Primitive stresk
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of the primitive streak drawn from authoritative embryology textbooks.
Primitive Streak
What It Is
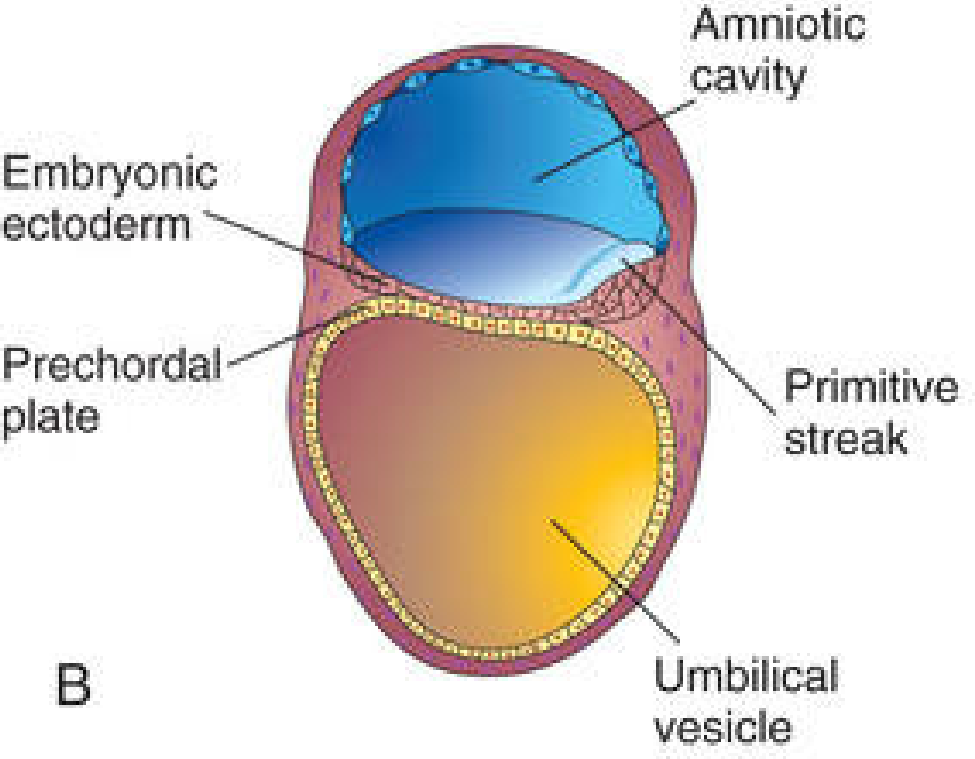
The primitive streak is the first morphological sign of gastrulation. It appears at the beginning of the third week (~day 15) as a thickened, linear band of epiblastic cells at the caudal end of the dorsal surface of the bilaminar embryonic disc. It forms by proliferation and movement of epiblast cells toward the median plane.
Structure
| Part | Description |
|---|---|
| Primitive streak | Caudal thickening of epiblast in the midline |
| Primitive groove | Central depression running along the streak |
| Primitive node (Hensen's node) | Cranial end of the streak; slightly elevated knot of cells |
| Primitive pit | Depression in the center of the primitive node |
As soon as the streak appears, the embryo's craniocaudal axis, dorsal/ventral surfaces, and right/left sides can be identified.
