Perioperative pulmonary embolism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"perioperative pulmonary embolism" AND management
Reading File
Reading File
Searching PubMed
"pulmonary embolism" AND "perioperative" AND prevention
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content to write a thorough, well-organized answer on perioperative pulmonary embolism. Let me compile the full response.
Perioperative Pulmonary Embolism
Perioperative PE is one of the leading preventable causes of in-hospital death. In the Confidential Enquiry into Perioperative Deaths, PE accounted for 7.8% of causes of perioperative mortality - Miller's Anesthesia, 10e. It results from thrombotic occlusion of the pulmonary vasculature, almost always from a deep vein thrombosis (DVT) originating in the lower extremity or pelvic veins.
1. Pathophysiology and Virchow's Triad in Surgery
Surgery activates all three components of Virchow's triad:
- Venous stasis - immobility, positioning on the operating table, general anaesthesia reducing venous tone
- Hypercoagulability - the systemic inflammatory and prothrombotic response to surgical trauma, increases in coagulation factors (V, VIII, X, von Willebrand factor)
- Endothelial injury - direct vessel trauma, especially in pelvic, orthopaedic, and vascular surgery
The thrombus typically forms in the deep veins of the calf, propagates proximally, and embolizes to the pulmonary arteries. The resulting obstruction causes:
- Increased right ventricular afterload → RV dilation and dysfunction
- Ventilation-perfusion mismatch → hypoxaemia
- Release of vasoactive mediators (serotonin, thromboxane A2) causing bronchoconstriction
- Reduced left ventricular preload → hypotension and shock
2. Risk Factors
Surgical patients carry multiple compounding risk factors - Schwartz's Principles of Surgery, 11e:
Acquired
| Category | Examples |
|---|---|
| Patient-related | Advanced age, obesity, prior VTE, malignancy, pregnancy/puerperium, antiphospholipid syndrome, polycythemia, myeloproliferative disease |
| Surgical | Major surgery (general, vascular, orthopaedic), prolonged procedure time, pelvic surgery, lower limb surgery |
| Situational | Immobility/hospitalization, trauma, spinal cord injury, hormone use (OCP/HRT), nephrotic syndrome |
Inherited thrombophilias
- Factor V Leiden, Prothrombin G20210A, antithrombin deficiency, protein C and S deficiency, factor XI elevation
High-risk surgical procedures:
- Hip and knee arthroplasty (disproportionately elevated risk)
- Major abdominal and pelvic surgery (colorectal, gynaecological, urological)
- Neurosurgery and spinal surgery
- Operations involving renal cell carcinoma with IVC extension
3. Preoperative Risk Stratification
Validated scoring systems guide prophylaxis decisions - Schwartz's, 11e:
- Caprini Score and Rogers Score - these take into account the number of VTE risk factors and recommend prophylactic anticoagulation for moderate-to-high risk patients. Orthopaedic patients are excluded from general risk scores due to their disproportionately elevated VTE risk and are managed separately.
- The 9th edition ACCP Guidelines for Prevention of VTE in Non-Orthopaedic Surgical Patients recognise both scores and provide risk-stratified prophylaxis recommendations.
4. Prophylaxis
Mechanical methods (preferred in high bleeding risk):
- Graduated compression stockings
- Pneumatic sequential compression devices (applied to the lower limbs intraoperatively and postoperatively)
Pharmacological methods:
- Low-molecular-weight heparin (LMWH) - e.g., enoxaparin
- Unfractionated heparin (UFH) - low dose subcutaneous
- Direct oral anticoagulants (DOACs) - particularly for orthopaedic surgery (rivaroxaban, apixaban, dabigatran)
- Low-dose aspirin - the Pulmonary Embolism Prevention (PEP) trial showed benefit in orthopaedic surgery
Combination of mechanical + pharmacological prophylaxis is preferable in high-VTE-risk patients - Current Surgical Therapy, 14e.
Duration:
- Standard: duration of hospital stay
- Extended prophylaxis (>3 weeks post-surgery) is necessary for major procedures such as hip/knee arthroplasty, major abdominal/pelvic surgery for cancer, and surgery for IBD (LMWH for up to 28 days after any abdominal procedure for IBD - Bailey & Love, 28e)
Early mobilisation is one of the most important non-pharmacological measures, as it reduces venous stasis and lowers VTE risk - Current Surgical Therapy, 14e.
