Antivirals drugs pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have extensive data from multiple authoritative textbooks. Let me compile the comprehensive answer.
Antiviral Drugs - Pharmacology
Overview
Viruses replicate inside host cells using host cellular machinery, which makes selective toxicity a major pharmacological challenge. Antiviral drugs must target virus-specific events - viral enzymes, structural proteins, or replication steps - that are distinct from host cell processes. Most antivirals inhibit viral DNA/RNA replication, but targets also include virus entry, uncoating, protein cleavage, and viral release. Importantly, antivirals generally suppress replication rather than eradicate latent infection; once treatment stops, latent virus can reactivate.
- Harrison's Principles of Internal Medicine 22E, p. 1528
Classification by Target Virus
1. Anti-Herpesvirus Drugs
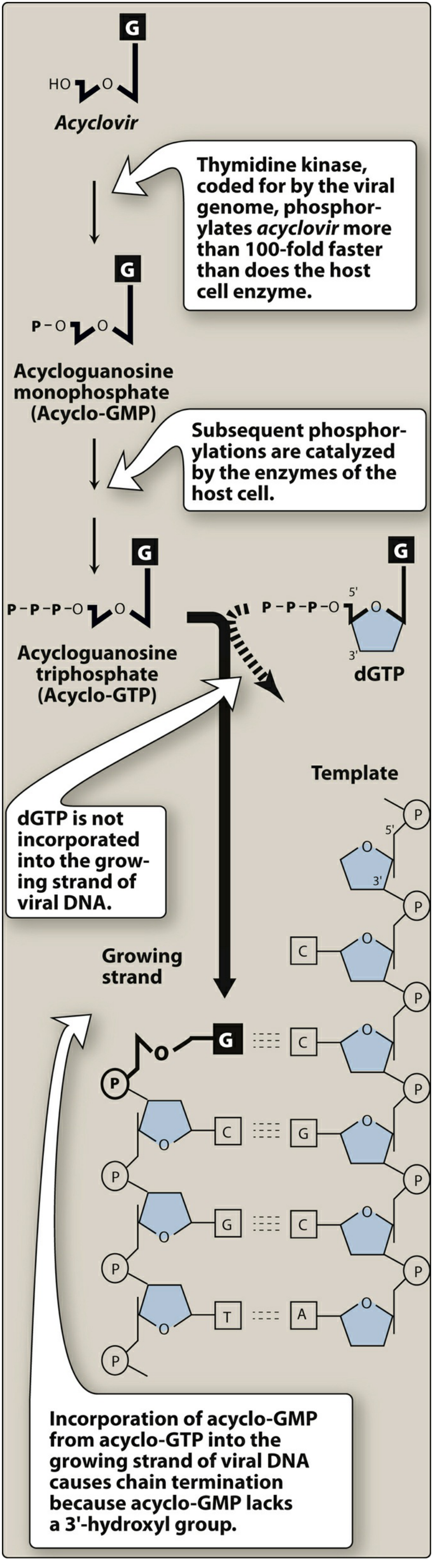
A. Acyclovir (Prototype)
Mechanism of Action (the 2-step selectivity trick):
- Acyclovir is a guanosine analogue with no 3'-hydroxyl group on its acyclic sugar moiety.
- It enters virus-infected cells and is monophosphorylated by viral thymidine kinase - this enzyme phosphorylates acyclovir ~100-fold faster than the host cell enzyme does. Uninfected cells activate very little drug, giving excellent selectivity.
- Host cell kinases then convert it to the triphosphate (Acyclo-GTP), which:
- Competes with deoxyguanosine triphosphate (dGTP) for viral DNA polymerase
- Is incorporated into the growing viral DNA strand
- Causes premature chain termination (lacks 3'-OH needed for next phosphodiester bond)
Spectrum: HSV-1, HSV-2, VZV; limited activity against EBV; poor activity against CMV.
