Wound In adult health nursing textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all the information needed for a thorough answer. Note that the library does not contain a dedicated "adult health nursing" textbook, but the surgical and medical textbooks provide excellent coverage of the same wound content. Let me now compose the comprehensive response.
Wound - Adult Health Nursing
Note: The medical library does not contain a dedicated adult health nursing textbook. The content below is drawn from the closest authoritative equivalents - Bailey & Love's Short Practice of Surgery (28th ed.), Schwartz's Principles of Surgery (11th ed.), and Mulholland & Greenfield's Surgery (7th ed.) - which cover all core wound topics taught in adult health nursing programs.
Definition
A wound is a disruption in the continuity of body tissue, resulting from physical, chemical, thermal, or other injury. Understanding wound types, healing mechanisms, and nursing management principles is foundational to adult health nursing practice.
Classification of Wounds
By Etiology (Bailey & Love, 28th ed.)
| Class | Description |
|---|---|
| Surgical/Clean | Intentional, sterile incision |
| Traumatic | Accidental - lacerations, abrasions, crush, blast, bite |
| Burns | Thermal, electrical, chemical, radiation |
| Chronic | Pressure ulcers, vascular ulcers, diabetic ulcers |
By Bacterial Contamination (CDC Surgical Wound Classification)
| Class | Type | Key Features |
|---|---|---|
| I | Clean | Uninfected; no hollow organ entered; primarily closed |
| II | Clean-contaminated | Hollow organ entered under controlled conditions; no unusual contamination |
| III | Contaminated | Open/fresh accidental wounds; major sterile technique breaks; gross GI spillage |
| IV | Dirty | Old traumatic wounds with devitalized tissue; clinical infection or perforated viscera present |
By Depth
- Epidermal
- Dermal (superficial or deep)
- Full-thickness (subcutaneous/fascial/muscle involvement)
By Complexity
- Simple
- Complex (significant soft-tissue loss, open fracture/joint, visceral involvement)
- Complicated (infection, necrosis, haematoma, gas gangrene, compartment syndrome)
Phases of Wound Healing
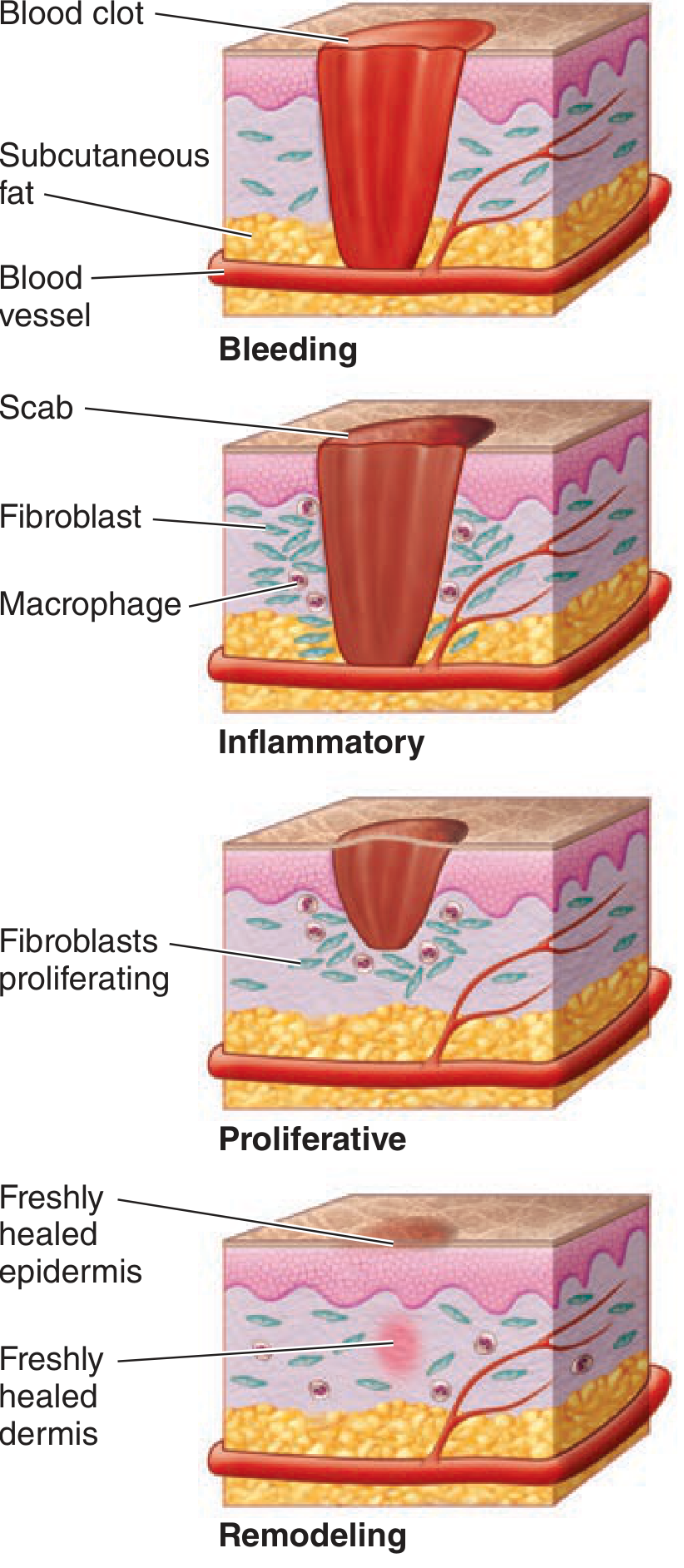
Figure: The four phases of wound healing (Schwartz's Principles of Surgery, 11th ed.)