Function: Gastrulation
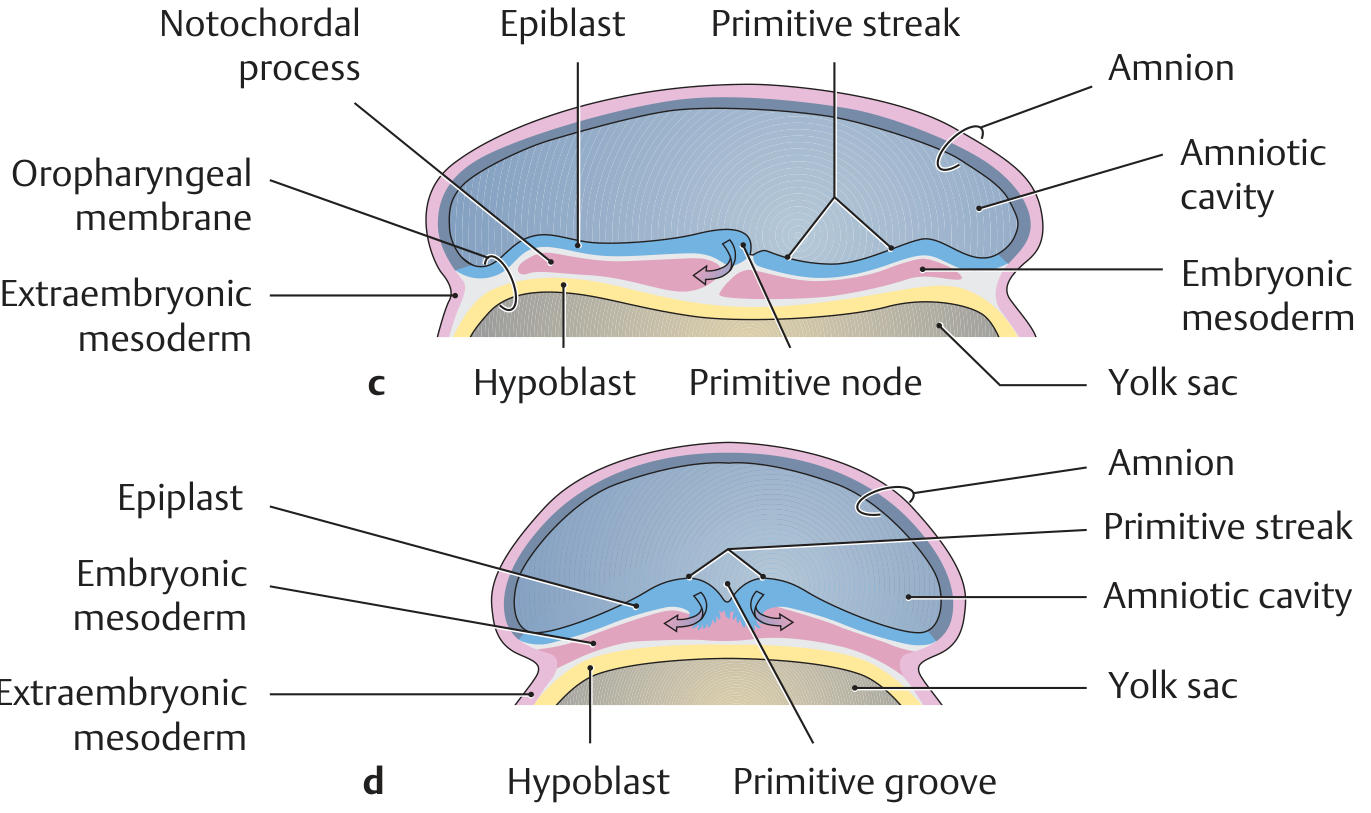
Epiblast cells migrate toward the streak, invaginate through the primitive groove, and spread out laterally and cranially between the epiblast and hypoblast. This process - gastrulation - converts the bilaminar disc into a trilaminar disc with 3 germ layers:
- Ectoderm - cells that remain in the epiblast layer
- Mesoderm (intraembryonic) - cells that migrate through the streak and spread between ectoderm and endoderm; first form mesenchyme (mesoblast)
- Endoderm - cells that migrate through the streak and displace the hypoblast
Cells from the primitive node specifically migrate cranially to form the notochordal process, which eventually becomes the notochord.
Molecular Signals
- Nodal (TGF-β superfamily) - induces mesoderm formation
- Wnt3a, Wnt5a, FGFs - specify germ layer fates
- Nodal + veg T + Wnt signaling - involved in endoderm specification
Fate of the Primitive Streak
The streak actively produces mesoderm until early week 4, then slows. It regresses caudally into the sacrococcygeal region and normally disappears by the end of week 4.
Clinical relevance - Sacrococcygeal teratoma: If remnants of the primitive streak persist, they can give rise to a sacrococcygeal teratoma - a tumor containing tissues from all three germ layers (hair, teeth, nervous tissue, etc.). This is the most common tumor of the newborn, occurring predominantly in females (~4:1 ratio). Because of the pluripotent nature of these cells, the tumors can be benign or malignant.
