Otitis media
Reading File
Finding Sources
Searching PubMed
"otitis media"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Searching Images
acute otitis media tympanic membrane
Reading File
I now have comprehensive information to construct a thorough answer. Let me compile the full response.
Otitis Media
Definition & Types
Otitis media (OM) refers to inflammation of the middle ear. Three main forms exist:
| Type | Key Feature |
|---|---|
| Acute Otitis Media (AOM) | Acute middle ear infection with effusion and inflammation |
| Otitis Media with Effusion (OME) | "Glue ear" — fluid without signs of acute infection |
| Chronic Otitis Media (COM) | Persistent perforation ± cholesteatoma |
Epidemiology
- Most common infection for which children visit a physician
- By age 7, 93% of children have had at least one AOM episode; 75% have had recurrent infections
- Peak incidence: 6–24 months
- Annual cost in the US: ~$2.88 billion
Pathophysiology
Primary cause is eustachian tube dysfunction — abnormal tubal compliance and delayed innervation of the tensor veli palatini muscle leads to tube collapse, impaired drainage, and negative middle ear pressure. Nasopharyngeal bacteria colonize the middle ear space through this dysfunctional tube. A viral URI typically precedes AOM.
Microbiology
| Organism | Frequency |
|---|---|
| Streptococcus pneumoniae | 25–40% |
| Haemophilus influenzae | 10–30% |
| Moraxella catarrhalis | 2–15% |
Viruses and anaerobes also contribute. S. pneumoniae resistance to penicillin (via altered penicillin-binding proteins, not β-lactamase) ranges 15–50% regionally and is higher in children in daycare or with recent antibiotic exposure.
Risk Factors
- Male sex
- Age < 2 years
- Bottle feeding in supine position
- Daycare attendance / winter season
- Parental smoking
- Pacifier use
- Allergy
- Craniofacial abnormalities (e.g., cleft palate)
- Previous AOM within 3 months
- Genetic/ethnic factors (Inuit, Native American)
Clinical Features
Symptoms: ear pain (tugging/holding/rubbing in nonverbal children), fever, irritability, otorrhea, diminished hearing, tinnitus, vertigo, vomiting, loss of appetite.
Diagnosis of AOM requires ALL of:
- Middle ear effusion (MEE) — visualized as air-fluid level, bulging drum, reduced/absent TM mobility on pneumatic otoscopy, or flat tympanogram
- Signs of inflammation — acute onset of ear pain OR intense TM erythema, moderate to severe bulging of the TM, or new-onset otorrhea not due to otitis externa
Erythema of the TM alone (without MEE) = myringitis/tympanitis, not AOM.
Bullous myringitis (bullae on TM) is a variant of AOM — treatment does not differ.
Otoscopic Appearances

From left to right: AOM (erythema, bulging, loss of landmarks), OME (translucent, fluid with air-fluid level), COM (central perforation), COM with cholesteatoma (keratin debris, destruction).
Treatment
Watchful Waiting vs. Immediate Antibiotics
Most AOM resolves spontaneously. The observation option (48–72 hours) is valid in appropriately selected patients — this is not validated in adults.
| Age | Criteria | Recommendation |
|---|---|---|
| < 6 months | Any | Immediate antibiotics |
| 6 months – 2 years | Bilateral AOM | Immediate antibiotics |
| 6 months – 2 years | Unilateral, non-severe | Observation acceptable |
| > 2 years | Severe (otalgia + fever > 39°C) | Immediate antibiotics |
| > 2 years | Non-severe, reliable follow-up | Observation acceptable |
Antibiotic Therapy
| Scenario | Drug & Dose |
|---|---|
| Low-risk (>6 yr, no recent antibiotics, afebrile, not in daycare, no otorrhea) | Amoxicillin 40–50 mg/kg/day ÷ doses × 5 days |
| High-risk (<2 yr, daycare, recent antibiotics, fever >38°C, otorrhea) | Amoxicillin 80–90 mg/kg/day ÷ doses × 10 days |
| Treatment failure (symptoms persist after 3 days) | Amoxicillin-clavulanate 80–90 mg/kg/day × 7–10 days OR Cefuroxime axetil 20–30 mg/kg/day × 7–10 days OR Ceftriaxone IM 50 mg/kg × 1–3 days |
| Penicillin allergy | Cefuroxime axetil, cefpodoxime, or ceftriaxone |
Note: Antibiotics alone do NOT relieve pain in the first 24 hours. Always add analgesics (acetaminophen or ibuprofen) for pain.