Pharmacokinetics:
- Available IV, oral, topical (topical is much less effective)
- Distributes well including CSF (useful for HSV encephalitis)
- Excreted by glomerular filtration + tubular secretion; dose adjust in renal failure
- Valacyclovir = valine ester prodrug; oral bioavailability ~4x higher; rapidly hydrolyzed to acyclovir in liver/intestine
Adverse effects: Topical: local irritation. Oral: nausea, headache, diarrhea. IV high-dose: transient renal dysfunction (crystalluria - hydration prevents it); rare neurotoxicity.
Resistance: Mutations in viral thymidine kinase (most common) or DNA polymerase. Acyclovir-resistant HSV is treated with foscarnet or cidofovir (which don't require viral TK for activation).
- Lippincott Illustrated Reviews Pharmacology, p. 1122-1124
- Harrison's 22E, p. 1528-1529
B. Valacyclovir and Famciclovir/Penciclovir
| Drug | Key Feature |
|---|---|
| Valacyclovir | Prodrug of acyclovir; much better oral bioavailability; used for HSV, VZV, herpes labialis, suppression of genital HSV |
| Famciclovir | Oral prodrug of penciclovir; similar mechanism; penciclovir triphosphate has a longer intracellular half-life than acyclovir triphosphate |
| Penciclovir | Topical use only for orolabial herpes |
C. Ganciclovir and Valganciclovir
- Ganciclovir is a guanosine analogue structurally similar to acyclovir, differing by one carboxyl side chain - this gives it ~50x more activity against CMV than acyclovir.
- CMV lacks a true thymidine kinase; instead, ganciclovir is phosphorylated by the UL97 protein kinase encoded by CMV.
- Valganciclovir is the oral prodrug (like valacyclovir for acyclovir) with much better bioavailability.
- Key toxicity: myelosuppression (neutropenia, thrombocytopenia) - limits use; also nephrotoxicity.
D. Foscarnet
- Pyrophosphate analogue - directly inhibits viral DNA polymerase and HIV reverse transcriptase at the pyrophosphate-binding site, without requiring phosphorylation by viral kinase.
- Active against all herpesviruses, including acyclovir-resistant and ganciclovir-resistant strains.
- Used for CMV retinitis and acyclovir-resistant HSV/VZV in immunocompromised patients.
- Key toxicity: nephrotoxicity (most common), electrolyte disturbances (hypocalcemia, hypomagnesemia, hypophosphatemia), genital ulcers.
E. Cidofovir
- Nucleotide analogue (contains phosphonate group) - does not require viral kinase for initial phosphorylation, bypassing TK-based resistance.
- Active against CMV, acyclovir-resistant HSV, adenovirus, poxviruses.
- Severe nephrotoxicity - must be given with probenecid and IV saline pre-hydration to reduce tubular toxicity.
- Long intracellular half-life allows weekly/biweekly dosing.
F. Maribavir (newer)
- Benzimidazole that inhibits the CMV UL97 protein kinase, blocking viral replication and egress of viral particles from the nucleus.
- Approved for posttransplant CMV infection/disease refractory to ganciclovir, cidofovir, or foscarnet.
- Important: antagonizes ganciclovir (both target UL97) - do not co-administer.
- Side effect: taste disturbance (dysgeusia) is most common.
2. Anti-Influenza Drugs
A. Neuraminidase Inhibitors
Mechanism: Influenza virus neuraminidase cleaves sialic acid residues on host cell surfaces, which is required for release of new viral particles from infected cells and spread to neighboring cells. Neuraminidase inhibitors block this cleavage, trapping virions on the cell surface.
| Drug | Route | Key Points |
|---|---|---|
| Oseltamivir (Tamiflu) | Oral | Prodrug, activated by esterases in liver/GI tract/blood; approved for treatment (within 48 h of symptoms) and prophylaxis of influenza A and B; dose adjust in renal failure; resistance reported (~15% in children, ~1% adults) |
| Zanamivir (Relenza) | Inhaled | Active drug (not prodrug); can cause bronchospasm - avoid in asthma/COPD |
| Peramivir (Rapivab) | IV | Single-dose 600 mg; for hospitalized/severe cases |
Side effects (oseltamivir): Nausea, vomiting, abdominal pain; possible CNS effects in children (unclear if drug vs. disease).
