ABG analysis from basic to clinical
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete ABG guide.
Arterial Blood Gas (ABG) Analysis: Basic to Clinical
1. What Is an ABG?
An arterial blood gas (ABG) measures the partial pressures of oxygen and carbon dioxide, pH, and bicarbonate in blood drawn from an artery (usually the radial). It reports gas exchange after the lungs and before peripheral tissue oxygen consumption. Blood gas analyzers directly measure pH, PaCO₂, and PaO₂; bicarbonate (HCO₃⁻) is calculated from the Henderson-Hasselbalch equation.
The ABG often includes additional values: serum lactate, total hemoglobin, and sometimes electrolytes - though results should be compared with reference lab values when significantly abnormal.
- Tintinalli's Emergency Medicine, p. 121
2. Normal Values
| Parameter | Normal Value |
|---|---|
| pH | 7.35 - 7.45 (mean 7.40) |
| PaCO₂ | 35 - 45 mm Hg (mean 40) |
| HCO₃⁻ | 22 - 26 mEq/L (mean 24) |
| PaO₂ | 75 - 100 mm Hg |
| SaO₂ | ≥95% |
| Base Excess (BE) | -2 to +2 mEq/L |
| A-a gradient | <10 mm Hg (on room air) |
3. The Henderson-Hasselbalch Equation
The relationship between pH, bicarbonate, and CO₂ is:
pH = 6.1 + log ( [HCO₃⁻] / 0.03 × PaCO₂ )
- The lungs regulate CO₂ (respiratory component) - rapidly, within minutes
- The kidneys regulate HCO₃⁻ (metabolic component) - slowly, over 3-5 days
The body always tries to bring pH back toward 7.40, but compensation is never complete.
4. The Four Primary Disorders
| Disorder | pH | Primary Change | Compensation |
|---|---|---|---|
| Metabolic acidosis | ↓ | ↓ HCO₃⁻ | ↓ PaCO₂ (hyperventilation) |
| Metabolic alkalosis | ↑ | ↑ HCO₃⁻ | ↑ PaCO₂ (hypoventilation) |
| Respiratory acidosis | ↓ | ↑ PaCO₂ | ↑ HCO₃⁻ (renal retention) |
| Respiratory alkalosis | ↑ | ↓ PaCO₂ | ↓ HCO₃⁻ (renal excretion) |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, p. 1157
5. Compensation Formulas (Winters' and Others)
These formulas check whether the compensation is appropriate. If it falls outside the predicted range, a mixed disorder is present.
