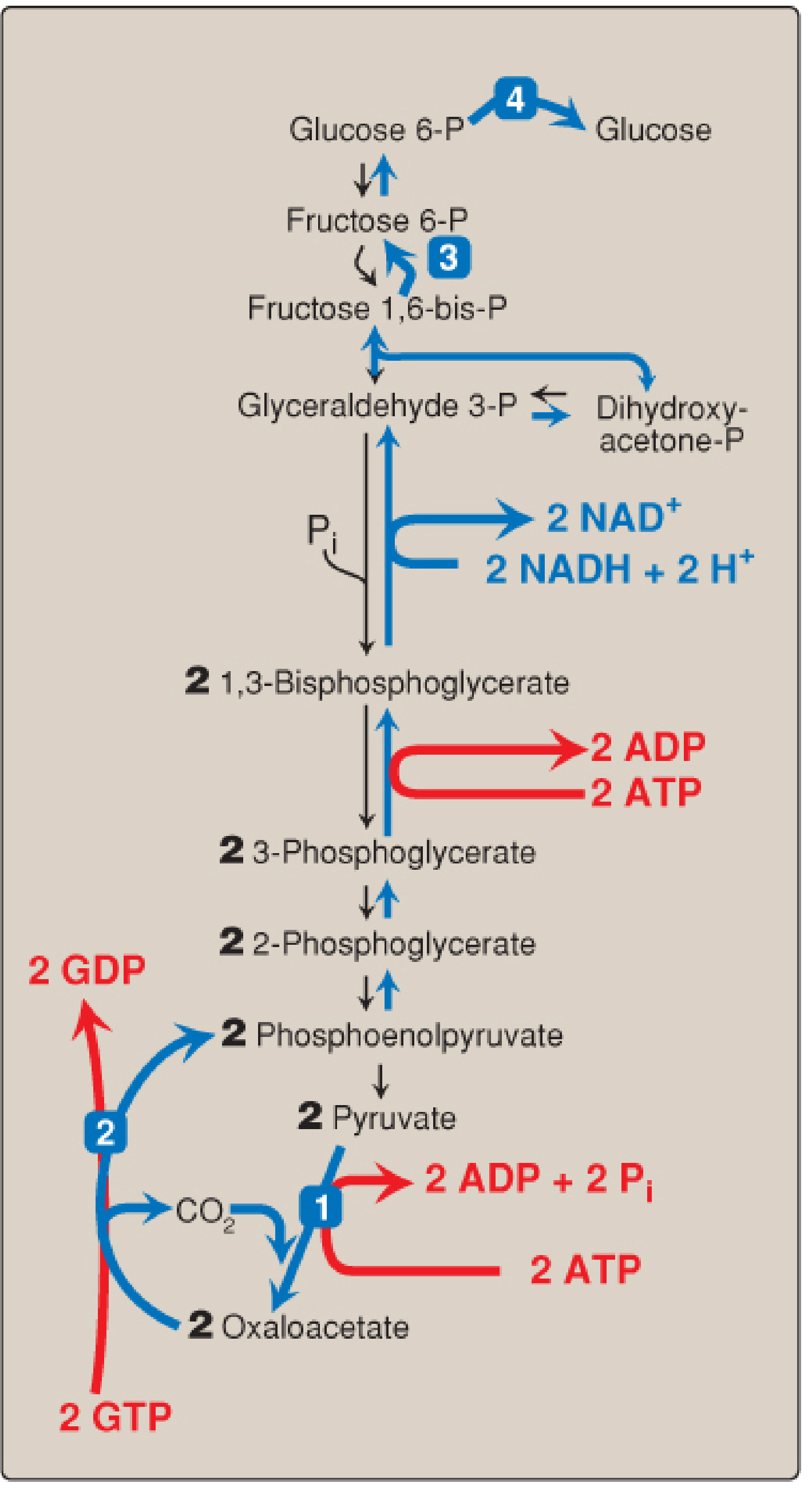
Numbered reactions (1-4) are unique to gluconeogenesis. Red arrows show energy inputs. - Lippincott Biochemistry 8e, Fig. 10.7
This energy is supplied primarily by beta-oxidation of fatty acids in the liver during fasting.