Wound healing is a continuous, overlapping process spanning up to 12 months. According to Schwartz's Principles of Surgery, there are three major phases (some texts divide into four):
Phase 1: Hemostasis (Minutes to Hours)
- Immediately follows injury
- Damaged blood vessels constrict (vasoconstriction via catecholamines, prostaglandins)
- Platelets aggregate and degranulate, releasing:
- Platelet-derived growth factor (PDGF)
- Transforming growth factor-beta (TGF-β)
- Vascular endothelial growth factor (VEGF)
- Fibronectin, serotonin, platelet-activating factor (PAF)
- Coagulation cascade activated → fibrin clot forms
- Fibrin clot acts as scaffold for incoming inflammatory cells
- Result: bleeding controlled, healing initiated
Phase 2: Inflammation (Days 1-4)
Classically described by: rubor (redness), tumor (swelling), calor (heat), dolor (pain).
Neutrophils (PMNs):
- First cells to arrive; peak at 24-48 hours
- Primary role: phagocytosis of bacteria and debris
- Release cytokines (TNF-α, IL-1) and proteases (collagenases)
- Stimulated by: complement factors, IL-1, TNF-α, TGF-β
Macrophages:
- Derived from circulating monocytes
- Peak at 48-96 hours; remain until healing complete
- Central regulators: release TGF-β, VEGF, IGF, EGF, lactate
- Direct fibroblast proliferation, angiogenesis, and matrix synthesis
- Essential to successful healing - without macrophages, healing fails
Phase 3: Proliferation / Fibroplastic Phase (Days 3 - Weeks 3-4)
Starts around day 3 and lasts 2-4 weeks. Key processes:
Fibroblast activity:
- Fibroblasts migrate into the wound and produce collagen (initially type III, later type I)
- Collagen synthesis requires: oxygen, vitamin C (cofactor for prolyl hydroxylase), iron, amino acids
- Ground substance laid down: glycosaminoglycans and proteoglycans
Granulation tissue:
- Pink, granular tissue formed in early proliferative phase
- Composed of new capillaries (angiogenesis), fibroblasts, and provisional matrix
Angiogenesis:
- New blood vessels form to supply oxygen and nutrients to the healing wound
Epithelialization:
- Begins within 24 hours of injury
- Marginal basal cells migrate across the wound surface
- Complete in <48 hours for approximated incisions; longer for open wounds
- Re-establishes the epidermal barrier
Wound contraction:
- Myofibroblasts (fibroblasts with actin microfilaments) cause wound edges to pull inward
- Particularly prominent in wounds healing by secondary intention
Phase 4: Maturation and Remodeling (Weeks to Months - up to 1 Year)
- Collagen type III replaced by stronger collagen type I
- Matrix metalloproteinases (MMPs) break down and reorganize collagen
- TGF-β increases new collagen transcription AND inhibits breakdown
- Wound progressively becomes avascular and acellular
- Tensile strength increases over months but never reaches that of uninjured tissue
- Scar remodeling continues for 6-12 months
Types of Wound Healing (Intention)
| Type | Description | Clinical Example |
|---|---|---|
| Primary intention (1st intention) | Wound edges directly approximated; minimal tissue loss | Surgical incision closed with sutures |
| Secondary intention (2nd intention) | Wound left open; heals by granulation, contraction, and re-epithelialization | Infected wound, large open wound |
| Tertiary intention (Delayed primary closure) | Wound initially left open, then surgically closed when clean | Contaminated wound debrided, closed after 4-5 days |
- Bailey & Love, 28th ed.: "Primary healing is also known as healing by first intention. This occurs when there is direct approximation of the wound edges and is the aim of treatment."
Factors Affecting Wound Healing
Local Factors
- Skin tension
- Hypoxia and ischaemia
- Vascular insufficiency
- Lymphoedema
- Contamination and infection
- Presence of foreign bodies
- Radiotherapy
Systemic Factors
- Advancing age
- Obesity
- Malnutrition (especially protein, vitamin C, zinc deficiency)
- Smoking (reduces tissue oxygenation)
- Diabetes mellitus (impairs neutrophil function, microvascular disease)
- Immunocompromised states (HIV/AIDS)
- Medications: corticosteroids, immunosuppressants, chemotherapy
Abnormal Wound Healing
Hypertrophic Scars
- Excess collagen in a parallel arrangement
- Do NOT extend beyond original wound boundary
- Eventually regress spontaneously
- More common in: high-tension areas, wounds crossing tension lines, deep dermal burns, wounds healing by secondary intention >3 weeks
Keloid Scars
- Excess collagen in a disorganised arrangement
- Extend beyond original wound boundary
- Do NOT regress spontaneously - difficult to treat
- Genetic predisposition; more common in darker skin pigmentation
- Can result from relatively minor trauma
Chronic / Non-healing Wounds
- Failure to progress through normal healing phases
- Causes: persistent infection, ischaemia, pressure, underlying disease (diabetes, venous insufficiency)
- Examples: pressure ulcers, venous leg ulcers, diabetic foot ulcers
Wound Management Principles
| Stage | Actions |
|---|---|
| Preparation | Antibiotic prophylaxis (for contaminated/dirty wounds), tetanus prophylaxis, adequate analgesia/anaesthesia, wound irrigation |
| Wound | Early debridement (excise non-viable tissue until healthy bleeding), exploration, repair structures, haemostasis |
| Closure | Skin closure without tension, reconstruction options, appropriate suture choice, drains, optimal dressings |
| Follow-up | Suture/splint removal, physiotherapy, monitoring for complications, scar management |
Tetanus-Prone Wounds (Bailey & Love, 28th ed.)
