1,2,3 trimester abdominal examination in pregnant women with visual,and images form and easy to understand and give all essential data
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
abdominal examination pregnant women 1st 2nd 3rd trimester Leopold maneuvers fundal height clinical guide
Finding Sources
Finding Sources
Reading Web Page
abdominal examination pregnancy trimester Leopold maneuvers fundal height
Loading Image
Searching the Web
Leopold maneuvers 4 steps diagram clinical image pregnancy abdominal palpation
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Searching the Web
fundal height landmarks weeks gestation diagram pubic symphysis umbilicus xiphoid
Loading Image
Loading Image
Excellent! I now have all the key images and clinical content. Let me compile the comprehensive, visually rich guide.
Abdominal Examination in Pregnancy: All Three Trimesters
A complete, trimester-by-trimester guide to obstetric abdominal examination with clinical landmarks, techniques, and images.
🔷 Before You Begin: General Setup
Patient Positioning
| Gestational Age | Position | Reason |
|---|---|---|
| < 28 weeks (1st & 2nd trimester) | Supine, head raised 15-30° | Uterus small enough - no vascular compression |
| > 28 weeks (3rd trimester) | Left lateral tilt (small pillow under right hip) | Prevents aortocaval (IVC) compression causing supine hypotensive syndrome |
Always ask the patient to void before examination - a full bladder obscures fetal contour and causes discomfort.
Systematic Order of Examination
- Inspection - skin changes, shape, size
- Palpation - uterine size, fundal height, fetal parts
- Auscultation - fetal heart rate
📍 Fundal Height: The Most Important Landmark
Textbook Diagram - Fundal Growth at Various Weeks
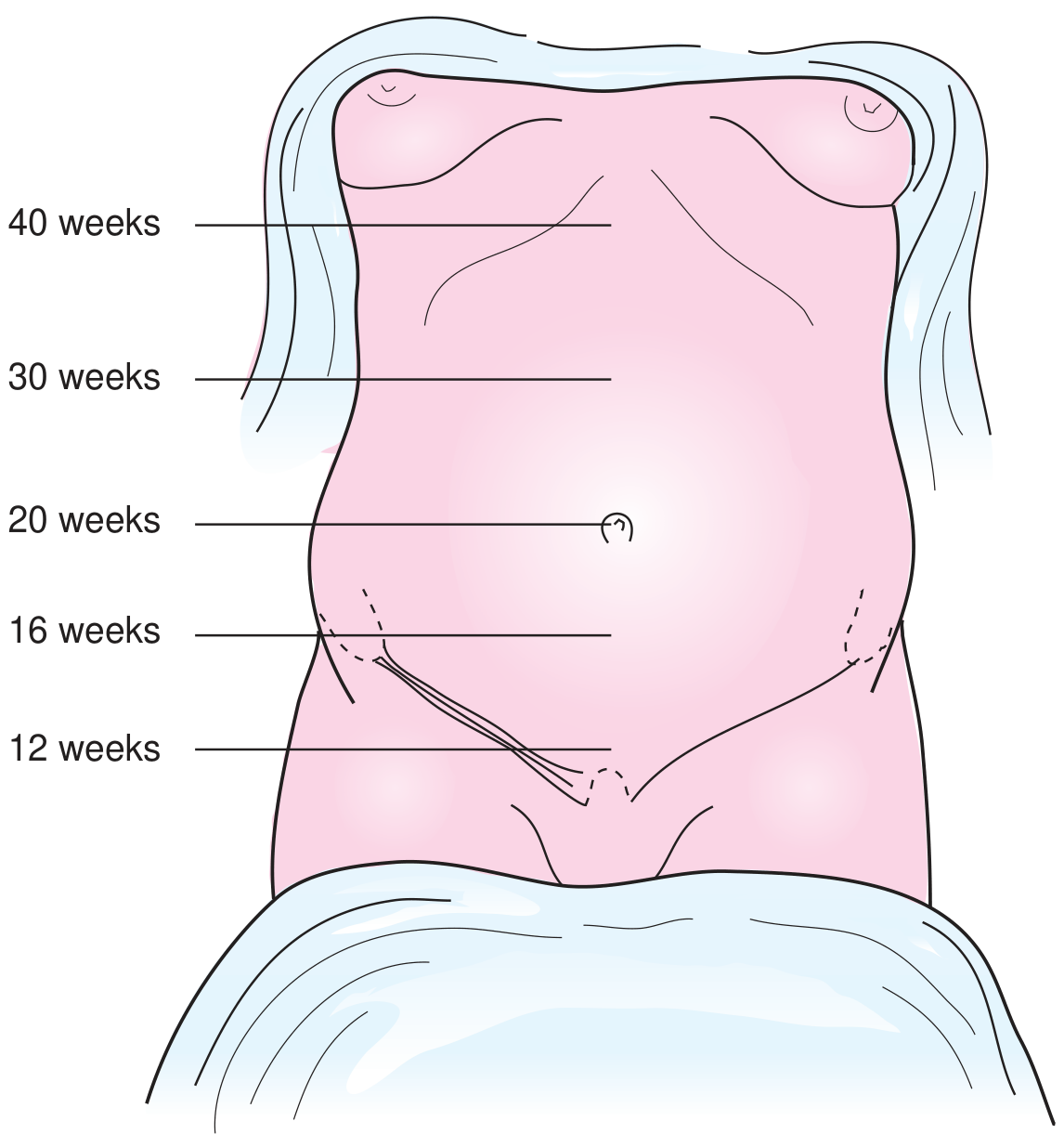
Fig. A - Fundal growth landmarks at 12, 16, 20, 30, and 40 weeks (Textbook of Family Medicine, 9e)
Detailed Fundal Height Reference Diagram
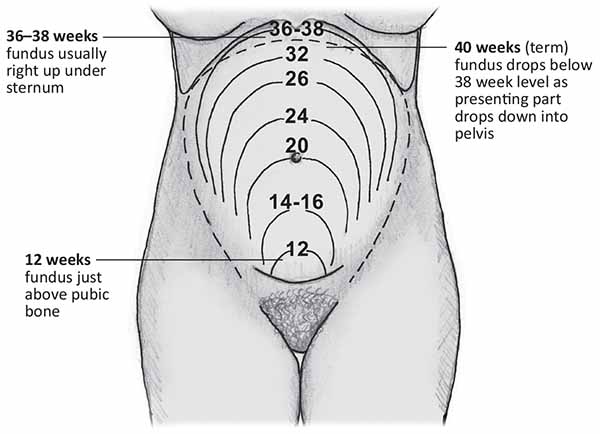
Fig. B - Fundal height contours from 12 weeks to term, with regression at 40 weeks as the presenting part descends
Fundal Height Landmarks at a Glance
| Weeks | Fundal Position | Key Landmark |