The Cori Cycle
A key inter-organ relationship:
- Exercising muscle/RBCs produce lactate via anaerobic glycolysis
- Lactate travels via blood to the liver
- Liver converts lactate → pyruvate → glucose
- Glucose travels back to muscle/RBCs
This recycles lactate into usable glucose but transfers the metabolic burden (ATP cost) from peripheral tissues to the liver.
Regulation
Hormonal
| Hormone | Effect | Mechanism |
|---|---|---|
| Glucagon | Stimulates ↑ | Lowers fructose 2,6-bisphosphate (activates FBPase-1); phosphorylates/inactivates pyruvate kinase; increases PEPCK transcription via CREB |
| Insulin | Inhibits ↓ | Increases fructose 2,6-bisphosphate (inhibits FBPase-1); decreases PEPCK gene expression |
| Cortisol | Stimulates ↑ | Mobilizes amino acids from muscle protein; increases PEPCK gene expression |
| Epinephrine | Stimulates ↑ | Similar cAMP-mediated mechanism to glucagon |
Allosteric
| Effector | Target | Effect |
|---|---|---|
| Acetyl-CoA | Pyruvate carboxylase | Activates (signals excess fatty acid oxidation) |
| Acetyl-CoA | PDH kinase | Activates → inhibits PDH → diverts pyruvate toward gluconeogenesis |
| AMP | FBPase-1 | Inhibits (reciprocal with PFK-1 activation by AMP) |
| Fructose 2,6-bisphosphate | FBPase-1 | Inhibits |
| Citrate | FBPase-1 | Activates |
Substrate Availability
Decreased insulin during fasting promotes muscle protein catabolism, flooding the liver with glucogenic amino acids. Fatty acid oxidation provides the ATP and NADH required for gluconeogenesis to proceed.
Clinical Relevance
| Condition | Connection |
|---|---|
| Type 2 diabetes | Hepatic gluconeogenesis is inappropriately elevated, contributing to fasting hyperglycemia |
| Metformin (first-line T2DM drug) | Inhibits Complex I of mitochondrial ETC → raises AMP/ATP ratio → activates AMPK → inhibits gluconeogenesis |
| Biotin deficiency | Impairs pyruvate carboxylase → hypoglycemia |
| Deficiency of FBPase-1 or glucose 6-phosphatase | Severe fasting hypoglycemia |
| Glucagonoma | Excess glucagon → uncontrolled gluconeogenesis → hyperglycemia |
| DKA | Excess glucagon + cortisol drive gluconeogenesis, worsening hyperglycemia alongside ketogenesis |
| Alcohol intoxication | Ethanol oxidation generates excess NADH → depletes OAA and pyruvate → impairs gluconeogenesis → hypoglycemia |
Summary Table: Glycolysis vs. Gluconeogenesis Bypass Points
| Glycolysis Enzyme | Direction | Gluconeogenesis Bypass |
|---|---|---|
| Pyruvate kinase | PEP → Pyruvate | Pyruvate carboxylase + PEPCK |
| PFK-1 | F6P → F1,6bP | Fructose 1,6-bisphosphatase |
| Hexokinase/Glucokinase | Glucose → G6P | Glucose 6-phosphatase |
Sources: Biochemistry, Lippincott Illustrated Reviews 8e; Basic Medical Biochemistry: A Clinical Approach 6e; Guyton and Hall Textbook of Medical Physiology
Circle of wilis
Reading File
Finding Sources
Searching the Web
circle of Willis anatomy components clinical significance
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Here is a comprehensive overview of the Circle of Willis, sourced from Neuroanatomy through Clinical Cases (3rd ed.), Medical Physiology, and Robbins Pathology.