Patients with prior PE presenting for elective surgery:
- If the acute PE occurred >1 year earlier, the risk from temporarily stopping anticoagulation is probably small - Morgan & Mikhail's Clinical Anaesthesiology, 7e
- Emphasis is on preventing new embolic events with adequate perioperative prophylaxis
5. Intraoperative PE
Significant PE during anaesthesia is rare but life-threatening. It requires a high index of suspicion - Morgan & Mikhail, 7e.
Types of intraoperative embolism:
| Type | Setting |
|---|---|
| Thromboembolism | Prolonged procedures; pre-existing thrombus dislodged by surgical manipulation or position change |
| Air embolism | Common but often overlooked; large amounts can be fatal |
| Fat embolism | Orthopaedic procedures (intramedullary reaming, joint replacement) |
| Bone marrow / microthrombi | During cemented arthroplasty |
| Tumour embolism | Renal cell carcinoma with IVC extension |
| Amniotic fluid embolism | Late pregnancy and obstetric delivery; rare, unpredictable, often fatal |
Intraoperative presentation:
- Sudden cardiovascular collapse, severe hypotension
- Hypoxaemia (unexplained fall in SpO₂)
- Bronchospasm
- Sudden decrease in end-tidal CO₂ (increased dead space - not specific but suggestive)
- Elevated central venous pressure (on invasive monitoring)
- TEE: right heart dilatation and dysfunction (may not directly visualise the clot)
Intraoperative management:
- Intravenous fluids and vasopressors/inotropes (supportive care)
- Aspiration of air via central venous catheter if air embolism is suspected
- Cardiopulmonary bypass for emergency pulmonary embolectomy in extreme cases
- Postoperative consideration of IVC filter placement
6. Postoperative PE: Clinical Presentation
Postoperative PE most commonly occurs in the first 2 weeks after surgery. The presentation can range from asymptomatic to sudden cardiovascular collapse - Rosen's Emergency Medicine, 10e.
Symptoms:
- Dyspnoea - most common (75-80% of cases); may be absent in ~25%
- Chest pain - second most common; may be pleuritic (worsened by inspiration) - only present in 20%; suggests peripheral infarction
- Haemoptysis - with pulmonary infarction
- Unilateral leg swelling (DVT symptoms) - <30% of PE patients
- Palpitations, syncope, severe anxiety
- Low-grade fever (<38.6°C; higher temperature suggests infection rather than infarction)
- Shock index >1 (HR > systolic BP) with impending arrest
Massive PE: can occlude the entire right ventricular outflow system (see autopsy image below), causing sudden cardiac arrest. Approximately 25% of sudden cardiac deaths are thought to be due to PE - Rosen's.
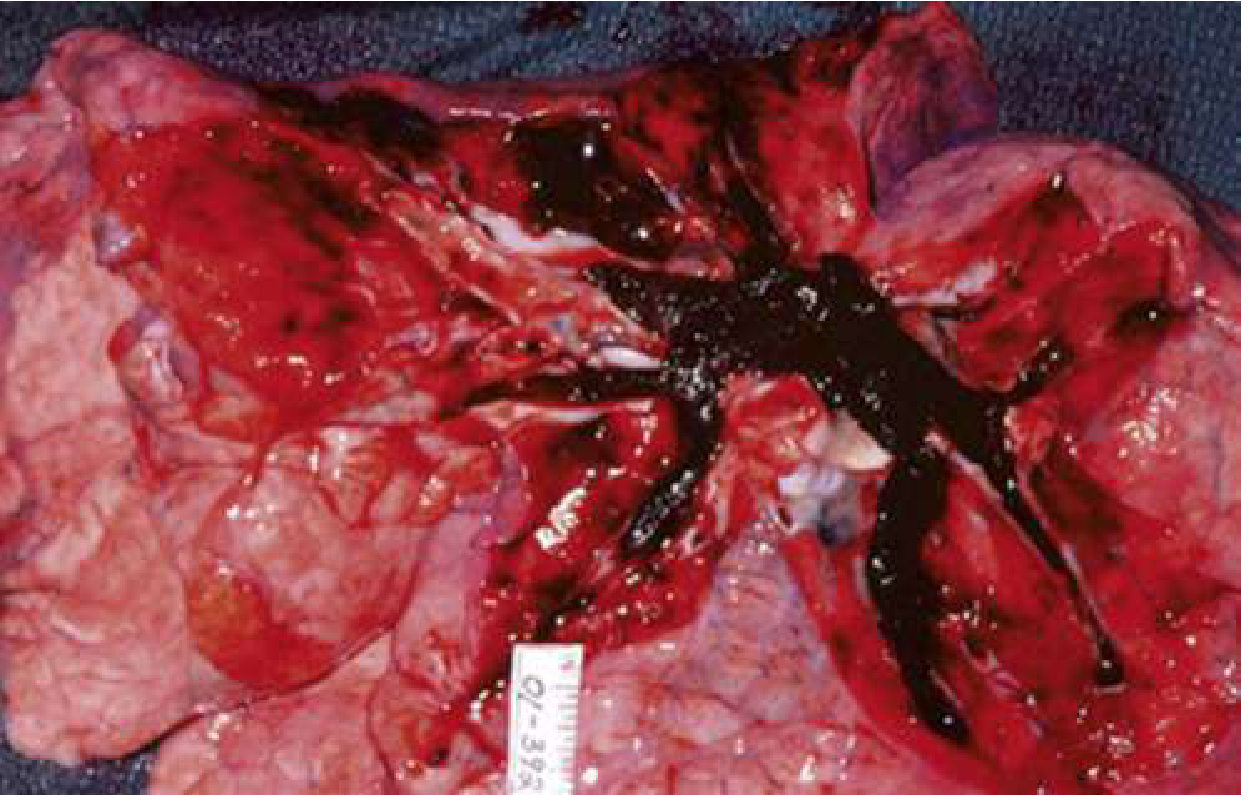
Autopsy photograph: massive PE with complete occlusion of the right ventricular outflow system - Rosen's Emergency Medicine, 10e
7. Diagnosis
Clinical Probability Assessment
- Wells Score (PE version) and Revised Geneva Score - stratify patients into low, intermediate, and high pre-test probability (PTP)
- PERC Rule (Pulmonary Embolism Rule-Out Criteria) - if ALL 8 criteria met in a low-PTP patient, PE can be excluded without further testing - Rosen's:
| PERC Criteria |
|---|
| Age < 50 |
| Pulse < 100 bpm |
| SaO₂ > 94% |
| No unilateral leg swelling |
| No haemoptysis |
| No recent trauma or surgery |
| No prior PE/DVT |
| No hormone use |
D-Dimer