Summary Table
| Feature | Detail |
|---|---|
| Appears | Day 15 (start of week 3) |
| Location | Caudal midline of embryonic disc epiblast |
| Establishes | Craniocaudal axis, left-right axis, dorsoventral axis |
| Products | Mesoderm, endoderm (ectoderm = remaining epiblast) |
| Disappears | End of week 4 |
| Remnant tumor | Sacrococcygeal teratoma |
- The Developing Human: Clinically Oriented Embryology; General Anatomy and Musculoskeletal System (THIEME Atlas)
Give me a 5 marks ready ram short note
Short Note: Primitive Streak (5 Marks)
Definition & Appearance
The primitive streak is the first morphological sign of gastrulation. It appears at the beginning of the 3rd week (day 15) as a thickened linear band of epiblast cells at the caudal end of the dorsal surface of the bilaminar embryonic disc.
Structure
- Primitive groove - central depression along the streak
- Primitive node (Hensen's node) - cranial bulge/knot at the head end
- Primitive pit - depression within the node
Once formed, it establishes the embryo's craniocaudal axis, dorsoventral surfaces, and left-right sides.
Function (Gastrulation)
Epiblast cells migrate toward the streak, invaginate through the primitive groove, and spread laterally to form 3 germ layers:
- Ectoderm - epiblast cells that remain
- Mesoderm - cells migrating through the streak laterally
- Endoderm - cells that displace the hypoblast
Cells from the primitive node migrate cranially to form the notochord.
Fate