Circle of Willis (Circulus Arteriosus Cerebri)
Overview
The Circle of Willis is an anastomotic ring of arteries located at the base of the brain, sitting in the subarachnoid space around the optic chiasm and the interpeduncular fossa. It connects the two major arterial systems supplying the brain:
- Anterior circulation - from the bilateral internal carotid arteries (ICAs)
- Posterior circulation - from the bilateral vertebral arteries (which join to form the basilar artery)
Its primary function is to provide collateral blood flow - if one vessel is occluded, blood can be rerouted through the ring to maintain perfusion. However, a complete, full-caliber ring is present in only approximately 34% of individuals; anatomical variants are the norm rather than the exception.
- Neuroanatomy through Clinical Cases, 3rd ed., p. 417
Diagram: Full Arterial Supply from Aorta to Circle of Willis
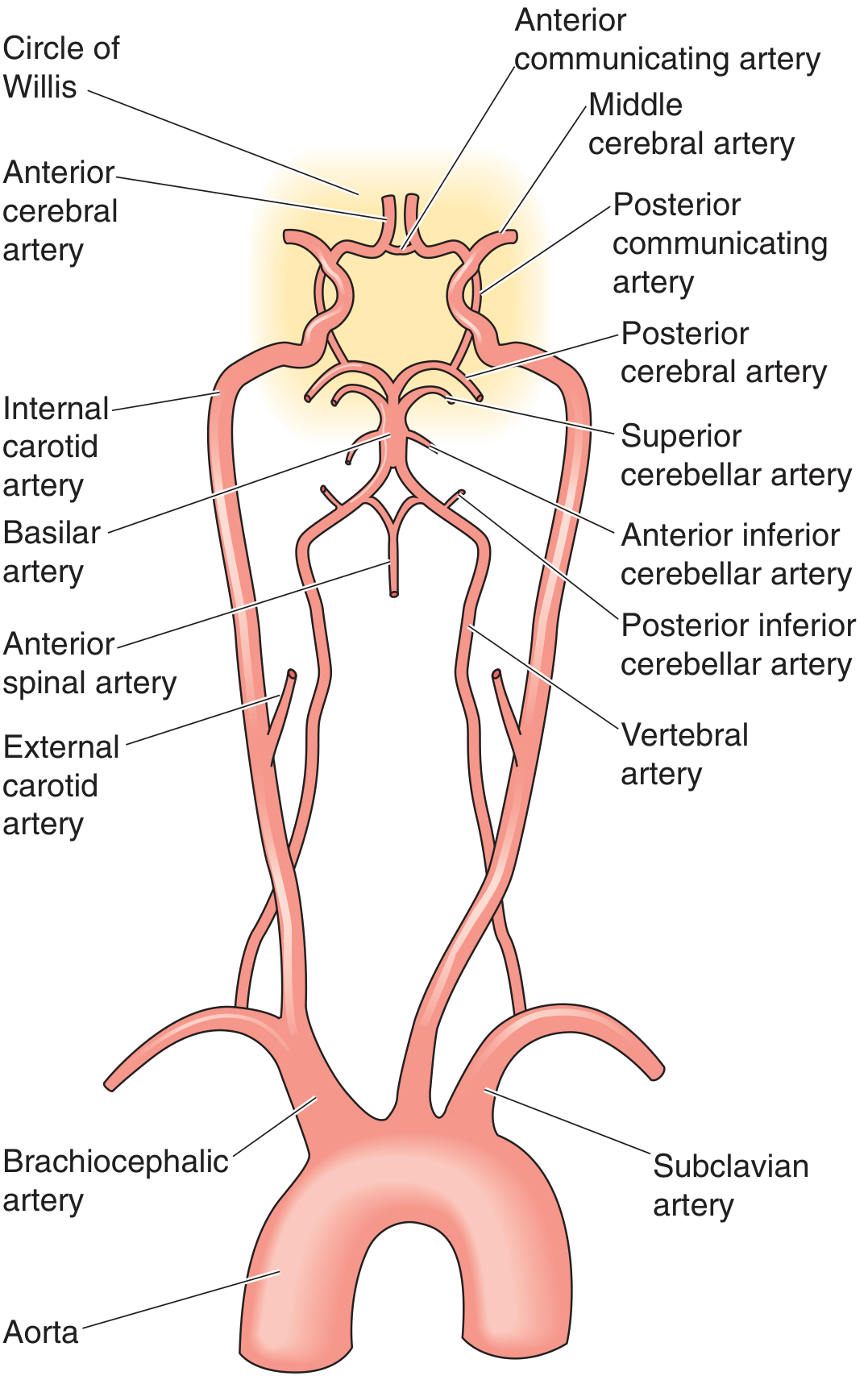
Vascular anatomy showing origin of anterior and posterior circulations - Medical Physiology
Components of the Circle of Willis
The circle is made up of 7 arteries arranged as an irregular heptagon around the base of the brain:
Anterior Part (from Internal Carotid Arteries)
| Vessel | Origin | Contribution |
|---|---|---|
| Anterior cerebral arteries (ACA) x2 | Terminal branches of ICA | Forms the anterior limbs of the ring |
| Anterior communicating artery (AComm) x1 | Connects the two ACAs | Closes the anterior portion of the ring |
