what is the seizure
Reading File
Finding Sources
Searching the Web
seizure definition types causes treatment 2024
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive information from multiple authoritative medical textbooks. Here is a complete answer:
What is a Seizure?
A seizure (from the Latin sacire, "to take possession of") is a transient occurrence of signs or symptoms due to abnormal, excessive, or synchronous neuronal activity in the brain. Depending on where the discharge occurs, manifestations range from dramatic convulsive activity to subtle experiential phenomena. About 5-10% of the population will have at least one seizure in their lifetime, with the highest incidence in early childhood and late adulthood.
- Harrison's Principles of Internal Medicine 22E, p. 3452
Seizure vs. Epilepsy - Key Distinction
| Term | Meaning |
|---|---|
| Seizure | A single episode of abnormal brain electrical activity (may be provoked or unprovoked) |
| Epilepsy | A chronic condition - at least 2 unprovoked seizures >24 hours apart, OR 1 unprovoked seizure with ≥60% risk of recurrence over 10 years |
- A provoked seizure occurs in close temporal relationship with an acquired precipitating condition (also called "acute symptomatic seizure")
- An unprovoked seizure occurs without such a temporary or reversible cause
- After a single unprovoked seizure, the risk of a second seizure is approximately 40-50% over the next 2-8 years
- Frameworks for Internal Medicine, p. 559
Classification of Seizures (ILAE 2017)
The International League Against Epilepsy (ILAE) 2017 classification divides seizures into three main categories:
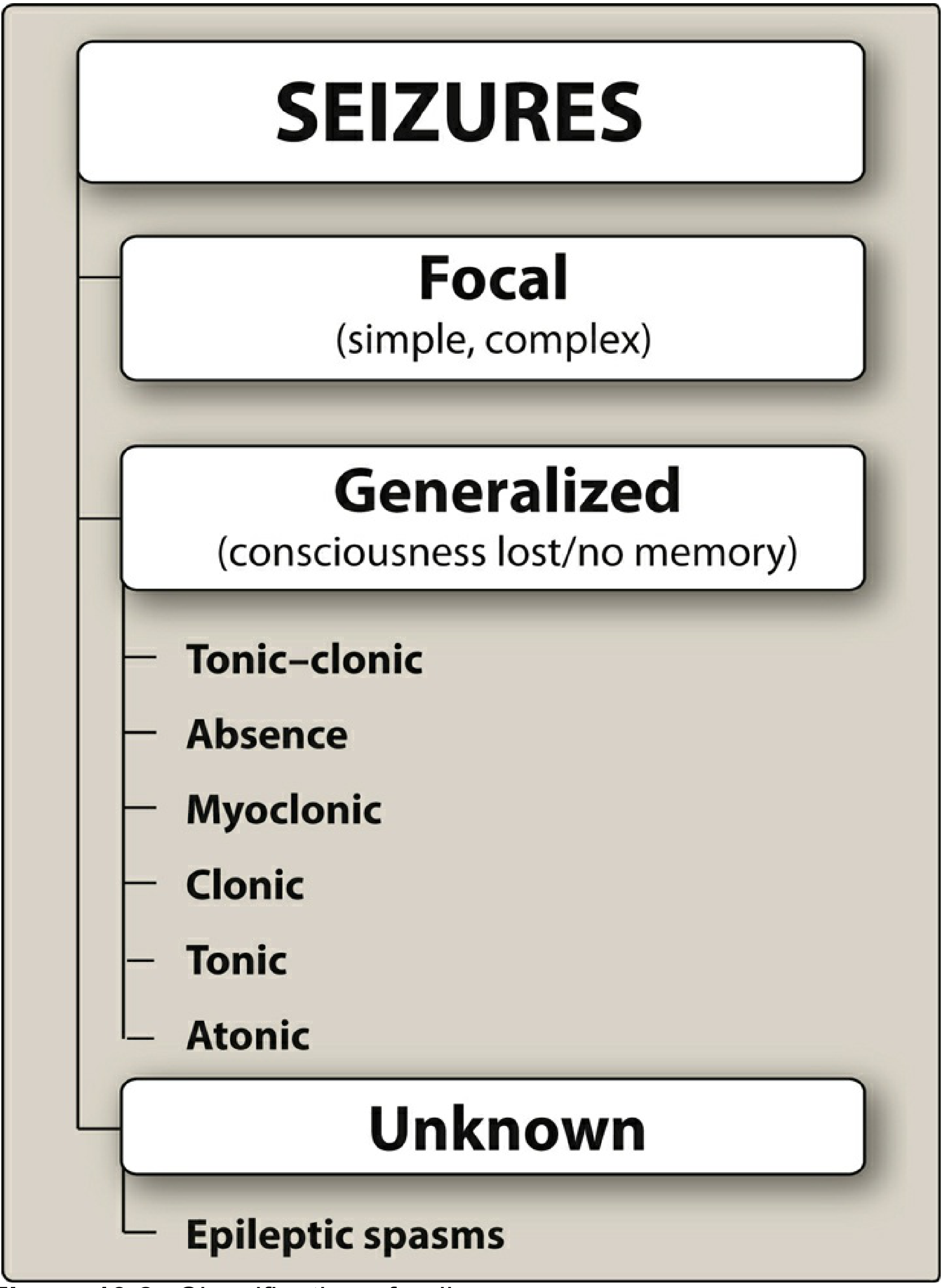
1. Focal Onset Seizures
Originate within a neuronal network limited to one cerebral hemisphere. The older terms "partial," "simple partial," and "complex partial" are no longer used. They are now described by:
- Awareness: intact or impaired
- Onset type: motor or nonmotor
Examples:
- Focal motor seizure: involuntary movements (e.g., hand jerking); can show "Jacksonian march" (spreading from fingers up the arm as seizure spreads across motor cortex)
- Todd's paralysis: localized weakness for minutes to hours after a focal motor seizure
- Focal seizures can secondarily evolve into bilateral tonic-clonic seizures
2. Generalized Onset Seizures
Arise within and rapidly engage both cerebral hemispheres simultaneously, with resultant loss of consciousness. Types include:
| Type | Description |
|---|---|
| Tonic-clonic ("grand mal") | Loss of consciousness, then tonic (rigid) phase followed by clonic (rhythmic jerking) phase; post-ictal confusion and exhaustion |