- Puncture injuries in contaminated environments
- Bites
- Compound fractures
- Wounds containing foreign bodies
- Burns/wounds with systemic sepsis
- High-risk: heavy contamination (soil/manure), surgical delay >6 hours, extensive devitalized tissue
Debridement
- Removes all devitalized tissue and foreign material
- Non-viable tissue excised until healthy bleeding occurs at wound edges
- Methods: surgical, mechanical, enzymatic, autolytic (moist dressings), biological (maggot therapy)
Wound Assessment (Nursing)
Key assessment parameters for a wound include:
- Location - anatomical site
- Size - length × width × depth (cm)
- Wound bed - color: red (granulating), yellow (slough), black (necrotic)
- Exudate - amount, color, consistency, odor
- Wound edges - attached/unattached, rolled/undermined
- Periwound skin - erythema, maceration, induration
- Signs of infection - erythema, warmth, purulent discharge, odor, fever, increased pain
- Pain - at rest and during dressing changes
Sources:
- Bailey and Love's Short Practice of Surgery, 28th ed., Chapter 3 (Wound Healing & Management)
- Schwartz's Principles of Surgery, 11th ed., Chapter 9 (Wound Healing)
- Mulholland and Greenfield's Surgery, 7th ed., Chapter on Wound Management
Can you prepare Wound definition Types Etiology Clinical manifestations Pathophysiology Diagnostic measures Complications Prognosis Management *medical *Surgical - pre operative order, *surgical note,post operative orders Nursing management assessment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
WOUND - Adult Health Nursing
Sources: Bailey & Love's Short Practice of Surgery (28th ed.) | Schwartz's Principles of Surgery (11th ed.) | Sabiston Textbook of Surgery | Pfenninger & Fowler's Procedures for Primary Care (3rd ed.)
1. DEFINITION
A wound is any disruption in the normal continuity of body structures - skin, mucous membrane, or organ tissue - caused by physical, mechanical, chemical, thermal, or pathological processes.
More specifically:
- It is a break in the epithelial integrity of the skin, with or without involvement of deeper structures (dermis, subcutaneous tissue, muscle, bone, viscera)
- Wounds may be intentional (surgical incisions) or unintentional (traumatic injuries)
- A wound that fails to progress through normal healing in an orderly, timely manner is classified as a chronic wound
2. TYPES OF WOUNDS
A. By Mechanism / Etiology
| Type | Description |
|---|---|
| Incised wound | Clean cut by a sharp instrument (scalpel, knife, glass) |
| Laceration | Irregular tear of tissue by blunt force |
| Contusion | Bruising; intact skin with underlying tissue damage |
| Abrasion | Superficial scraping of skin (epidermis only) |
| Puncture | Deep, narrow wound from a sharp pointed object |
| Avulsion | Forcible tearing away of tissue |
| Crush wound | Tissue compressed between two forces; may have minimal skin break |
| Burn wound | Thermal, chemical, electrical, or radiation injury |
| Bite wound | Human or animal; highly contaminated |
| Degloving | Avulsion of skin and subcutaneous fat from underlying fascia/muscle/bone |
B. By Skin Integrity
| Type | Description |
|---|---|
| Open wound | Skin or mucosa is broken; tissue exposed to environment |
| Closed wound | Skin intact; damage to underlying tissue (contusion, haematoma) |
C. By Bacterial Contamination (CDC Classification) - Bailey & Love
| Class | Category | Features |
|---|---|---|
| I | Clean | Uninfected; no hollow organ entered; primarily closed |
| II | Clean-contaminated | Hollow organ entered under controlled conditions; no infection |
| III | Contaminated | Open fresh accidental wounds; gross GI spillage; acute non-purulent inflammation |
| IV | Dirty | Old wounds with devitalized tissue; existing clinical infection or perforated viscera |
D. By Duration
| Type | Description |
|---|---|
| Acute wound | Heals in expected time frame (days to weeks) |
| Chronic wound | Fails to heal in orderly/timely manner; stalled in inflammation (>4-6 weeks without progress) |
Chronic wound examples: pressure ulcers, venous leg ulcers, diabetic foot ulcers, arterial ulcers
E. By Depth
- Superficial - epidermis only
- Partial-thickness - epidermis + superficial dermis
- Full-thickness - epidermis + dermis + subcutaneous tissue
- Deep - involves fascia, muscle, tendon, bone, or viscera
3. ETIOLOGY
| Category | Causes |
|---|---|
| Traumatic | Road traffic accidents, falls, assaults, industrial injuries, bites, gunshot wounds |
| Surgical | Intentional operative incisions |