- Actively forms mesoderm until early 4th week
- Regresses to the sacrococcygeal region
- Normally disappears by end of week 4
Clinical Significance
Persistence of primitive streak remnants leads to sacrococcygeal teratoma - a tumor containing tissues of all 3 germ layers, most common tumor of the newborn, more common in females (4:1).
Sn on branchopulmonary segments
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Short Note: Bronchopulmonary Segments (5 Marks)
Definition
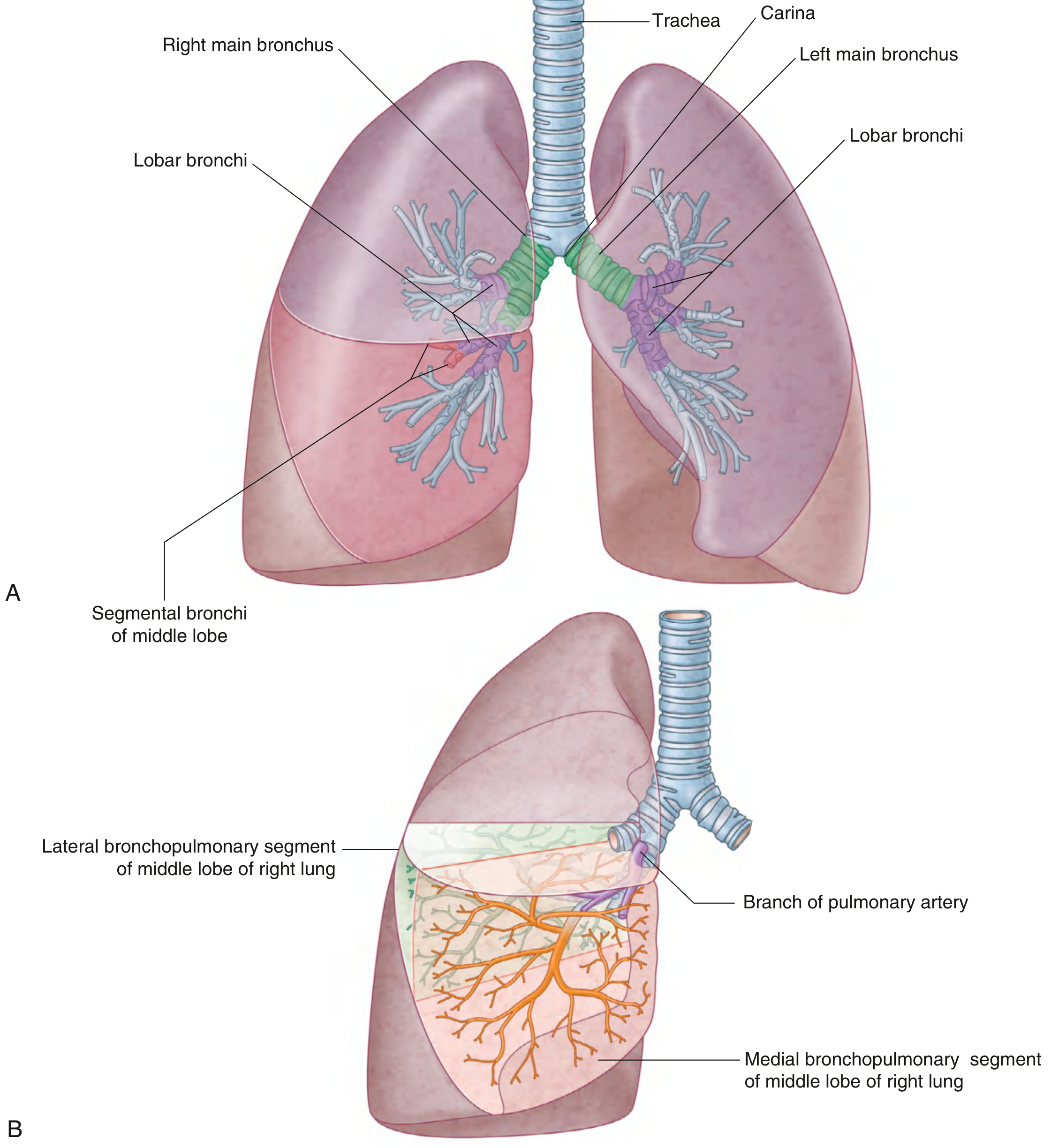
A bronchopulmonary segment is the smallest functionally independent unit of the lung, supplied by a segmental (tertiary) bronchus and an accompanying branch of the pulmonary artery. It is the smallest area of lung that can be surgically resected without affecting adjacent regions.
Structure
- Shape: Irregular cone/pyramid - apex directed toward the hilum, base projecting onto the lung surface
- Each segment is surrounded by connective tissue septa (subpleural connective tissue)
- Segmental bronchus + pulmonary artery branch run together centrally (intrasegmental)
- Pulmonary vein tributaries run in the connective tissue between segments (intersegmental) - they demarcate segment boundaries
Number of Segments
| Lung | Lobes | No. of Segments |
|---|---|---|
| Right lung | 3 (upper, middle, lower) | 10 |
| Left lung | 2 (upper, lower) | 8-9 (some fuse) |
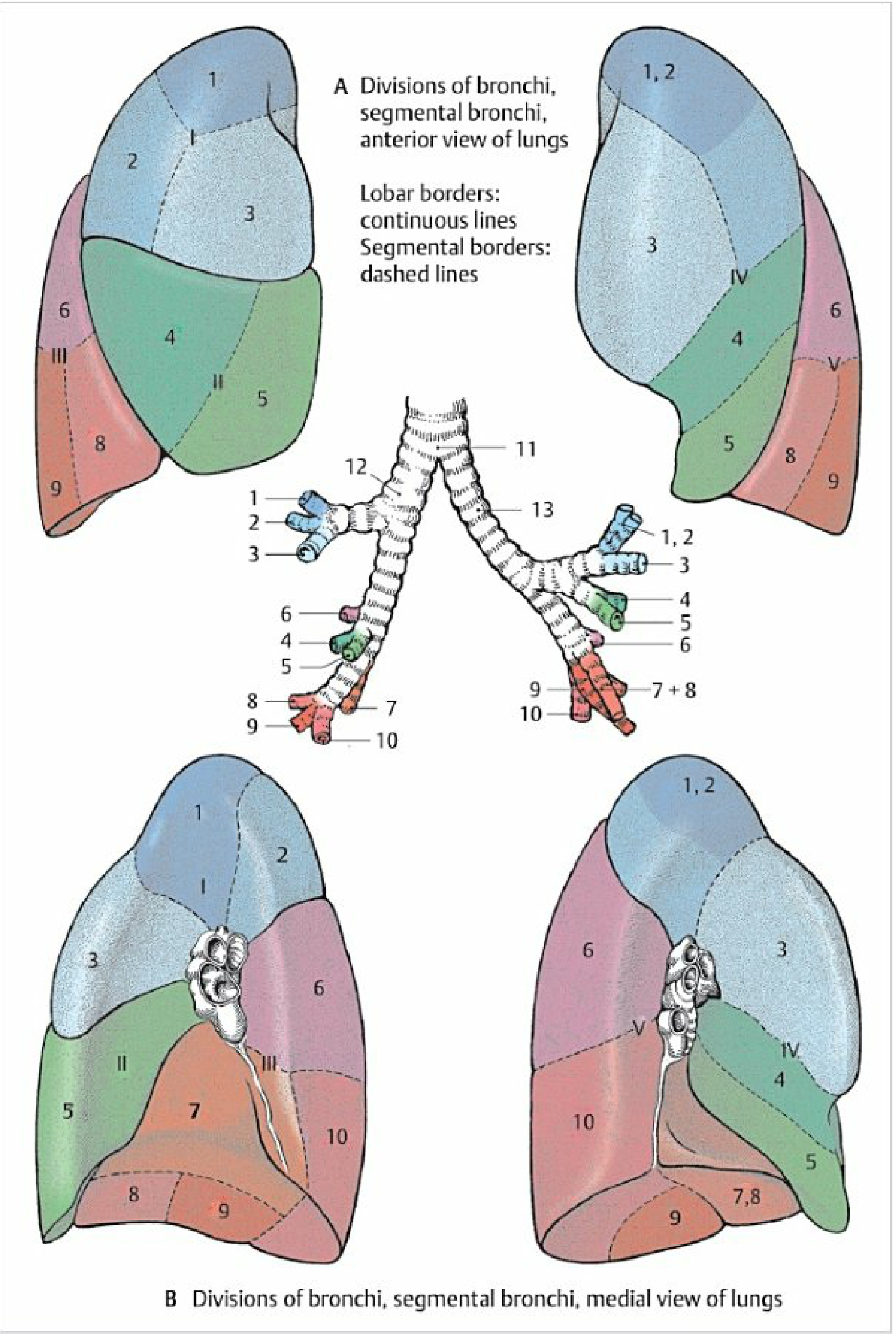
Segments - Right Lung (10)
| Lobe | Segments |
|---|---|