Metabolic Disorders
| Primary | Expected Compensation |
|---|---|
| Metabolic acidosis | ↓PaCO₂ = 1.3 × ↓HCO₃⁻ |
| Metabolic alkalosis | ↑PaCO₂ = 0.6 × ↑HCO₃⁻ |
Winter's Formula (for metabolic acidosis):
Expected PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2
Quick trick: in pure metabolic acidosis, PaCO₂ approximates the last two digits of pH (e.g., pH 7.23 → expected PaCO₂ ≈ 23 mm Hg).
Respiratory Disorders
| Primary | Time | HCO₃⁻ Change |
|---|---|---|
| Respiratory acidosis | Acute | +1 mEq/L per 10 mm Hg ↑ PaCO₂ |
| Respiratory acidosis | Chronic | +4 mEq/L per 10 mm Hg ↑ PaCO₂ |
| Respiratory alkalosis | Acute | -2 mEq/L per 10 mm Hg ↓ PaCO₂ |
| Respiratory alkalosis | Chronic | -5 mEq/L per 10 mm Hg ↓ PaCO₂ |
If the measured PaCO₂ is higher than predicted by Winter's formula in metabolic acidosis → concomitant respiratory acidosis. Normocapnia with severe metabolic acidosis may signal impending respiratory failure and need for ventilation.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1734-1735
6. The Acid-Base Map
This diagram (from National Kidney Foundation Primer on Kidney Diseases, 8e) plots all six disorders with their 95% confidence compensation zones. Points outside these zones indicate a mixed disorder:
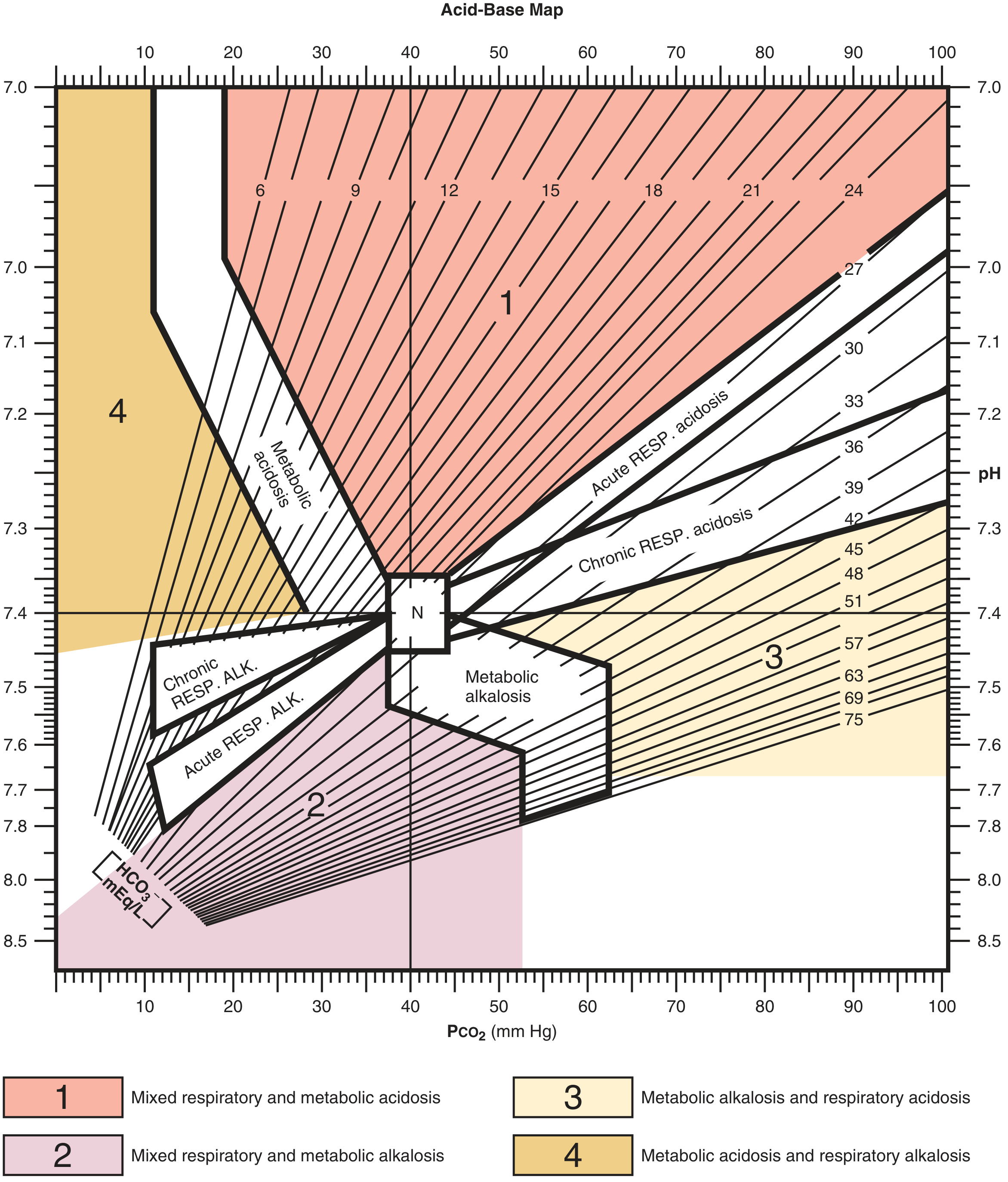
Figure: Acid-Base Map. Zone 1 = mixed respiratory + metabolic acidosis; Zone 2 = mixed respiratory + metabolic alkalosis; Zone 3 = metabolic alkalosis + respiratory acidosis; Zone 4 = metabolic acidosis + respiratory alkalosis. "N" marks the normal point (pH 7.40, PaCO₂ 40 mm Hg).
7. Step-by-Step ABG Interpretation (6-Step Method)
Step 1 - Determine acidemia or alkalemia
- pH < 7.35 = acidemia
- pH > 7.45 = alkalemia
Step 2 - Identify the primary process
- pH ↓ + PaCO₂ ↑ = respiratory acidosis
- pH ↓ + PaCO₂ ↓ = metabolic acidosis
- pH ↑ + PaCO₂ ↓ = respiratory alkalosis
- pH ↑ + PaCO₂ ↑ = metabolic alkalosis
Step 3 - Check compensation
Apply the formulas above. If actual compensation differs significantly from expected → mixed disorder.