| Thermal | Burns (heat, cold/frostbite) |
| Chemical | Acids, alkalis, caustic substances |
| Electrical | Electrical current - entry and exit wounds |
| Radiation | Radiation therapy-induced wound breakdown |
| Pathological / Vascular | Arterial insufficiency, venous hypertension (ulcers) |
| Pressure | Sustained pressure over bony prominences causing ischaemic necrosis (pressure ulcers) |
| Diabetic / Neuropathic | Loss of protective sensation + microangiopathy |
| Malignant | Tumour invasion/ulceration through skin |
| Iatrogenic | Extravasation injuries, line-site wounds, post-procedure |
4. CLINICAL MANIFESTATIONS
Local Signs
| Sign | Description |
|---|---|
| Pain / Tenderness | Variable depending on wound depth and nerve involvement; absent in neuropathic wounds |
| Bleeding / Haemorrhage | Active in acute wounds; may be occult in closed wounds |
| Tissue disruption | Visible break, loss of tissue continuity, exposed structures |
| Swelling / Oedema | Localised, due to inflammatory response |
| Erythema | Redness around wound margin (normal up to 0.5-1 cm); >2 cm suggests infection |
| Warmth (Calor) | Local heat due to increased vascularity |
| Exudate / Discharge | Serous (clear, normal), sanguineous (bloody), serosanguineous (pink), purulent (infection) |
| Odour | Malodour suggests infection or necrosis (Pseudomonas - fruity; anaerobes - fetid) |
| Skin discoloration | Bruising (ecchymosis) in closed injuries; necrosis (black/brown eschar) in severe wounds |
| Wound bed appearance | Red (granulating), yellow (slough), black (necrotic) |
Signs of Wound Infection (NERDS/STONEES Criteria)
Superficial infection (NERDS):
- N - Non-healing wound
- E - Exudate increasing
- R - Red/bleeding wound bed
- D - Debris (slough/tissue) on wound
- S - Smell/odour from wound
Deep infection (STONEES):
- S - Size increasing
- T - Temperature elevated (local and systemic)
- O - Os (bone) exposed
- N - New areas of breakdown
- E - Erythema/oedema
- E - Exudate (purulent)
- S - Smell
Systemic Manifestations (if infected)
- Fever (>38°C), chills, rigors
- Tachycardia, tachypnoea
- Elevated WBC (leukocytosis)
- Fatigue, malaise
- Sepsis/septic shock in severe cases
5. PATHOPHYSIOLOGY
Normal Wound Healing - Four Overlapping Phases
(Schwartz's Principles of Surgery, Sabiston Textbook of Surgery)
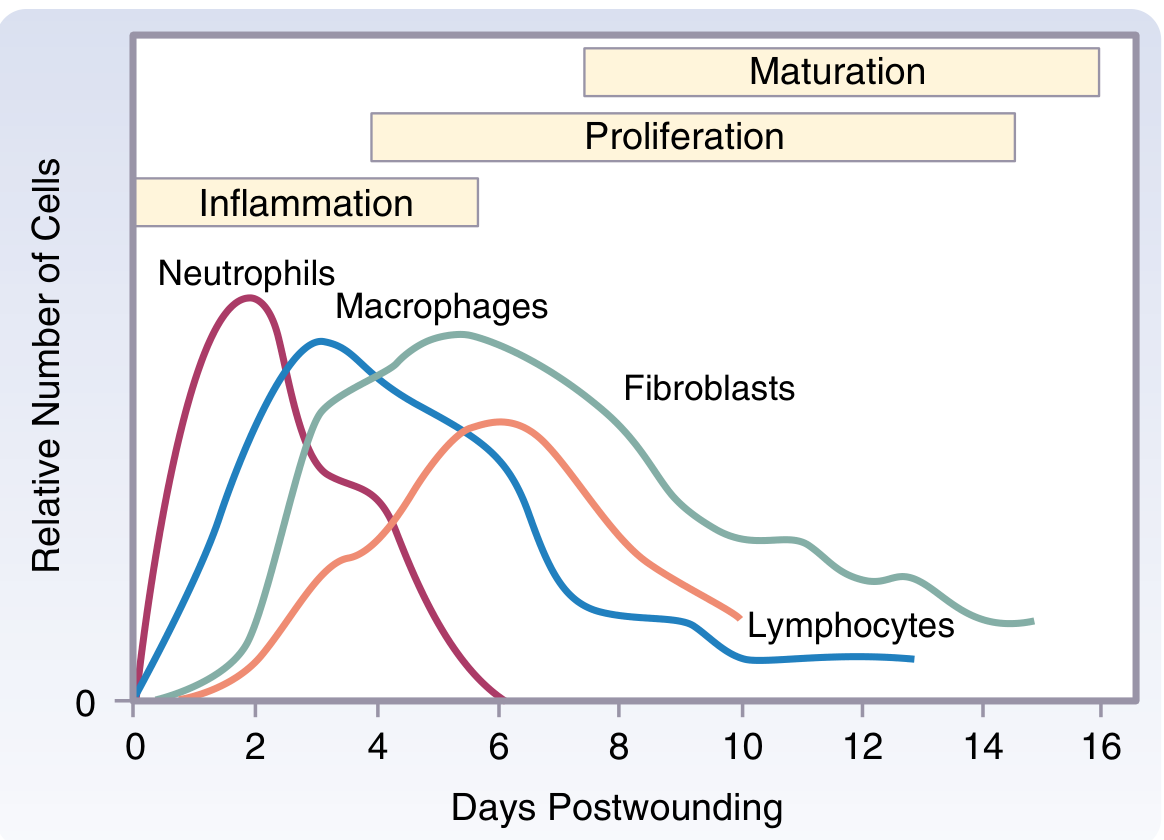
Cell sequence during wound healing: neutrophils peak Day 2, macrophages Day 3, lymphocytes Day 7, fibroblasts throughout proliferative phase (Sabiston Textbook of Surgery)
Phase 1: Hemostasis (0 - Hours)
- Tissue injury → vasoconstriction → platelet aggregation and degranulation
- Platelets release: PDGF, TGF-β, VEGF, fibronectin, serotonin
- Coagulation cascade activated → fibrin clot formed
- Fibrin clot = physical barrier to blood loss AND scaffold for healing cells
Phase 2: Inflammation (Hours - Day 4)
- Vasodilation and increased vascular permeability
- Classic signs: Rubor (red), Tumor (swelling), Calor (heat), Dolor (pain)
- Neutrophils (PMNs): First responders; peak 24-48 hours; phagocytose bacteria and debris; release cytokines (TNF-α, IL-1) and proteases
- Macrophages: Peak 48-96 hours; phagocytosis + regulation of repair; release TGF-β, VEGF, EGF, IGF; essential to coordinated healing
Phase 3: Proliferation (Day 3 - Week 3-4)
- Fibroblasts proliferate and synthesize collagen (type III initially, then type I) and ground substance
- Granulation tissue forms: pink, vascular, granular tissue filling the wound bed
- Angiogenesis: New capillary formation supplies oxygen and nutrients
- Epithelialization: Marginal basal cells migrate across wound surface; begins within 24 hours; complete in <48 hours for closed incisions
- Wound contraction: Myofibroblasts pull wound edges inward (prominent in secondary intention healing)
- Collagen synthesis requires: oxygen, vitamin C, iron, zinc, protein
Phase 4: Maturation and Remodeling (Weeks - 12 Months)
- Collagen type III → replaced by stronger type I collagen
- Matrix metalloproteinases (MMPs) continuously remodel collagen
- TGF-β controls balance of synthesis vs. degradation
- Scar becomes progressively avascular and acellular
- Tensile strength reaches 50% at 3 weeks, 80% at 3 months - never achieves 100% of unwounded tissue
- Scar remodeling continues 6-12 months
Chronic Wound Pathophysiology
- Persistent inflammation → proteases (MMPs) overwhelm new tissue formation
- Biofilm formation → impairs host defenses
- Ischaemia/hypoxia → cells cannot sustain proliferation
- Healing remains "stuck" in inflammatory phase