- 95-98% sensitive, 40-55% specific - Rosen's
- Useful to exclude PE in non-high PTP patients (NPV 99-100% with normal result)
- Age-adjusted threshold: Age × 10 ng/mL (when standard threshold is 500 ng/mL) - increases the number who can avoid CT by 5-6% overall and 10-20% in patients >70 years old
- False negatives: subacute/chronic PE, severe lipaemia, ongoing warfarin therapy
- Important caveat in postoperative patients: D-dimer is almost universally elevated after surgery due to wound healing - it has essentially no diagnostic utility in the early postoperative period and imaging is required when suspicion exists
Imaging
- CT Pulmonary Angiography (CTPA) - first-line recommended imaging when PE is suspected - Miller's Anesthesia, 10e
- V/Q scan - used when CTPA is contraindicated (contrast allergy, renal insufficiency, pregnancy - halving the perfusion dose is standard in pregnancy)
- Echocardiography - NOT recommended in initial diagnostic evaluation, but has utility in risk stratification, prognostication, and monitoring response to therapy once diagnosis is established - Miller's Anesthesia, 10e
Biomarkers
- Troponin - elevation indicates myocardial injury from RV strain; associated with high short-term mortality - Murray & Nadel, 2e
- BNP/NT-proBNP - marker of RV pressure overload
- ABG - hypoxaemia, hypocapnia (hyperventilation), respiratory alkalosis; increased alveolar-arterial oxygen gradient
8. Risk Stratification and Treatment
Classification - Miller's Anesthesia, 10e:
| Category | Definition | Mortality |
|---|---|---|
| High-risk (Massive) | Sustained hypotension or shock not explained by other causes | 15-50% |
| Intermediate-risk (Submassive) | Normotensive + RV dysfunction and/or troponin elevation | 3-15% |
| Low-risk | Normotensive, no RV dysfunction | <1% to 3% |
Treatment Table - Rosen's Emergency Medicine, 10e:
| Category | Criteria | Management |
|---|---|---|
| Low-risk PE | Haemodynamically stable; no RV dysfunction | DOAC (preferred); may discharge home if Hestia criteria negative |
| Intermediate-risk PE | Stable + RV dysfunction on echo/CTPA, troponin positive, or elevated BNP | Anticoagulation (DOAC or heparin); activate PERT; monitored bed; thrombolysis in minority |
| High-risk PE | Haemodynamically unstable | UFH + thrombolysis (if no contraindication) or thromboembolectomy; PERT activation; ICU |
Anticoagulation
- Unfractionated heparin (IV infusion) - preferred when thrombolysis or surgical embolectomy is planned (short half-life, reversible)
- LMWH (e.g., enoxaparin) - for stable patients; predictable pharmacokinetics; avoid or dose-adjust in renal failure
- DOACs (rivaroxaban, apixaban, dabigatran) - preferred for low/intermediate risk if no contraindications; avoid in haemodynamic instability
Respiratory and Haemodynamic Support - Rosen's:
- Supplemental oxygen to target SpO₂ >90% (hypoxaemia worsens pulmonary vasoconstriction)
- Avoid intubation if possible - positive pressure ventilation increases intrathoracic pressure, reduces RV preload, and can precipitate haemodynamic collapse in severe PE
- If intubation is unavoidable: pre-optimise haemodynamics with vasopressors before induction
- Vasopressors (noradrenaline) + inotropes (dobutamine) for RV support
Systemic Thrombolysis
- Alteplase (rtPA) 100 mg IV over 2 hours - indicated for massive PE without contraindications