| Middle cerebral arteries (MCA) x2 | Terminal branches of ICA | Not part of the ring itself; arise from the ICA at its bifurcation point |
| Internal carotid arteries (ICA) x2 | Common carotid → ICA | Supply the lateral portions of the ring |
Posterior Part (from Vertebrobasilar System)
| Vessel | Origin | Contribution |
|---|---|---|
| Posterior cerebral arteries (PCA) x2 | Terminal branches of basilar artery | Forms the posterior limbs of the ring |
| Posterior communicating arteries (PComm) x2 | Connect ICA to PCA | Bridges the anterior and posterior circulations - the "communicators" |
The AComm and the two PComms are the three communicating arteries of the circle - they are the segments that allow collateral flow between the two sides and between the anterior and posterior circulations.
Detailed Anatomy Diagram (Inferior View)
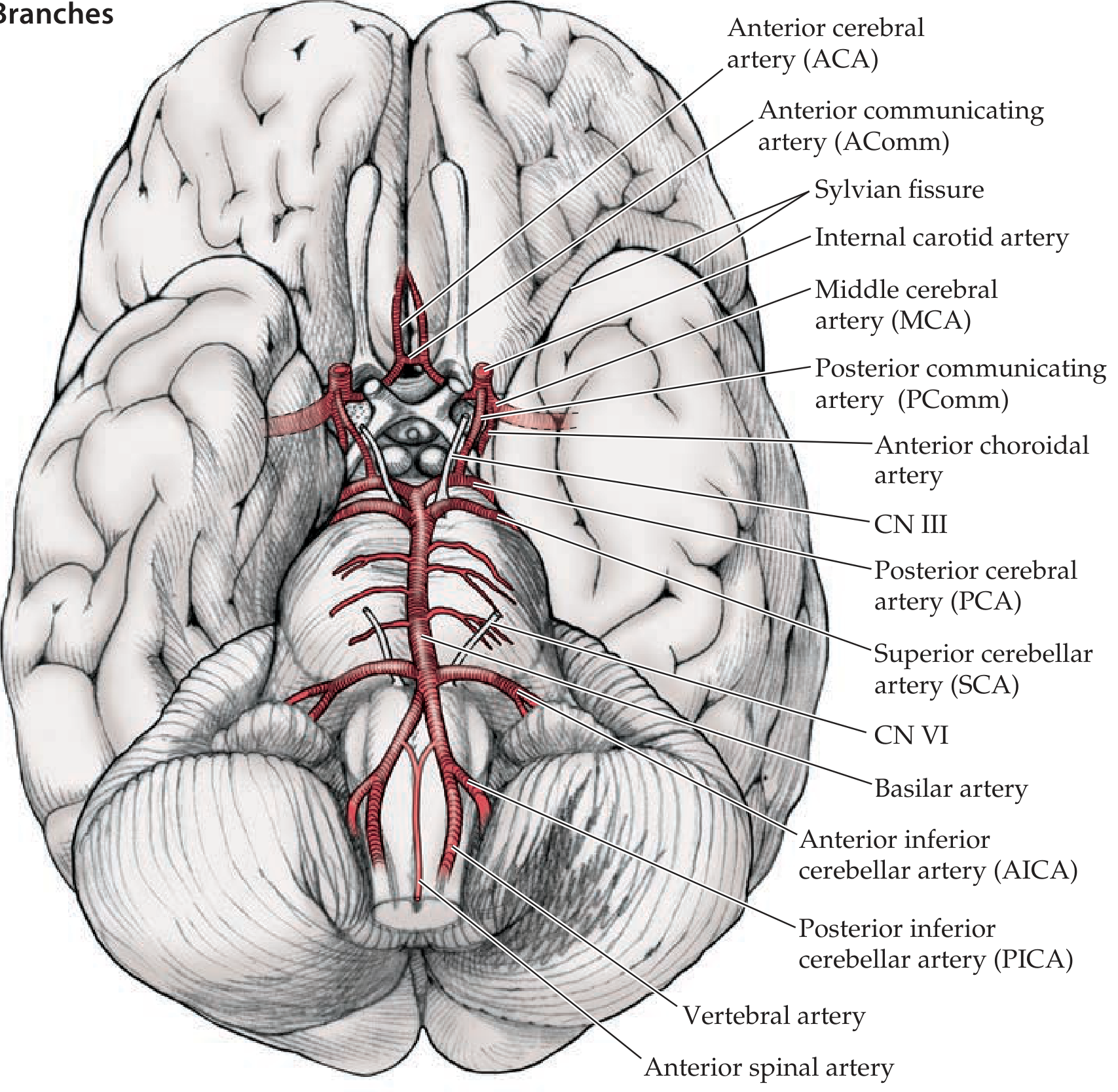
Circle of Willis and its main branches - inferior view of the brain. Note the relationship of CN III to the posterior communicating artery - Neuroanatomy through Clinical Cases, 3rd ed., Fig. 10.3
Feeding Vessels
Anterior circulation pathway:
Aorta → Brachiocephalic/Common carotid → Internal carotid artery → bifurcates into ACA + MCA
Posterior circulation pathway:
Aorta → Subclavian → Vertebral arteries (ascend through foramina transversaria of C1-C6) → enter foramen magnum → converge to form basilar artery → bifurcates at the pontomesencephalic junction into bilateral PCAs
Vascular Territories of the Three Main Cerebral Arteries