6. DIAGNOSTIC MEASURES
Laboratory
| Test | Purpose |
|---|---|
| CBC (Complete Blood Count) | WBC elevated in infection; Hgb/Hct for blood loss |
| Blood glucose / HbA1c | Identify diabetes as underlying factor |
| Serum albumin / Pre-albumin | Nutritional status; low albumin impairs healing |
| Coagulation studies (PT, aPTT) | Assess bleeding tendency |
| CRP / ESR / Procalcitonin | Markers of systemic infection/inflammation |
| Blood cultures | If systemic sepsis suspected |
| Wound swab / culture and sensitivity | Identify causative organism; guide antibiotic therapy - surface swab (Levine technique) or tissue biopsy (gold standard: >10^5 organisms/g tissue = infection) |
| Bone biopsy | If osteomyelitis suspected |
Imaging
| Study | Indication |
|---|---|
| X-ray | Foreign body detection, underlying fracture, osteomyelitis (late changes) |
| Ultrasound | Fluid collections, abscess, vascular insufficiency (Doppler) |
| CT scan | Deep infection, necrotizing fasciitis, foreign bodies, complex wounds |
| MRI | Osteomyelitis (most sensitive), soft tissue extent |
| Ankle-Brachial Index (ABI) | Assess arterial perfusion in leg wounds (ABI <0.8 = arterial insufficiency) |
| Duplex ultrasound | Venous or arterial disease assessment |
Wound-Specific Assessment Tools
| Tool | Use |
|---|---|
| Wound measurement | Length × width × depth; undermining/tunneling |
| Wound photography | Serial photos to document progress |
| PUSH Tool | Pressure Ulcer Scale for Healing |
| Bates-Jensen Wound Assessment Tool (BWAT) | Comprehensive chronic wound scoring |
| Ankle-Brachial Index | Leg wound vascular assessment |
7. COMPLICATIONS
| Complication | Description |
|---|---|
| Wound infection / Surgical Site Infection (SSI) | Most common; superficial, deep, or organ/space |
| Wound dehiscence | Partial or complete disruption of wound edges; risk factors: infection, obesity, diabetes, malnutrition, poor suturing technique |
| Evisceration | Extrusion of abdominal contents through dehisced wound; surgical emergency |
| Haematoma | Collection of blood in wound; risk of infection, pressure necrosis |
| Seroma | Collection of serous fluid; impairs healing, risk of infection |
| Abscess formation | Loculated pus requiring drainage |
| Fistula formation | Abnormal tract between wound and another epithelial surface |
| Necrotizing fasciitis | Rapidly spreading infection of fascia/subcutaneous tissue; life-threatening |
| Gas gangrene (Clostridial myonecrosis) | Clostridium perfringens; crepitus, severe pain, systemic toxicity |
| Hypertrophic scar | Raised scar within original wound boundary; may regress |
| Keloid | Raised scar extending beyond original wound; does not regress; more common in dark skin |
| Contracture | Scar shortening across joints → limits range of motion |
| Chronic non-healing wound | Stalled healing >4-6 weeks |
| Malignant transformation | Marjolin's ulcer - SCC developing in chronic wound/scar |
| Osteomyelitis | Bone infection from chronic or deep wound |
| Sepsis / Septic shock | Systemic infection spread; life-threatening |
| Tetanus | From tetanus-prone wounds in non-immunized patients |
8. PROGNOSIS
Prognosis depends on multiple factors:
| Factor | Impact |
|---|---|
| Wound type/size | Small, clean wounds heal quickly; large/complex wounds take longer |
| Blood supply | Adequate perfusion essential; ischaemic wounds heal poorly |
| Age | Elderly patients have delayed healing |
| Diabetes mellitus | Significantly impairs healing; high risk of amputation |
| Infection | Delays healing; if systemic, worsens overall prognosis |
| Nutrition | Protein and micronutrient deficiency impairs all phases |
| Immunosuppression | Chemotherapy, steroids, HIV increase infection risk |
| Smoking | Reduces tissue oxygenation; delays healing 40-50% |
| Radiation | Impairs vascularity permanently |
| Patient compliance | Adherence to dressing changes, offloading, glucose control |
General prognosis:
- Simple acute wounds in healthy adults: heal well within 2-4 weeks
- Chronic wounds (venous ulcers): 40-70% healed at 24 weeks with optimal care
- Diabetic foot ulcers: 5-year recurrence rate >50%
- Infected wounds with sepsis: mortality increases significantly (septic shock mortality 20-40%)
9. MANAGEMENT
A. MEDICAL MANAGEMENT
1. Wound Irrigation and Cleaning
- Warm normal saline is the standard irrigant
- High-pressure irrigation (20 mL syringe, 19G needle) for contaminated wounds
- Antiseptic solutions (Betadine, chlorhexidine) used with caution - cytotoxic to healing cells at full strength