Special Situations
- Acute perforation with otorrhea: treat same as AOM without perforation; small perforations usually heal spontaneously
- Tympanostomy tube with acute otorrhea: ototopical fluoroquinolone drops (NOT aminoglycosides — these are ototoxic if TM is non-intact)
Otitis Media with Effusion (OME)
- Fluid in middle ear without signs of acute infection
- Common after AOM; may persist for weeks
- Most resolve spontaneously — monitor with tympanometry and audiometry
- Tympanostomy tubes indicated for persistent bilateral OME with hearing loss, especially in children with developmental concerns
Complications
| Complication | Notes |
|---|---|
| Tympanic membrane perforation | Usually small, heals spontaneously; keep ear dry; refer if not healed in weeks |
| Mastoiditis | Most common suppurative complication; presents with postauricular erythema/tenderness, auricle protrusion; CT if intracranial involvement suspected |
| Cholesteatoma | Keratin-filled cyst in middle ear/mastoid; destructive; requires surgical excision |
| Meningitis, brain abscess, sinus thrombosis | Rare intracranial extensions |
| Conductive hearing loss | From persistent MEE or ossicular damage |
Recurrent AOM
Defined as ≥3 episodes in 6 months or ≥4 in 12 months. Options include:
- Observation without prophylactic antibiotics (preferred)
- Tympanostomy tube insertion — reduces frequency of AOM and restores hearing in OME
Sources: Textbook of Family Medicine 9e, ch. 18; Rosen's Emergency Medicine, ch. 10
Cholesteatoma
Finding Sources
Searching Images
cholesteatoma tympanic membrane otoscopy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"cholesteatoma"[MeSH Terms] AND "surgical treatment"[MeSH Terms]
Reading File
I now have comprehensive material. Let me compile the full answer.
Cholesteatoma
Definition
A cholesteatoma is an epidermal inclusion (keratinizing squamous epithelium) entrapped within the middle ear or mastoid. The name — coined by Johannes Müller in 1838 — reflects the gross resemblance of white-yellow keratin flakes to cholesterol crystals, though cholesteatomas actually contain only a small amount of cholesterol. Cruveilhier originally called it a "pearly tumor" of the temporal bone.
It is not a true neoplasm but a destructive, expansile cyst filled with desquamated keratin debris, prone to bone erosion and infection.
Classification
| Type | Origin | Key Features |
|---|---|---|
| Primary Acquired | Retraction of pars flaccida | Most common acquired type; attic/epitympanic pocket with keratin debris |
| Secondary Acquired | Migration of keratinizing epithelium through a TM perforation | Keratinizing epithelium invades middle ear via existing perforation |
| Congenital | Retained embryonic epithelial rest | Behind intact TM; white cyst-like structure medial to TM; no prior otitis/perforation |
| EAC Cholesteatoma | External auditory canal | Rare; arises from canal skin |
Epidemiology
- Acquired cholesteatoma: 9–12.6 per 100,000 adults and 3–15 per 100,000 children annually
- Most commonly presents around age 10 in children, but can occur as early as 3–4 years with extensive disease
- Associated with cleft palate and poor Eustachian tube function
- Underdevelopment of mastoid pneumatization is an almost invariable finding — in both acquired and congenital types
Pathogenesis
Acquired Cholesteatoma — Four Major Theories
1. Retraction Pocket / Invagination Theory (most accepted)
Chronic Eustachian tube dysfunction → persistent negative middle ear pressure → progressive retraction (invagination) of the pars flaccida into Prussak's space → deepening pocket traps keratin debris → cholesteatoma.