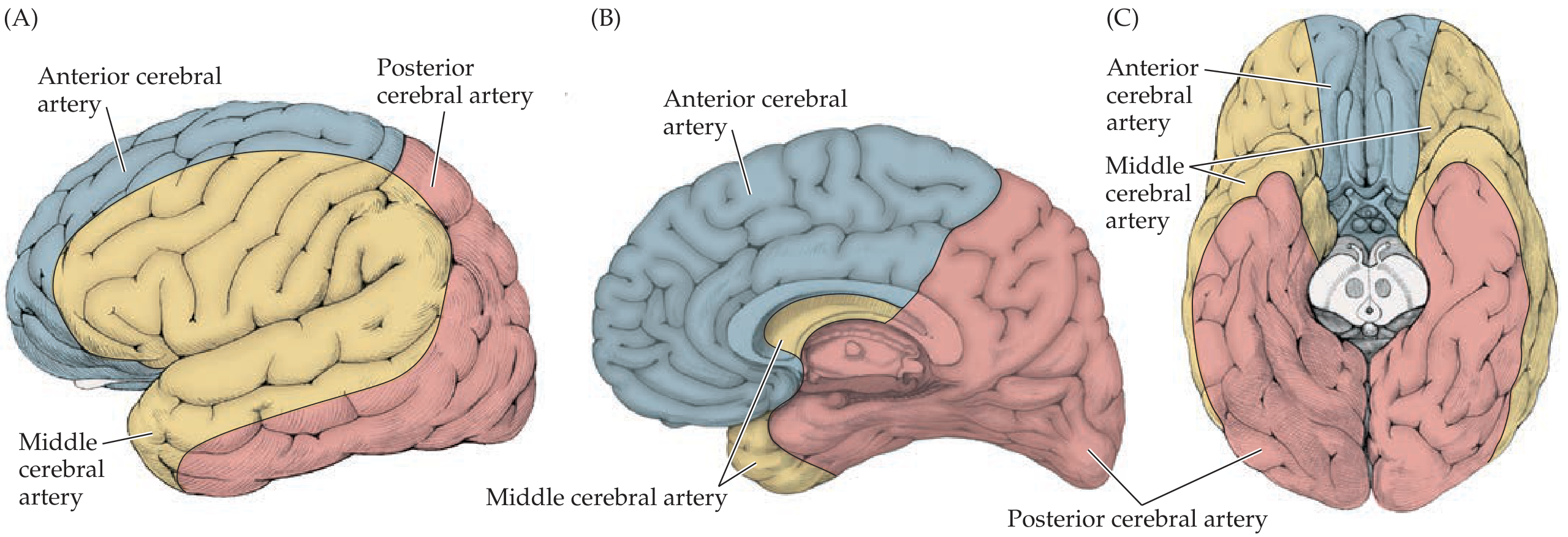
Cortical territories of ACA (blue), MCA (yellow/gold), and PCA (pink) - Neuroanatomy through Clinical Cases, 3rd ed., Fig. 10.5
| Artery | Territory | Key Clinical Deficit if Occluded |
|---|---|---|
| ACA | Medial frontal & parietal cortex, anterior corpus callosum | Contralateral leg weakness/sensory loss (medial homunculus) |
| MCA | Lateral cortex (frontal, parietal, temporal), internal capsule via lenticulostriate branches | Contralateral face + arm weakness, aphasia (dominant), neglect (non-dominant) |
| PCA | Occipital lobe, medial temporal lobe, thalamus | Contralateral homonymous hemianopia, memory deficits |
Deep Penetrating Branches
Arising near the circle of Willis are small perforating arteries that supply deep structures:
- Lenticulostriate arteries (from MCA) - supply basal ganglia, putamen, internal capsule
- Anterior choroidal artery (from ICA) - supplies posterior limb of internal capsule, hippocampus, choroid plexus
- Thalamoperforating arteries (from PCA/PComm) - supply thalamus
These small vessels are prone to hypertensive lacunar strokes.
Clinical Significance
1. Berry (Saccular) Aneurysms
The branch points of the Circle of Willis are the most common sites for intracranial saccular aneurysms, due to congenital deficiency of the elastic lamina at arterial bifurcations.
Common locations (in order of frequency):
- AComm / ACA junction (most common, ~35%)
- ICA / PComm junction (~30%) - classically causes CN III palsy due to compression of the nerve running adjacent to PComm