2. Debridement (Bailey & Love, 28th ed.)
| Method | Description |
|---|---|
| Surgical | Scalpel/scissors excision of non-viable tissue until healthy bleeding; gold standard |
| Mechanical | Wet-to-dry dressings, irrigation, hydrotherapy; non-selective |
| Autolytic | Hydrocolloid/hydrogel dressings - wound enzymes liquefy necrotic tissue; selective, painless |
| Enzymatic | Topical collagenase or papain-urea; chemically liquefies necrotic tissue |
| Biological (Larval therapy) | Medical-grade maggots of Lucilia sericata; produce proteolytic and antimicrobial substances |
3. Wound Dressings (Pfenninger & Fowler's)
| Wound Type | Dressing Goal | Recommended Dressing |
|---|---|---|
| Incisional/Surgical | Protect, immobilize edges | Steri-Strips, low-adherent dressing, semipermeable film |
| Partial-thickness | Facilitate epithelialization, absorb exudate | Foam, hydrocolloid, antibiotic cream + gauze |
| Full-thickness/Dehisced | Maintain moisture, absorb, debride | Hydrogel, alginate, foam, NPWT (VAC) |
| Heavy necrotic load | Debridement, absorb | Larval therapy, VAC dressing |
| Malignant wound | Moisture, odour control | Foam, metronidazole gel, activated charcoal dressing |
Moist wound healing principle: A moist wound environment promotes faster epithelialization and reduces pain (vs. dry dressings)
4. Pharmacological Treatment
| Agent | Indication / Use |
|---|---|
| Antibiotics | Systemic for cellulitis/deep infection; topical for surface colonization |
| Tetanus prophylaxis | All tetanus-prone wounds (see tetanus table) |
| Analgesics | Pain control; important before dressing changes |
| NSAIDs | Reduce inflammation and fever |
| Corticosteroids | AVOID in acute wounds (impair healing); used in keloid management |
| Vitamin C | Cofactor for collagen synthesis; supplement if deficient |
| Zinc | Cofactor for healing; supplement if deficient |
| Insulin / Glycaemic control | Diabetic wounds - target HbA1c <7% |
| Anticoagulants | Prevent DVT in immobile/post-op patients with wounds |
5. Advanced Medical Therapies
| Therapy | Mechanism |
|---|---|
| Negative-Pressure Wound Therapy (NPWT/VAC) | Sub-atmospheric pressure draws wound edges together, removes exudate, reduces oedema, promotes granulation tissue |
| Hyperbaric Oxygen Therapy (HBO) | Increases tissue PO2; promotes angiogenesis and collagen synthesis; used for diabetic foot ulcers, radiation wounds, osteomyelitis |
| Biological/Growth factor therapy | Becaplermin (PDGF) gel for diabetic neuropathic ulcers |
| Skin substitutes | Bioengineered skin for large or non-healing wounds |
B. SURGICAL MANAGEMENT
PRE-OPERATIVE ORDERS
PHYSICIAN'S ORDERS - PRE-OPERATIVE
Patient Name: _______________ Date: ____________ Time: ______
Diagnosis: Wound requiring surgical intervention
Procedure: Wound debridement / Wound exploration / Wound closure / Skin graft
1. NOTHING BY MOUTH (NPO)
- NPO after midnight (or 6 hours before procedure for solids,
2 hours for clear liquids per anaesthesia guidelines)
2. LABORATORY INVESTIGATIONS
- CBC with differential
- BMP (Basic Metabolic Panel): BUN, Creatinine, Electrolytes
- Fasting blood glucose / HbA1c (if diabetic)
- PT / INR / aPTT
- Blood group and crossmatch / type and screen
- Serum albumin / Pre-albumin
- Blood cultures x2 (if signs of systemic infection)
- Wound swab for C&S
3. IMAGING
- X-ray of affected area (if foreign body or fracture suspected)
- Doppler ultrasound (if vascular compromise suspected)
4. IV ACCESS
- Insert peripheral IV line (18G or 16G)
- IV fluids: Lactated Ringer's / Normal Saline 0.9% at
___ mL/hr (maintenance rate)
5. MEDICATIONS
- Antibiotic prophylaxis: Cefazolin 2g IV 30-60 minutes
before incision (adjust dose: 3g if weight >120 kg)
- (If penicillin allergy: Clindamycin 900 mg IV OR
Vancomycin 15-20 mg/kg IV)
- Continue home medications EXCEPT:
• Hold anticoagulants (as per physician order)
• Hold metformin 24-48 hours pre-op
• Hold ACE inhibitors / ARBs on day of surgery
6. TETANUS PROPHYLAXIS
- Review immunisation status
- Tetanus toxoid 0.5 mL IM if indicated
- Tetanus immunoglobulin (TIG) 250 IU IM if high-risk wound
and incomplete immunisation
7. ANAESTHESIA CONSULT
- Anaesthesiology review required
8. SKIN PREPARATION
- Clip hair (do not shave) in operative field as needed
- Do NOT apply skin prep until in OR
9. CONSENT
- Informed consent obtained and signed
10. PRE-OP CHECKLIST
- Allergy identification band applied
- Surgical site marked by surgeon
- Remove jewellery, nail polish, prosthetics
- Patient identification confirmed x2 (name + DOB)
Physician Signature: _____________ Time: ______
SURGICAL (OPERATIVE) NOTE
OPERATIVE / SURGICAL NOTE
Date: ____________ Time of procedure: _______ to _______
Surgeon: _______________ Assistant: _______________
Anaesthesiologist: _______________
Anaesthesia type: [ ] General [ ] Regional [ ] Local [ ] MAC
PATIENT: _______________ DOB: _______________
MRN: _______________
PRE-OPERATIVE DIAGNOSIS:
Wound: [specify type, location, size, classification]
e.g., Contaminated traumatic wound, right forearm, 8 x 3 cm
Full-thickness; devitalized tissue; no vascular compromise
POST-OPERATIVE DIAGNOSIS:
[Same / or revised findings]
PROCEDURE PERFORMED:
e.g., Wound exploration, debridement, and primary closure
/ Split-thickness skin graft / Flap coverage
ESTIMATED BLOOD LOSS (EBL): ___ mL
FLUIDS ADMINISTERED: ___ mL (type: ___)