| Absence ("petit mal") | Brief (3-5 sec), abrupt loss of consciousness with staring and rapid eye blinking; classic 3/sec spike-wave on EEG; onset ages 3-5 |
| Myoclonic | Brief, sudden muscle jerks; often occur after waking; typically begin around puberty |
| Clonic | Rhythmic muscle contractions; more impaired consciousness than myoclonic |
| Tonic | Sustained muscle rigidity/extension; usually <60 seconds |
| Atonic ("drop attacks") | Sudden loss of muscle tone, patient collapses |
3. Unknown Onset
Used when onset cannot be determined; includes epileptic spasms.
Common Causes
Provoked (acute symptomatic) causes:
- Metabolic disturbances (low blood sugar, electrolyte abnormalities)
- CNS infection (meningitis, encephalitis)
- Drug or alcohol toxicity/withdrawal
- Head trauma
- Stroke
- Fever (especially in children - febrile seizures)
Epilepsy (unprovoked) causes:
- Genetic/idiopathic - most common overall (likely undiscovered genetic mutations)
- Structural: prior head trauma, stroke, brain tumor, intracranial infection
- Neurocutaneous disorders (tuberous sclerosis, neurofibromatosis)
Common Triggers (in Epileptic Patients)
Flashing lights, intense exercise, loud music, strong emotions, sleep deprivation, fever, hormonal changes, hyperventilation, stress, and certain medications (e.g., bupropion) can lower the seizure threshold.
How Anti-Seizure Drugs Work
Antiseizure medications suppress (but do not cure) seizures through:
- Blocking voltage-gated Na+ or Ca2+ channels
- Enhancing GABAergic (inhibitory) transmission
- Interfering with glutamate (excitatory) transmission
Long-term remission is achieved in most patients, though monotherapy is effective in less than half - many need combination therapy.
- Lippincott Illustrated Reviews: Pharmacology, p. 635-636
Key Investigations
- EEG (electroencephalogram): shows epileptiform spikes/waves; absence seizures have a classic 3/sec spike-and-wave pattern
- MRI/CT brain: to identify structural causes
- Blood tests: glucose, electrolytes, CBC, metabolic panel
- Detailed history from witnesses is essential since patients are often unaware of ictal events
In summary: A seizure is a sudden, abnormal electrical discharge in the brain producing transient symptoms. It is classified as focal (one hemisphere) or generalized (both hemispheres), with dozens of subtypes. Epilepsy is the chronic condition of recurrent unprovoked seizures. Management targets the underlying cause, avoidance of triggers, and antiseizure medications when indicated.
This is a shared conversation. Sign in to Orris to start your own chat.