|---|---|---|
| 8-10 weeks | Not yet palpable abdominally | Still in pelvis |
| 12 weeks | Just above pubic symphysis | Pubic bone edge |
| 14-16 weeks | Midway between pubis and umbilicus | Between landmarks |
| 20-22 weeks | At the level of the umbilicus | Umbilicus (belly button) |
| 24 weeks | ~4 cm above umbilicus | — |
| 28 weeks | ~8 cm above umbilicus | — |
| 32 weeks | Midway between umbilicus and xiphoid | — |
| 36-38 weeks | At or near xiphoid/sternum | Xiphoid process |
| 40 weeks (term) | Drops slightly below 36-38 wk level | Lightening - head engages |
McDonald's Rule: From 20-32 weeks, fundal height in cm ≈ gestational age in weeks (±2 cm). E.g., at 26 weeks → expect ~24-28 cm.
🟢 FIRST TRIMESTER (Weeks 1-13)
What to Expect
The uterus is a pelvic organ - it cannot be palpated abdominally before 12 weeks.
Inspection
| Feature | What You See | Significance |
|---|---|---|
| Abdominal shape | Flat or minimally distended | Normal - uterus still pelvic |
| Linea nigra | May begin to appear (dark midline line from pubis to umbilicus) | Caused by placental melanocyte-stimulating hormones - normal |
| Striae gravidarum | May begin to form | Stretch marks from dermal tearing - striae rubra (red/pink) appear first |
Palpation
- Uterus: Not palpable abdominally until ~12 weeks
- At 12 weeks: fundus is palpable just at the superior edge of the pubic symphysis
- Gently palpate the lower abdomen just above the pubic bone to feel the uterine dome
- Assess for tenderness (ectopic, miscarriage, fibroid degeneration)
Auscultation
- Fetal heart tones detectable by Doppler from ~10-12 weeks (not by Pinard stethoscope yet)
- Normal FHR: 110-160 bpm
Key Clinical Points - 1st Trimester
- Bimanual pelvic examination is more informative than abdominal exam at this stage
- Hegar's sign: softening of uterine isthmus on bimanual (8-10 wks)
- Goodell's sign: softening of cervix
- Any abdominal pain + positive pregnancy test → rule out ectopic pregnancy
🟡 SECOND TRIMESTER (Weeks 14-27)
What to Expect
The uterus rises out of the pelvis, becoming an abdominal organ. Fundal height measurement becomes clinically useful from 20 weeks onward.