URINE OUTPUT: ___ mL
SPECIMEN SENT: [ ] Wound culture [ ] Tissue biopsy [ ] None
PROCEDURE IN DETAIL:
- Patient positioned: _______________
- Surgical site prepped with ___ (e.g., 2% chlorhexidine
in 70% isopropyl alcohol) and draped in sterile fashion
- Tourniquet applied at ___ mmHg / not used
- Wound explored: extent of injury - [describe layers
involved: dermis / subcutaneous / fascia / muscle /
tendon / bone; neurovascular status]
- Non-viable tissue identified: [colour, texture, amount]
- Debridement performed: [surgical excision of ___ cm²
of devitalized tissue until healthy bleeding margins
obtained]
- Wound irrigated with [saline/betadine] x ___ litres
under pressure
- Haemostasis achieved: [electrocautery / ligation /
pressure]
- Repair of structures: [tendons, vessels, nerves if
applicable]
- Wound closed: [primary / secondary / tertiary intention]
- Deep layers: Vicryl [size] interrupted sutures
- Subcutaneous: Vicryl [size]
- Skin: [nylon / staples / Steri-Strips / skin glue]
- Drain placed: [ ] Yes - type ___ at ___ location
[ ] No
- Dressing applied: [specify type]
- Tourniquet released; circulation confirmed distal to wound
COMPLICATIONS: None / [list if any]
PATIENT CONDITION: Stable / [note any concerns]
PLAN: [Post-op wound care, follow-up, further procedures]
Surgeon Signature: _______________ Date: _______________
POST-OPERATIVE ORDERS
PHYSICIAN'S ORDERS - POST-OPERATIVE
Patient Name: _______________ Date: ____________ Time: ______
Procedure Performed: _______________
Post-op Diagnosis: _______________
1. VITAL SIGNS
- Every 15 minutes x 4, then every 30 min x 2, then
every 1 hour x 4, then every 4 hours (or per unit
protocol)
- Notify physician if:
• Temperature > 38.5°C or < 36°C
• HR > 100 or < 60 bpm
• SBP > 160 or < 90 mmHg
• SpO2 < 94%
• Increasing pain / wound drainage
2. MONITORING
- Continuous cardiac/SpO2 monitoring until stable
- Intake and output every 4 hours
- Blood glucose monitoring every 4-6 hours
(especially if diabetic)
3. ACTIVITY
- Bed rest for ___ hours post-op
- Elevate affected limb above heart level (if applicable)
- Ambulate when fully recovered from anaesthesia
(with assistance x first time)
- No weight bearing on ___ extremity until further
assessment
4. DIET
- Clear liquids when fully awake and bowel sounds present
- Advance to regular diet as tolerated
- High-protein diet encouraged to promote wound healing
5. IV FLUIDS
- Continue IV [NS / LR] at ___ mL/hr
- D/C IV fluids when tolerating oral intake
6. WOUND CARE
- Leave initial dressing intact for 24-48 hours
unless saturated/soiled
- Inspect wound every shift: note colour, temperature,
exudate type and amount, odour, surrounding skin
- First dressing change: _____ (date/time) by surgeon/
nurse per protocol
- Wound care orders: [specify dressing type, frequency]
- NPWT settings if applicable: ___ mmHg continuous/
intermittent
- Drain care: measure output every shift; document colour
and character
- Remove drain when output < 30 mL/24 hours (or per
surgeon order)
7. MEDICATIONS
a. Pain Management:
- Morphine / Hydromorphone PCA: [dose/lockout settings]
OR
- Ketorolac 15-30 mg IV every 6 hours x 5 doses, then
- Paracetamol (Acetaminophen) 1 g IV/oral every 6 hours
- Ibuprofen 400 mg oral every 8 hours with food
b. Antibiotics:
- Continue Cefazolin 1g IV every 8 hours x [24-48 hours
for prophylaxis] OR [5-7 days for established infection]
- (Adjust based on culture and sensitivity results)
c. DVT Prophylaxis:
- Enoxaparin 40 mg SC every 24 hours (start 12-24 hrs
post-op when haemostasis confirmed)
AND
- Sequential Compression Device (SCD) to lower
extremities while in bed
d. GI Protection:
- Omeprazole 20 mg oral/IV daily (while on NSAIDs or
stressed patient)
e. Anti-emetics:
- Ondansetron 4 mg IV every 6 hours PRN nausea
f. Glycaemic Control:
- Target blood glucose 140-180 mg/dL
- Insulin sliding scale / basal-bolus insulin as ordered
g. Nutritional Supplements:
- Vitamin C 500 mg oral twice daily
- Zinc sulfate 220 mg oral daily (if deficient)
- Ensure/Boost supplement with meals if intake inadequate
8. SUTURE / STAPLE REMOVAL
- Facial wounds: Day 5-7
- Scalp: Day 7-10
- Trunk / extremities: Day 10-14
- Over joints: Day 14
- Contaminated/complex wounds: per surgeon review
9. FOLLOW-UP
- Wound clinic/outpatient review in ___ days
- Remove drain on Day ___
- Physiotherapy referral if joint/function involved
- Occupational therapy if hand/upper limb involved
10. DOCUMENTATION
- Document wound assessment each shift
- Photograph wound at baseline and with each major change
- Report signs of infection, dehiscence, or unusual
drainage to physician immediately
Physician Signature: _______________ Time: ______
10. NURSING MANAGEMENT
A. NURSING ASSESSMENT
1. Health History
- Mechanism and time of injury (hours since wound occurred)
- Previous wounds, surgeries, or skin conditions
- Tetanus immunisation status
- Allergies (especially to antiseptics, adhesives, latex)
- Current medications (steroids, anticoagulants, immunosuppressants)
- Past medical history: diabetes, vascular disease, connective tissue disorders, malignancy
- Smoking, alcohol, and nutritional status
- Psychosocial factors: living situation, ability to perform self-care
2. Physical Assessment
Wound-Specific (HEAD-TO-TOE, wound-focused):
| Parameter | What to Assess |
|---|---|
| Location | Anatomical site; document using body diagram |