- MCA bifurcation in the Sylvian fissure (~20%)
- Basilar tip (~5-10%)
Rupture → subarachnoid hemorrhage (SAH) → "worst headache of life," meningismus, xanthochromia on LP
2. Stroke and Occlusion Syndromes
Occlusion at or near the circle produces predictable deficits based on the territory involved (see table above). The completeness of the circle determines how much collateral compensation is possible.
3. CN III Palsy - "Surgical Third Nerve Palsy"
A PComm aneurysm expands and compresses CN III as it runs parallel to it. This produces:
- Ptosis
- "Down and out" eye position
- Dilated, unreactive (blown) pupil - the hallmark that distinguishes compressive (surgical) from ischemic (medical) CN III palsy
4. Anatomical Variations
Only ~34% of people have a complete ring. Common variants:
- Hypoplastic or absent PComm (most common, ~20%) - reduces posterior-anterior collateral capacity
- Fetal-type PCA - PCA arises directly from ICA rather than basilar (present in ~20-30%) - means PCA territory becomes vulnerable if ICA is occluded
5. Collateral Flow
If the ICA is gradually occluded (e.g., atherosclerosis), a complete Circle of Willis allows the contralateral ICA or the vertebrobasilar system to compensate via the communicating arteries, potentially preventing stroke.
Sources: Neuroanatomy through Clinical Cases 3rd ed.; Medical Physiology (Boron & Boulpaep); Robbins Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.