Step 4 - Calculate the Anion Gap (AG)
AG = Na⁺ - (Cl⁻ + HCO₃⁻)
- Normal: 8-12 mEq/L
- The AG reflects unmeasured anions (albumin, phosphate, sulfate, organic acids)
- Correct for albumin: AG falls ~2.5 mEq/L for every 1 g/dL drop in albumin below normal
Step 5 - If non-anion gap acidosis: Urine Anion Gap
Urine AG = Urine (Na⁺ + K⁺ - Cl⁻)
- Negative urine AG → GI bicarbonate loss (diarrhea)
- Positive urine AG → renal bicarbonate loss (renal tubular acidosis)
Step 6 - Delta-Delta Ratio (ΔΔ) for High AG Metabolic Acidosis
ΔΔ = ΔAG / ΔHCO₃⁻ (change from normal values)
-
ΔΔ < 1.0 → mixed high AG + non-AG metabolic acidosis
-
ΔΔ 1.0-2.0 → pure high AG metabolic acidosis
-
ΔΔ > 2.0 → high AG metabolic acidosis + concurrent metabolic alkalosis (or chronic respiratory acidosis with compensation)
-
Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, p. 1158-1159
8. Causes of High Anion Gap Metabolic Acidosis
Use the mnemonic MUDPILE CAT (or GOLDMARK):
MUDPILE CAT:
- M - Methanol / Metformin
- U - Uremia
- D - Diabetic ketoacidosis
- P - Paraldehyde / Phenformin
- I - Isoniazid / Iron
- L - Lactate
- E - Ethylene glycol
- C - Carbon monoxide / Cyanide
- A - Alcoholic ketoacidosis
- T - Toluene
GOLDMARK (alternative): Glycols, Oxoproline (acetaminophen), L-Lactate, D-Lactate, Methanol, Aspirin, Renal failure, Ketoacidosis
- Roberts and Hedges', p. 1749; National Kidney Foundation Primer, p. 150
9. Non-Anion Gap (Hyperchloremic) Metabolic Acidosis
When HCO₃⁻ falls but AG stays normal, Cl⁻ must rise. Causes include:
- Diarrhea (GI bicarbonate loss)
- Renal tubular acidosis (types 1, 2, 4)
- Normal saline infusion (hyperchloremic dilutional acidosis)
- Bladder reconstruction / urinary diversions
- Acetazolamide
10. Oxygenation on the ABG
The ABG assesses not just acid-base but also oxygenation:
PaO₂ and Hypoxemia
- PaO₂ < 60 mm Hg (or SaO₂ < 90%) = hypoxemia = Type 1 respiratory failure
- Type 2 respiratory failure = hypercapnia (PaCO₂ > 45) ± hypoxemia
The Alveolar-Arterial (A-a) Gradient
A-a gradient = PAO₂ - PaO₂
PAO₂ (alveolar PO₂) = FiO₂ × (760 - 47) - (PaCO₂ / 0.8)
On room air at sea level: PAO₂ ≈ 148 - (PaCO₂ × 1.2)
- Normal A-a gradient: < 10 mm Hg (increases with age: ≈ age/4 mm Hg is a useful rule)
Five Mechanisms of Hypoxemia
| Mechanism | A-a Gradient | Response to O₂ |
|---|---|---|
| Hypoventilation | Normal | Improves |
| Right-to-left shunt | Elevated | Minimal/none |
| V/Q mismatch | Elevated | Improves |
| Diffusion impairment | Elevated | Improves |
| Low inspired O₂ | Normal | Improves |
A hallmark of significant right-to-left shunting is failure of PaO₂ to rise with supplemental oxygen.
- Tintinalli's Emergency Medicine, p. 467-468
11. Worked Clinical Examples
Example 1 - Metabolic Acidosis (Diarrhea)
Patient: 58-year-old woman, 1 week of diarrhea
- Na⁺ 133, K⁺ 2.8, Cl⁻ 118, pH 7.26, PaCO₂ 13, HCO₃⁻ 5
Step 1: pH 7.26 → acidemia
Step 2: PaCO₂ low (13), HCO₃⁻ low (5) → metabolic acidosis
Step 3: Expected ΔPaCO₂ = 1.3 × (25-5) = 26 → predicted PaCO₂ = 40-26 = 14 ✓ (actual = 13, appropriate compensation)
Step 4: AG = 133 - (118+5) = 10 → normal AG → hyperchloremic metabolic acidosis from diarrhea
Step 2: PaCO₂ low (13), HCO₃⁻ low (5) → metabolic acidosis
Step 3: Expected ΔPaCO₂ = 1.3 × (25-5) = 26 → predicted PaCO₂ = 40-26 = 14 ✓ (actual = 13, appropriate compensation)
Step 4: AG = 133 - (118+5) = 10 → normal AG → hyperchloremic metabolic acidosis from diarrhea
Example 2 - Respiratory Alkalosis (Sepsis)
Patient: 74-year-old, urosepsis (E. coli), hypotension, fever
- Na⁺ 138, K⁺ 3.2, Cl⁻ 105, pH 7.49, PaCO₂ 25, HCO₃⁻ 22