- Harrison's 22E, Table 196-3
B. Baloxavir Marboxil (newer)
- Cap-dependent endonuclease inhibitor - targets the PA subunit of influenza RNA polymerase, blocking viral mRNA transcription ("cap-snatching" mechanism).
- Active against influenza A and B; single oral dose; active against oseltamivir-resistant strains.
- Dose: 40 mg once (80 mg if >80 kg).
C. Adamantanes (M2 Ion Channel Blockers)
- Amantadine and Rimantadine block the M2 ion channel of influenza A, preventing viral uncoating after endocytosis.
- Only active against influenza A (influenza B has no M2 protein).
- Largely obsolete: most circulating influenza A strains are resistant; use only if confirmed sensitivity.
- Amantadine side effects: CNS (insomnia, confusion, hallucinations - especially in elderly), anticholinergic.
3. Anti-Hepatitis Drugs
Hepatitis B (HBV)
| Drug | Class | Mechanism |
|---|---|---|
| Tenofovir (TDF/TAF) | Nucleotide analogue (NRTI) | Inhibits HBV DNA polymerase (reverse transcriptase); preferred first-line |
| Entecavir | Guanosine nucleoside analogue | Inhibits HBV polymerase; high barrier to resistance |
| Lamivudine | NRTI | Inhibits HBV RT; high rate of resistance limits long-term use |
| Adefovir | Nucleotide analogue | Inhibits HBV polymerase; nephrotoxic at high doses |
| Interferon-alfa / Peginterferon-alfa | Immunomodulator | Stimulates innate immunity; finite treatment course; more side effects |
Hepatitis C (HCV)
Modern direct-acting antivirals (DAAs) have transformed HCV treatment, achieving >95% cure rates:
| Drug Class | Examples | Target |
|---|---|---|
| NS3/4A protease inhibitors | Glecaprevir, voxilaprevir, grazoprevir | HCV NS3/4A serine protease |
| NS5A inhibitors | Pibrentasvir, velpatasvir, ledipasvir | NS5A replication complex protein |
| NS5B polymerase inhibitors | Sofosbuvir (nucleotide), dasabuvir (non-nucleoside) | HCV RNA-dependent RNA polymerase |
Current standard regimens are fixed-dose combinations like sofosbuvir/velpatasvir (Epclusa) or glecaprevir/pibrentasvir (Mavyret) - pangenotypic, 8-12 weeks.
4. Antiretroviral Drugs (HIV)
HIV targets include reverse transcriptase, protease, integrase, and entry steps.
A. Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs)
Mechanism: Analogues of native nucleosides lacking a 3'-OH group. After phosphorylation by cellular enzymes (not viral kinases), the triphosphate is incorporated into viral DNA by reverse transcriptase, causing chain termination.
Key drugs: Tenofovir (TDF/TAF), emtricitabine (FTC), lamivudine (3TC), abacavir (ABC), zidovudine (AZT), didanosine (ddI), stavudine (d4T).
- Most commonly used today: tenofovir/emtricitabine (Truvada) as the NRTI backbone.
- Abacavir - requires HLA-B*5701 screening before use (hypersensitivity reaction in carriers).
- Zidovudine (AZT) - first antiretroviral; causes myelosuppression, mitochondrial toxicity.
B. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
Mechanism: Bind directly and non-competitively to a hydrophobic pocket near the active site of HIV reverse transcriptase, causing conformational change and allosteric inhibition. Do not require phosphorylation.
Key drugs: Efavirenz, nevirapine, rilpivirine, etravirine, doravirine.
- Efavirenz - CNS side effects (vivid dreams, dizziness), teratogenic (avoid in first trimester); strong CYP3A4 inducer.
- Rilpivirine - better tolerated; must be taken with a substantial meal; not for high viral loads.