| Upper lobe | 1. Apical, 2. Posterior, 3. Anterior |
| Middle lobe | 4. Lateral, 5. Medial |
| Lower lobe | 6. Superior, 7. Medial basal, 8. Anterior basal, 9. Lateral basal, 10. Posterior basal |
Segments - Left Lung (8-9)
| Lobe | Segments |
|---|---|
| Upper lobe | 1+2. Apicoposterior (fused), 3. Anterior, 4. Superior lingular, 5. Inferior lingular |
| Lower lobe | 6. Superior, 7+8. Anteromedial basal (fused), 9. Lateral basal, 10. Posterior basal |
Blood Supply Summary
| Structure | Course |
|---|---|
| Segmental bronchus | Central, intrasegmental |
| Pulmonary artery branch | Central, intrasegmental (alongside bronchus) |
| Pulmonary vein tributaries | Peripheral, intersegmental (between segments) |
Clinical Significance
- Surgical resection (segmentectomy) - because each segment has its own independent vascular and bronchial supply, it can be removed individually (e.g., in localized bronchiectasis, tuberculosis, or small lung tumors)
- Postural drainage - knowledge of segment positions allows targeted positioning to drain infected/secretion-filled segments
- Aspiration pneumonia - most commonly affects dependent segments: posterior basal (right > left) in supine patients, superior segment of lower lobe in semi-recumbent patients
- Bronchoscopy - segmental anatomy guides bronchoscope navigation to lesions
- Gray's Anatomy for Students; Color Atlas of Human Anatomy Vol. 2 (THIEME)
This is a shared conversation. Sign in to Orris to start your own chat.