Inspection
| Feature | What You See | Notes |
|---|---|---|
| Abdominal distension | Visible uterine swelling, rounded | Progressive, symmetric |
| Linea nigra | Prominent dark line, pubis to umbilicus (sometimes to xiphoid) | Normal - fades postpartum |
| Striae gravidarum | Pink/red stretch marks (striae rubra) on flanks, lower abdomen | Normal |
| Umbilicus | May flatten or begin to protrude | As uterus expands |
| Fetal movements | Visible skin movement ("quickening") from ~20 weeks | Seen in thin patients |
Palpation - Fundal Height
- From 20 weeks: measure with a tape measure from the superior border of the pubic symphysis to the top of the uterine fundus
- The distance in cm should equal the gestational age in weeks (±2 cm)
- Feel for uterine contour: smooth, firm, non-tender
Organ displacement to be aware of:
- The appendix is pushed superiorly toward the RUQ as the uterus grows - so appendicitis pain may NOT be in the typical right lower quadrant
Palpation - Fetal Parts
- Fetal parts can be felt from ~24-26 weeks
- The fetus is still very mobile - position changes frequently
- The fundal grip identifies which pole is in the fundus
Auscultation
- Pinard stethoscope (fetal stethoscope): audible from ~20-24 weeks
- Doppler: audible from 12 weeks
- Location of heart tones: varies with position - best heard through the fetal back
Key Clinical Points - 2nd Trimester
- Fundal height larger than expected: multiple gestation, polyhydramnios, LGA fetus, uterine fibroids
- Fundal height smaller than expected: oligohydramnios, fetal growth restriction (FGR), inaccurate dates, fetal demise
- Braxton Hicks contractions may be felt - painless, irregular
- Organise referral if fundal height deviates >2 cm from expected
🔴 THIRD TRIMESTER (Weeks 28-40)
What to Expect
This is the most detailed phase of abdominal examination. Leopold's Maneuvers are performed from 30 weeks to determine fetal position and presentation.