Step 1: pH 7.49 → alkalemia
Step 2: PaCO₂ 25 (low), HCO₃⁻ 22 (normal/slightly low) → respiratory alkalosis
Step 3: ΔPaCO₂ = 15 mm Hg; expected ΔHCO₃⁻ = 2 mEq/L per 10 mm Hg drop = 3 mEq/L → predicted HCO₃⁻ = 25-3 = 22 ✓ (appropriate compensation = acute respiratory alkalosis)
Step 2: PaCO₂ 25 (low), HCO₃⁻ 22 (normal/slightly low) → respiratory alkalosis
Step 3: ΔPaCO₂ = 15 mm Hg; expected ΔHCO₃⁻ = 2 mEq/L per 10 mm Hg drop = 3 mEq/L → predicted HCO₃⁻ = 25-3 = 22 ✓ (appropriate compensation = acute respiratory alkalosis)
Example 3 - Anion Gap Acidosis (Ethylene Glycol)
Patient: Antifreeze ingestion
- Na⁺ 144, K⁺ 3.1, Cl⁻ 108, HCO₃⁻ 14
AG = 144 - (108 + 14) = 22 → elevated → high AG metabolic acidosis, likely ethylene glycol
→ Also check osmolal gap = measured Osm - [2×Na + BUN/2.8 + Glucose/18] (normally <10 mOsm/kg; elevated in toxic alcohol ingestion)
→ Also check osmolal gap = measured Osm - [2×Na + BUN/2.8 + Glucose/18] (normally <10 mOsm/kg; elevated in toxic alcohol ingestion)
- Roberts and Hedges', p. 1733-1735
12. Mixed Acid-Base Disorders
A mixed disorder is present when compensation falls outside expected ranges, or when the ABG values fall in the numbered zones of the acid-base map. Common clinical combinations:
| Combination | Clinical Setting |
|---|---|
| Metabolic acidosis + respiratory alkalosis | Salicylate poisoning, sepsis, liver failure |
| Metabolic acidosis + respiratory acidosis | Cardiopulmonary arrest, severe COPD exacerbation |
| Metabolic alkalosis + respiratory acidosis | COPD with diuretic use, vomiting |
| Metabolic alkalosis + respiratory alkalosis | Liver failure + vomiting, or post-correction of chronic hypercapnia |
- Harrison's Principles of Internal Medicine 22E, block 6
13. Venous vs. Arterial Blood Gas
An arterial sample is the reference standard for all parameters. Venous samples are widely used in emergencies:
-
Venous pH correlates closely with arterial (within ±0.05 units)
-
Venous CO₂ trends with arterial but varies (up to ±20 mm Hg)
-
Normal venous CO₂ is predictive of a normal PaCO₂
-
Venous PO₂ cannot be used to assess oxygenation - it reflects tissue extraction, not lung function
-
Tintinalli's Emergency Medicine, p. 121
14. Clinical Red Flags on ABG
| Finding | Significance |
|---|---|
| Normal or elevated PaCO₂ with severe metabolic acidosis | Respiratory muscle fatigue, impending respiratory failure → consider intubation |
| pH < 7.10 | Severe acidemia; risk of cardiac arrhythmia, vasodilation, reduced myocardial contractility |
| Rising PaCO₂ on serial ABGs in asthma | Status asthmaticus - patient tiring, ICU needed |
| A-a gradient normal with hypoxemia | Hypoventilation or high altitude; not intrinsic lung disease |
| Hypoxemia refractory to high FiO₂ | Significant right-to-left shunt (ARDS, intracardiac defect) |
Quick Reference Summary
pH < 7.35 → Acidemia pH > 7.45 → Alkalemia
PaCO₂ ↑ + pH ↓ → Resp acidosis PaCO₂ ↓ + pH ↑ → Resp alkalosis
HCO₃⁻ ↓ + pH ↓ → Met acidosis HCO₃⁻ ↑ + pH ↑ → Met alkalosis
AG = Na⁺ - (Cl⁻ + HCO₃⁻) | Normal: 8-12
Winter's: Expected PaCO₂ = 1.5×HCO₃⁻ + 8 ± 2
ΔΔ = ΔAG/ΔHCO₃⁻ [<1 mixed; 1-2 pure HAGMA; >2 HAGMA+met alk]
A-a gradient = PAO₂ - PaO₂ | Normal <10 mm Hg
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine | Barash, Cullen & Stoelting's Clinical Anesthesia (9e) | Tintinalli's Emergency Medicine | National Kidney Foundation Primer on Kidney Diseases (8e) | Ganong's Review of Medical Physiology (26e) | Miller's Anesthesia (10e) | Harrison's Principles of Internal Medicine (22e, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.