2. Epithelial Migration Theory
Normal external auditory canal epithelium migrates centrifugally; in abnormal ears, this migration is directed inward through perforations or retraction pockets.
3. Squamous Metaplasia Theory
The simple squamous epithelium of the middle ear undergoes metaplastic transformation into keratinizing epithelium (supported by finding islands of keratinizing epithelium in OME biopsies; but no validated animal model).
4. Mucosal Traction Theory (newer)
Opposing mucosal surfaces of the medial TM and lateral ossicles propel the pars flaccida into the attic via mucociliary clearance and adhesive forces; challenged by histologic findings showing ciliated cells are rare near the ossicles and even rarer in ears with cholesteatoma.
Congenital Cholesteatoma
Arises from retained embryonic epidermoid formations (normally involute by 33 weeks' gestation) or from meatal plug cells displaced during canalization — found behind an intact TM with no history of otitis, perforation, or surgery.
Bone Erosion Mechanism
The hallmark destructive property of cholesteatoma is osteoclast-mediated bone resorption (not simple pressure necrosis — direct pressure is only 1.3–11.9 mmHg, far below the 25 mmHg capillary perfusion pressure needed for ischemic necrosis).
The sequence:
- Inflammatory cytokines (including RANKL/OPG axis) released by the cholesteatoma matrix
- RANKL activates multinucleated osteoclasts via RANK receptors on osteoclast precursors
- Osteoclasts elaborate acid phosphatase, collagenase, and cathepsin-like proteases at their ruffled border
- Enzymatic dissolution of bone — intermittent in activity, explaining variable erosion
- Endochondral bone (otic capsule) is more resistant than intramembranous bone (middle ear/mastoid)
This same inflammatory process can also damage cochlear hair cells via ototoxic substances traversing the bony cochlear wall → sensorineural hearing loss in addition to conductive.
Growth Patterns (Acquired)
Originating at the pars flaccida → Prussak's space → then extends:
- Posteriorly into epitympanic recesses (lateral to incus body)
- Inferiorly into middle ear via pouch of von Tröltsch
- Anteriorly into protympanum