| Size | Length × width × depth in centimetres; use ruler/wound measurement guide |
| Wound bed | % Red (granulation), yellow (slough), black (necrosis) |
| Exudate | Amount (none/scant/moderate/heavy), type (serous/sanguineous/serosanguineous/purulent), odour |
| Wound edges | Attached/unattached; rolled/thickened (chronic); undermining/tunneling (measure clock position and depth) |
| Periwound skin | Erythema (measure extent from wound edge), warmth, induration, maceration, excoriation |
| Wound closure | Sutures/staples: intact, approximated, tension-free; signs of dehiscence |
| Drains | Type, position, output volume, character |
| Signs of infection | Increased pain, erythema >2 cm, warmth, purulent drainage, fever |
Systematic Assessment:
- Vital signs (temperature, HR, BP, RR, SpO2)
- Pain assessment: PQRST (Position, Quality, Radiation, Severity 0-10, Time/triggers)
- Neurovascular assessment distal to wound: pulses, capillary refill, sensation, movement
- Nutritional assessment: weight, BMI, dietary intake, albumin level
- Mobility and function: activity level, ability for self-care
- Psychosocial: anxiety, coping, body image concerns
3. Priority Nursing Diagnoses
| Nursing Diagnosis | Related Factors |
|---|---|
| Impaired tissue integrity | Disruption of skin and tissue continuity |
| Acute/Chronic pain | Tissue damage, inflammation, dressing changes |
| Risk for infection | Break in skin integrity, contamination |
| Impaired physical mobility | Pain, wound location, post-operative restrictions |
| Imbalanced nutrition: less than body requirements | Increased metabolic demands for healing |
| Risk for deficient fluid volume | Blood loss, wound exudate |
| Disturbed body image | Visible wound, scar, disfigurement |
| Knowledge deficit | Wound care, signs of infection, activity restrictions |
| Anxiety | Surgery, wound outcome, disfigurement |
B. NURSING INTERVENTIONS
1. Wound Care
- Perform dressing changes using aseptic/clean technique per hospital protocol
- Irrigate wound with normal saline; use pressure irrigation for contaminated wounds
- Apply appropriate dressing based on wound type and exudate level
- Protect periwound skin from maceration (use skin barrier/zinc oxide)
- Document wound appearance, measurements, and changes each shift
- Photograph wound with patient consent at baseline and regularly
2. Infection Prevention
- Strict hand hygiene before and after wound care
- Maintain sterile/aseptic technique for surgical wounds
- Monitor for SSTI signs every shift; report early indicators promptly
- Administer antibiotics on time; monitor for therapeutic effects
- Teach patient to avoid touching wound; hand hygiene education
3. Pain Management
- Assess pain before, during, and after dressing changes
- Pre-medicate 30-60 minutes before dressing changes (oral analgesia)
- Use non-pharmacological methods: positioning, distraction, relaxation
- Report uncontrolled pain (may indicate wound complication)
4. Nutritional Support
- Collaborate with dietitian for high-protein, high-calorie diet
- Offer protein supplements (Ensure, Boost) if oral intake inadequate
- Ensure adequate vitamin C and zinc intake
- Monitor albumin and pre-albumin levels as healing markers
- Maintain blood glucose <180 mg/dL in diabetic patients
5. Patient and Family Education
| Teaching Topic | Key Points |
|---|---|
| Wound care | Hand hygiene, dressing change technique, supply procurement |
| Signs of infection | When to call healthcare provider: increasing redness, swelling, purulent discharge, fever, increasing pain |
| Activity restrictions | No straining, lifting >2-5 kg, activity limitations per wound site |
| Diet | High protein, vitamin C-rich foods (citrus, leafy greens), zinc (meat, legumes), adequate hydration |
| Follow-up | Importance of keeping appointments; suture/staple removal timing |
| Scar management | Sunscreen protection, silicone gel, massage after complete closure |
| Medication | Completing antibiotic course, analgesic use |
6. Complications Monitoring and Reporting
| Complication | Nurse Action |
|---|---|
| Dehiscence | Cover with sterile moist saline dressing; keep patient supine; notify surgeon immediately |
| Evisceration | Medical emergency - cover bowel with large sterile moist saline dressing; keep NPO; call surgeon STAT |
| Haematoma | Monitor size; apply pressure; notify surgeon if expanding |
| Seroma | Monitor; may require aspiration |
| Infection/SSI | Culture wound; intensify cleaning; notify surgeon; antibiotics |
| Sepsis | Activate sepsis protocol: STAT blood cultures, broad-spectrum antibiotics, IV fluids, escalate care |
C. EVALUATION / EXPECTED OUTCOMES
- Wound dimensions decrease progressively (>30% reduction in 4 weeks = positive indicator)
- Wound bed: progressive granulation tissue formation
- Exudate decreasing in amount; no purulent discharge
- No signs of infection (afebrile, WBC normalizing, wound margins non-erythematous)
- Pain well-controlled (VAS/NRS ≤ 3/10)
- Patient and family demonstrate correct wound care technique
- Patient maintains adequate nutritional intake
- Wound completely closed within expected timeframe
Sources: Bailey and Love's Short Practice of Surgery, 28th ed. | Schwartz's Principles of Surgery, 11th ed. | Sabiston Textbook of Surgery, 21st ed. | Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.