- Relatively contraindicated in recent surgery - the perioperative period itself is a relative contraindication; the risk of haemorrhage must be weighed against the risk of death from massive PE
- Catheter-directed thrombolysis delivers lower doses locally for intermediate-high risk PE with unacceptable bleeding risk
Surgical / Interventional Options
- Catheter-directed thrombectomy - mechanical clot disruption/aspiration
- Surgical pulmonary embolectomy - reserved for massive PE with contraindications to thrombolysis or failed thrombolysis; patients are critically ill and often haemodynamically unstable; cardiopulmonary bypass is required - Morgan & Mikhail, 7e
- IVC filter - placed percutaneously under local anaesthesia + sedation; indicated when anticoagulation is contraindicated (recent surgery with high bleeding risk) or has failed; protects against further embolization but does NOT treat the existing PE and may increase long-term DVT risk
9. Special Situations
Pregnancy
- Leading cause of maternal mortality (15% of maternal deaths, USA 2003-2011) - Murray & Nadel, 2e
- Risk ~5x higher than non-pregnant women due to raised coagulation factors (V, VIII, X, von Willebrand factor), fall in protein S, and venous stasis from IVC compression
- Peak incidence: postpartum, especially after caesarean section
- D-dimer is not reliable in pregnancy - the pregnancy-adapted YEARS algorithm (clinical signs of DVT + haemoptysis + PE as most likely diagnosis + D-dimer) can assist but has limitations
- Imaging: V/Q scan (halved perfusion dose) or CTPA, both acceptable with radiation modifications
- Treatment: LMWH throughout pregnancy; warfarin teratogenic; DOACs contraindicated
IBD Surgery
- IBD carries 3x increased VTE risk; postoperative VTE rate ~3% - Bailey & Love, 28e
- 74% of VTE events occur during initial hospitalisation, 61% within first 2 weeks
- Extended prophylaxis with LMWH for up to 28 days post-surgery recommended
10. Summary: Key Perioperative Considerations
| Phase | Key Actions |
|---|---|
| Preoperative | Risk stratify (Caprini/Rogers score), plan prophylaxis, review anticoagulants |
| Intraoperative | Maintain high index of suspicion for PE; mechanical prophylaxis; minimise stasis |
| Postoperative | Early mobilisation; pharmacological + mechanical prophylaxis; extended duration in high-risk cases; prompt investigation of unexplained hypoxaemia or haemodynamic instability |
| Diagnosed PE | Classify risk; anticoagulate; supportive care; PERT activation; thrombolysis or embolectomy for massive PE |
Sources:
- Miller's Anesthesia, 2-Volume Set, 10e - Perioperative PE classification, imaging, risk stratification
- Morgan & Mikhail's Clinical Anaesthesiology, 7e - Intraoperative PE, anaesthetic management
- Rosen's Emergency Medicine, 10e - Clinical features, diagnosis (PERC, D-dimer, CTPA), risk stratification and treatment table
- Schwartz's Principles of Surgery, 11e - Risk factors, Caprini/Rogers scoring, prophylaxis guidelines
- Murray & Nadel's Respiratory Medicine, 2e - Troponin prognostication, PE in pregnancy
- Current Surgical Therapy, 14e - VTE prophylaxis within ERAS; mechanical + pharmacological strategies
- Bailey & Love's Short Practice of Surgery, 28e - Extended prophylaxis in IBD surgery
This is a shared conversation. Sign in to Orris to start your own chat.