Inspection
- Large, globular abdomen
- Fetal movements (kicks, rolls) visible through the abdominal wall
- Linea nigra prominent
- Umbilicus may be everted
- Lightening/engagement: at ~36-38 weeks in nulliparas, the fundus drops and the lower abdomen appears more prominent as the fetal head descends into the pelvis
🔬 LEOPOLD'S MANEUVERS (3rd Trimester - from 30 weeks)
Textbook Diagram - All 4 Maneuvers
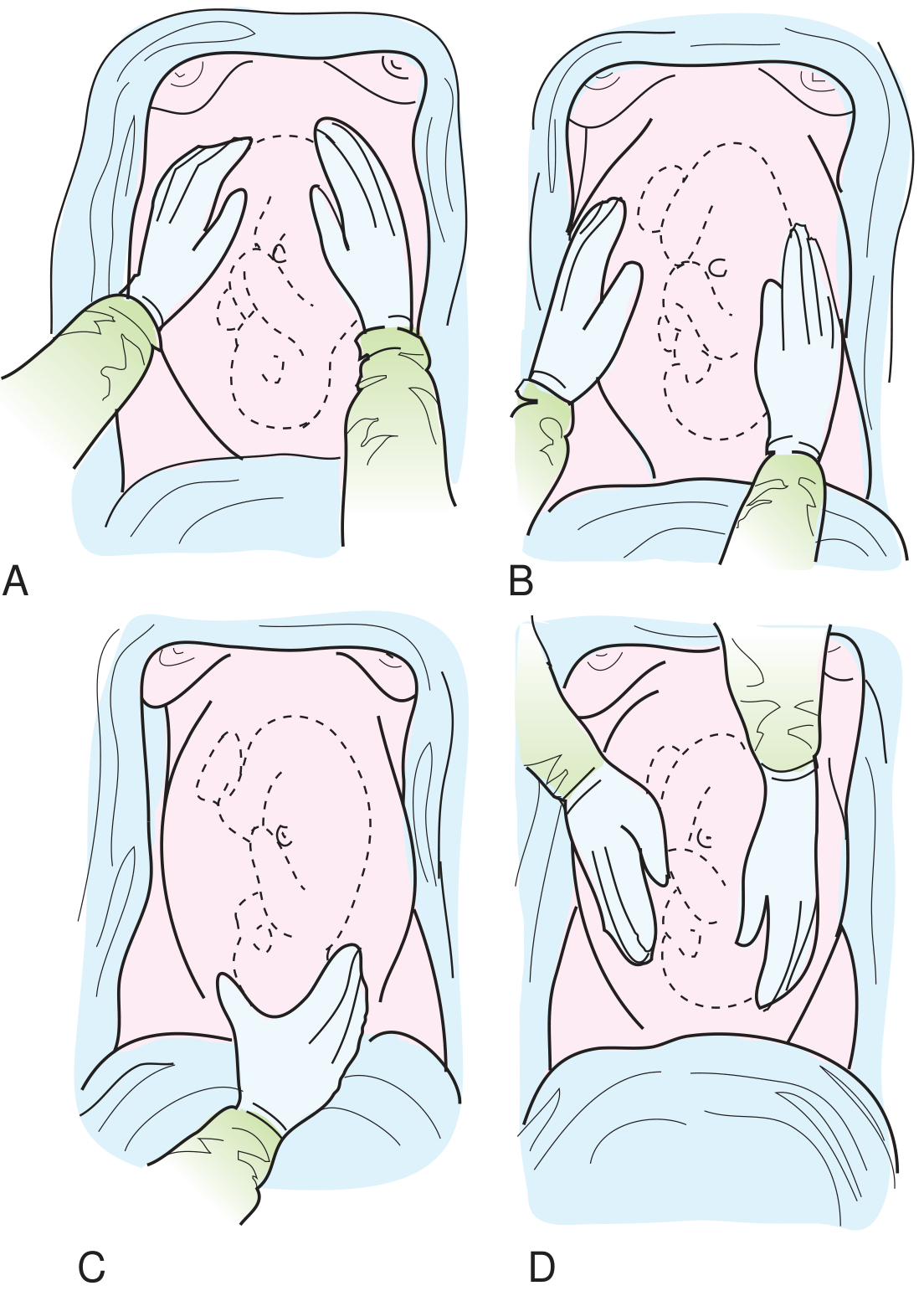
Fig. C - A: 1st maneuver (fundal grip), B: 2nd maneuver (lateral/back location), C: 3rd maneuver (presenting part), D: 4th maneuver (cephalic prominence) - Textbook of Family Medicine 9e
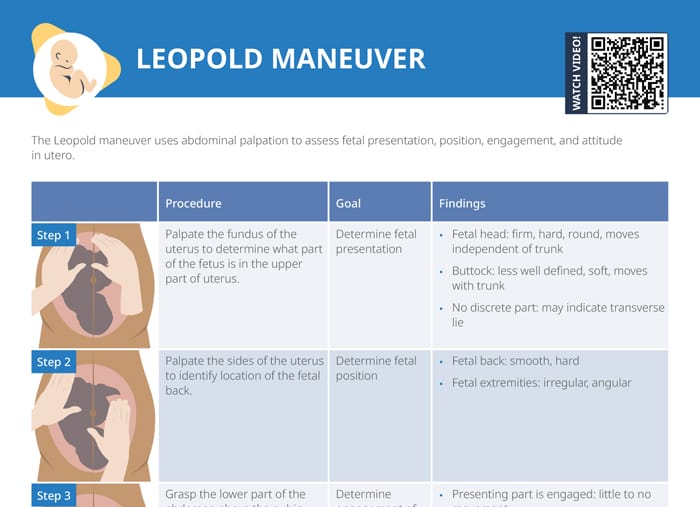
Clinical Reference Chart - Leopold Maneuvers
Step-by-Step Guide
MANEUVER 1 - Fundal Grip (What is in the fundus?)
Examiner faces maternal head
How: Place both hands on either side of the uterine fundus, fingers close together near the xiphoid. Gently palpate with fingertips.
| Finding | Interpretation |
|---|---|
| Hard, round, smooth, ballottable | Fetal head → breech presentation |
| Soft, irregular, less distinct, moves with trunk | Fetal buttocks → vertex (head down) presentation |
| No distinct fetal pole | Possible transverse lie |
Also used to estimate gestational age by fundal height (McDonald's rule).
MANEUVER 2 - Lateral/Umbilical Grip (Where is the fetal back?)
Examiner faces maternal head
How: Slide hands down from fundus to the lateral walls of the uterus. Stabilize one side while palpating the opposite side with the other hand. Alternate sides.
| Finding | Interpretation |
|---|---|
| Smooth, hard, continuous, convex surface | Fetal back |
| Irregular, knobby, multiple small parts | Fetal limbs / small parts |
The back and limbs are on opposite sides. Fetal heart tones are best auscultated over the fetal back.