- Posteriorly/inferiorly into sinus tympani and facial recess (posterior mesotympanic cholesteatoma)
Clinical Features
| Feature | Detail |
|---|---|
| Hearing loss | Conductive (ossicular erosion) ± sensorineural (cochlear damage) |
| Otorrhea | Chronic, often malodorous (anaerobic infection) |
| Otalgia | Variable |
| Asymptomatic | Some cholesteatomas found incidentally |
| Misdiagnosed as OE | Infected cholesteatoma can mimic otitis externa |
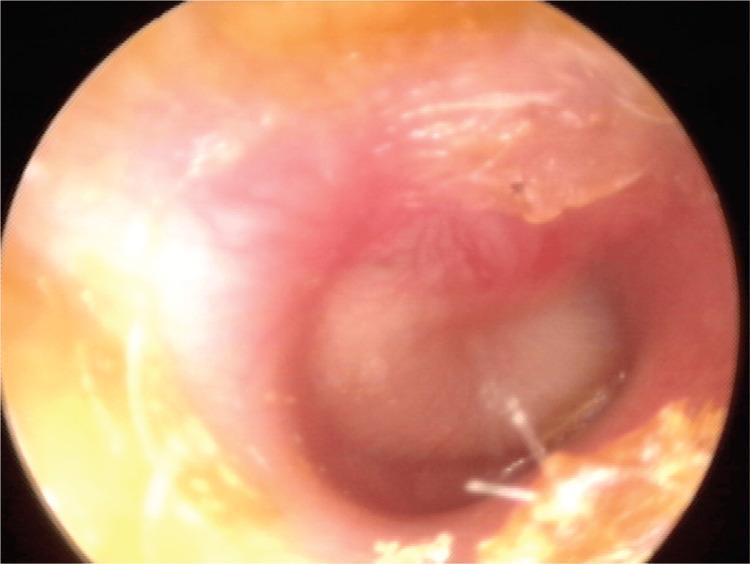
Otoscopic appearance:
- Attic retraction pocket with white keratin debris at the posterosuperior TM margin (primary acquired)
- Keratinizing epithelium visible through or around a TM perforation (secondary acquired)
- White cyst behind an intact TM — classic for congenital cholesteatoma
- Granulation tissue near eroded ear canal bone — hallmark sign
- "Aural polyp" if infected
Otoscopic / Imaging Appearances

Primary acquired cholesteatoma in the pars flaccida region with scutum erosion
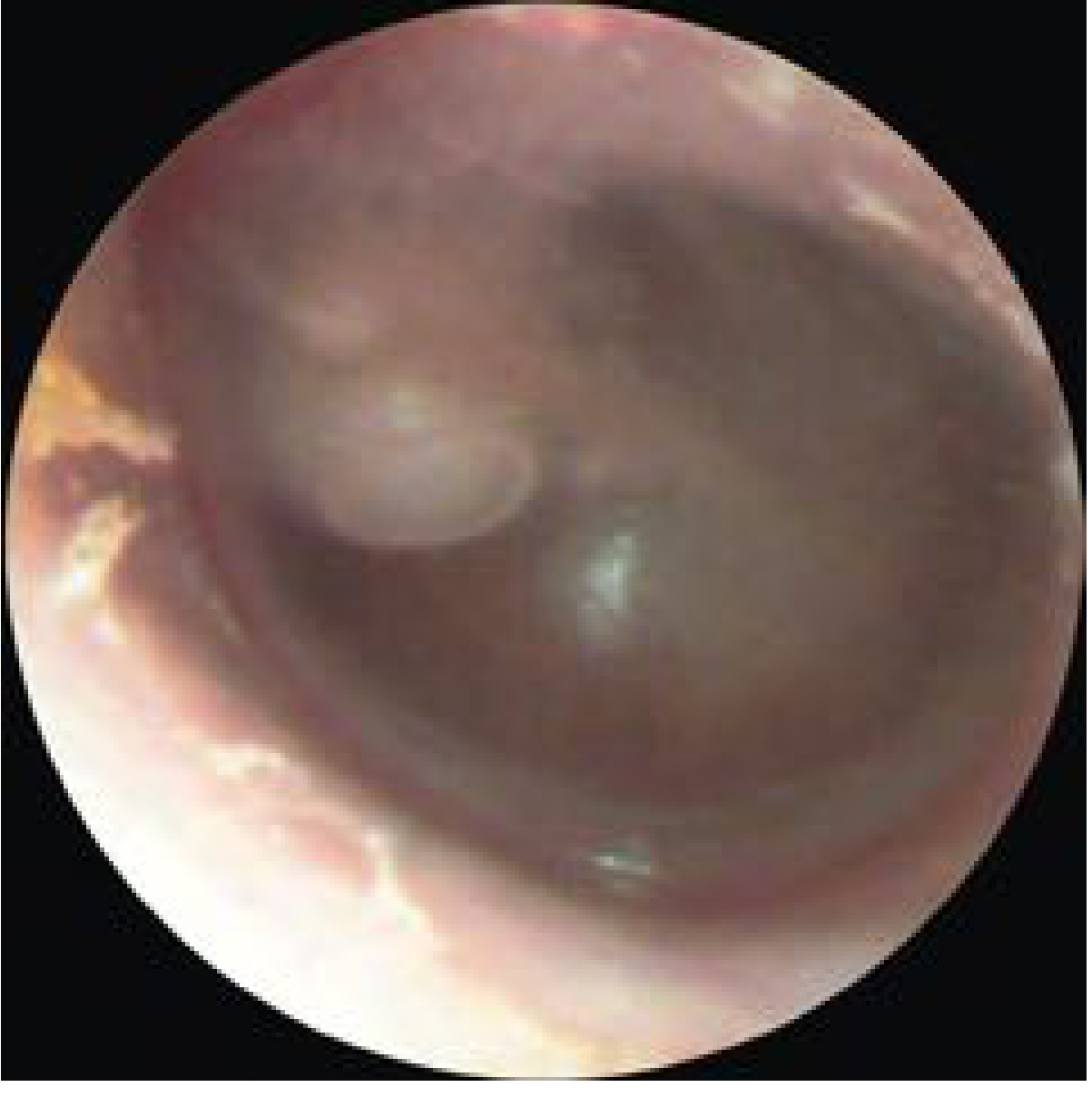
Congenital cholesteatoma — white mass visible behind an intact tympanic membrane

Complications
| Complication | Notes |
|---|---|
| Conductive hearing loss | Ossicular chain erosion (incus long process most vulnerable) |
| Sensorineural hearing loss | Ototoxic substances via labyrinthine fistula or through bony cochlear wall |
| Labyrinthine fistula | Lateral semicircular canal most commonly; causes vertigo |
| Facial nerve paralysis | Erosion of bony fallopian canal — typically the tympanic segment |
| Mastoiditis | Extension into mastoid |
| Intracranial | Meningitis, brain abscess, lateral sinus thrombosis, epidural abscess |
Diagnosis
| Modality | Role |
|---|---|
| Otoscopy / endoscopy | Primary diagnosis — retraction pocket, keratin, granulation tissue |
| High-resolution CT (HRCT) | Bony erosion, extent of disease, operative planning; scutum erosion on coronal CT and incus demineralization are key indicators. Mandatory for revision/complex surgery |
| Non-echo-planar DW-MRI | Detects cholesteatoma behind intact TM or recurrence; sensitivity/specificity ~94% — bright on DWI with low ADC. Use to reduce false-positives |
Treatment
Surgery is the only definitive treatment — there is no effective non-surgical management.