- All NNRTIs have a low barrier to resistance (single K103N mutation confers broad class resistance).
C. Protease Inhibitors (PIs)
Mechanism: Inhibit the HIV aspartyl protease enzyme, which cleaves polyprotein precursors (Gag-Pol) into functional viral proteins. Without cleavage, only immature, non-infectious virions are produced.
Key drugs: Ritonavir, darunavir, atazanavir, lopinavir, fosamprenavir, tipranavir.
- Ritonavir at low dose is a potent CYP3A4 inhibitor used as a pharmacokinetic booster ("ritonavir-boosted" regimens) to increase levels of co-administered PIs.
- Side effects: gastrointestinal, lipodystrophy, dyslipidemia, insulin resistance, hepatotoxicity.
D. Integrase Strand Transfer Inhibitors (INSTIs)
Mechanism: Block the HIV integrase enzyme, preventing the insertion of viral DNA into the host cell chromosome (a required step for productive infection).
Key drugs: Dolutegravir, bictegravir, raltegravir, cabotegravir, elvitegravir.
- Dolutegravir and bictegravir - high barrier to resistance; preferred in most guidelines.
- Dolutegravir is the cornerstone of WHO-preferred first-line regimens globally (e.g., TLD = tenofovir + lamivudine + dolutegravir).
E. Entry/Fusion Inhibitors
| Drug | Mechanism |
|---|---|
| Enfuvirtide (T-20) | Fusion inhibitor - peptide that binds gp41 on HIV envelope, preventing conformational change needed for membrane fusion. Subcutaneous injection only. |
| Maraviroc | CCR5 antagonist (entry inhibitor) - blocks the CCR5 co-receptor on CD4+ T cells that CCR5-tropic HIV uses for entry. Requires tropism testing before use. |
| Ibalizumab | Monoclonal antibody against CD4; blocks post-attachment entry; used for multidrug-resistant HIV. |
5. Anti-Respiratory Virus Drugs
| Drug | Target Virus | Mechanism |
|---|---|---|
| Ribavirin | RSV, Hep C, viral hemorrhagic fevers | Nucleoside analogue; inhibits RNA-dependent RNA polymerase; also acts as mutagen increasing lethal mutation load; highly teratogenic |
| Nirsevimab / Palivizumab | RSV | Monoclonal antibody against RSV F protein; prevents/limits RSV disease in infants |
| Nirmatrelvir/ritonavir (Paxlovid) | SARS-CoV-2 | Nirmatrelvir inhibits SARS-CoV-2 3CL protease; ritonavir boosts nirmatrelvir levels |
| Remdesivir | SARS-CoV-2 | Nucleotide analogue prodrug; inhibits viral RNA-dependent RNA polymerase; IV use |
| Molnupiravir | SARS-CoV-2 | Nucleoside analogue (NHC); causes lethal mutagenesis of viral RNA |
Key Pharmacological Principles Summary
| Principle | Details |
|---|---|
| Selectivity | Targeting viral-specific enzymes (e.g., viral TK, viral protease) vs. host enzymes |
| Prodrug activation | Many antivirals are prodrugs (valacyclovir, oseltamivir, famciclovir, valganciclovir) |
| Chain termination | Nucleoside/tide analogues lacking 3'-OH terminate DNA/RNA chain elongation |
| Resistance | RNA viruses mutate faster than DNA viruses; combination therapy delays resistance |
| Latency problem | Antivirals suppress replication but do not eliminate latent virus; virus rebounds on stopping treatment |
| Combination therapy (ART) | Targeting multiple steps prevents rapid emergence of resistance in HIV |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 196 - Antiviral Chemotherapy
- Lippincott Illustrated Reviews: Pharmacology, Ch. 34 - Antiviral Drugs
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28E, Ch. 44 - Antiviral Drugs
- Goldman-Cecil Medicine, International Ed., Ch. 328 - Antivirals for Influenza
This is a shared conversation. Sign in to Orris to start your own chat.