MANEUVER 3 - Pawlik's Grip / Lower Pole Grip (What is the presenting part?)
Examiner faces maternal head
How: Cup the lower abdomen just above the pubic symphysis with one hand (or both hands) and gently grasp the presenting part. Move it gently from side to side.
| Finding | Interpretation |
|---|---|
| Round, hard, smooth, can be ballotted (moves independently) | Head (vertex) - not yet engaged |
| Irregular, soft, not ballottable | Breech |
| No presenting part palpable | Head may be deeply engaged |
MANEUVER 4 - Pelvic Grip (Is the head flexed? Degree of engagement?)
Examiner TURNS 180° to face maternal feet
How: Place both hands on either side of the lower uterus, fingers pointing toward the pelvis. Press downward and inward.
| Finding | Interpretation |
|---|---|
| One hand meets resistance first (cephalic prominence on one side) | Head is flexed (well-flexed = normal vertex) if prominence is on same side as small parts (limbs) |
| Cephalic prominence on back side | Head is extended (face/brow presentation) |
| Both hands meet equal resistance | Head is military attitude (neither flexed nor extended) |
| Hands converge into pelvis | Head is deeply engaged |
Fetal Positions and Heart Tone Locations
| Fetal Position | Best FHR Auscultation Location |
|---|---|
| Left Occiput Anterior (LOA) - most common | Left lower quadrant, below umbilicus |
| Right Occiput Anterior (ROA) | Right lower quadrant, below umbilicus |
| Left Occiput Posterior (LOP) | Left lateral, near flank |
| Breech | Above umbilicus (periumbilical) |
| Transverse lie | Level of umbilicus, on side of fetal back |
📋 Symphysis-Fundal Height (SFH) Measurement - Technique
- Patient supine (left tilt if >28 wks)
- Locate the superior border of the pubic symphysis with one end of the tape
- Run the tape over the uterine contour to the top of the fundus (not the skin fold)
- Read the measurement in centimeters
- Plot on a customized growth chart
Normal: SFH (cm) = gestational age in weeks ± 2 cm
| SFH Result | Consider |
|---|---|
| > expected by >2-4 cm | Polyhydramnios, multiple gestation, LGA, wrong dates, fibroids |
| < expected by >2-4 cm | FGR, oligohydramnios, wrong dates, fetal demise, transverse lie |
⚠️ Contraindications & Limitations
Conditions reducing Leopold accuracy:
- Maternal obesity (BMI >35)
- Polyhydramnios (excess fluid)
- Anterior placenta praevia
- Multiple gestation
- Engaged head (makes palpation difficult)
- Patient discomfort / non-cooperation
Contraindications to vigorous palpation:
- Placenta praevia (confirmed)
- Active preterm labor
- Premature rupture of membranes (use caution)
Ultrasound is the gold standard for confirming fetal presentation when any malpresentation is suspected, and is recommended when Leopold findings are uncertain.
🩺 Summary Table: Trimester-by-Trimester Abdominal Exam
| Feature | 1st Trimester (0-13 wks) | 2nd Trimester (14-27 wks) | 3rd Trimester (28-40 wks) |
|---|---|---|---|
| Uterus palpable | From 12 wks (pubic level) | Yes - rising abdominally | Yes - large |
| Fundal height | Not measurable | From 20 wks (SFH in cm ≈ wks) | Continuous monitoring |
| Fetal parts felt | No | From ~24 wks | Yes - clear |
| Leopold maneuvers | Not applicable | Limited value | Full 4 maneuvers from 30 wks |
| Fetal heart - Doppler | From 10-12 wks | Yes | Yes |
| Fetal heart - Pinard | No | From ~20-24 wks | Yes |
| Position/presentation | N/A | Variable | Document from 30-36 wks |
| Key concern if abnormal | Ectopic, miscarriage | FGR, polyhydramnios | Malpresentation, engagement |
| Patient position | Supine 15-30° | Supine 15-30° | Left lateral tilt |
📚 Sources
- Textbook of Family Medicine, 9e (Rakel) - Figs. 20-2 and 20-3 (fundal growth and Leopold maneuvers diagrams)
- Leopold Maneuvers - StatPearls/NIH - comprehensive clinical technique reference
- Medmastery - Abdominal Exam in Pregnancy - trimester-by-trimester positioning guide
- Peninsula Health Clinical Practice Guideline - Abdominal Palpation in Pregnancy - SFH measurement protocols
This is a shared conversation. Sign in to Orris to start your own chat.