Surgical Approaches
| Approach | Description | Pros | Cons |
|---|---|---|---|
| Canal Wall Up (CWU) / Intact Canal Wall | Preserves posterior ear canal wall; mastoid exenteration through cortical mastoidectomy | Better cosmesis, no cavity maintenance, hearing aid mould fits normally | Higher recidivism; often requires second-look surgery |
| Canal Wall Down (CWD) / Modified Radical Mastoidectomy | Removes posterior canal wall; creates single cavity open to EAC | Lower recurrence; full visualization | Cavity requires lifelong regular cleaning/debridement; water avoidance; cosmetic meatoplasty issues |
| Mastoid Obliteration | Obliterates the dead mastoid space (with fat, bone, or cartilage) | Reduces cavity maintenance problems |
Meta-analyses show lower recidivism with CWD vs CWU — but CWU is often favored in children because:
- Open cavities are difficult to maintain and may require GA for debridement
- Robust regrowth of mastoid cortical bone in children can compromise cavity access
- Second-look surgery is more feasible than lifetime cavity management
Endoscopic approaches are increasingly used to improve visualization of hidden recesses (sinus tympani, facial recess) and improve completeness of disease removal.
KTP laser aids in disease removal in difficult-to-access areas.
Hearing Rehabilitation
- Ossiculoplasty performed at time of cholesteatoma removal or at second-look stage
- Bone conduction devices if ossicular reconstruction is not feasible
Key Pearls
- Malodorous otorrhea + retraction pocket + conductive hearing loss = cholesteatoma until proven otherwise
- Always debride the canal thoroughly before concluding no cholesteatoma is present — disease may be hidden during acute flares
- Otic capsule bone is more resistant to erosion than middle ear/mastoid bone
- Cholesteatoma is more aggressive when infected — infection accelerates tissue destruction
- Tympanostomy tubes are not preventative for cholesteatoma in children
Sources: Cummings Otolaryngology Head and Neck Surgery (6e), ch. 140; KJ Lee's Essential Otolaryngology; The Developing Human (Moore & Persaud), ch. 18
This is a shared conversation. Sign in to Orris to start your own chat.