Make presentation on syncope definition, pathophysiology,how it happens with detail information as well as diagnostic test and treatment and same with seizures and there co relation with each other there should be more text in the presentation with pictures according to emergency book
syncope pathophysiology vasovagal reflex mechanism
seizure classification types tonic clonic EEG brain activity
syncope vs seizure differential diagnosis comparison emergency
Make a separate presentation on status epilepticus management protocols
Presentation on syncope and seizures
Syncope and Seizure presentation prepare
Syncope Seizures Emergency Medicine
Presentation · PPTX
- Definition & Epidemiology (with baroreflex diagram)
- Pathophysiology (cerebral hypoperfusion, EEG patterns, autoregulation failure)
- Classification (Neurally Mediated / Orthostatic / Cardiac — 3-column layout)
- Clinical Features, Prodrome & Red Flags
- Diagnostic Evaluation (with syncope flowchart image)
- Treatment & Management
- Definition & Pathophysiology (excitation/inhibition imbalance, seizure propagation)
- ILAE 2017 Classification (with generalized tonic-clonic EEG image)
- Diagnostic Evaluation (with Harrison's evaluation algorithm image)
- Treatment & Emergency Management (benzodiazepines → second-line AEDs → refractory SE)
- Syncope vs Seizure — Clinical Differentiation (with differential diagnosis table)
- Full comparison table (14 features side-by-side)
- EEG differences (with ictal EEG image)
- Emergency Approach Summary & Key Takeaways
- References
In syncope what happened to afferent and efferent pathway
syncope vasovagal afferent efferent reflex arc baroreflex pathway diagram
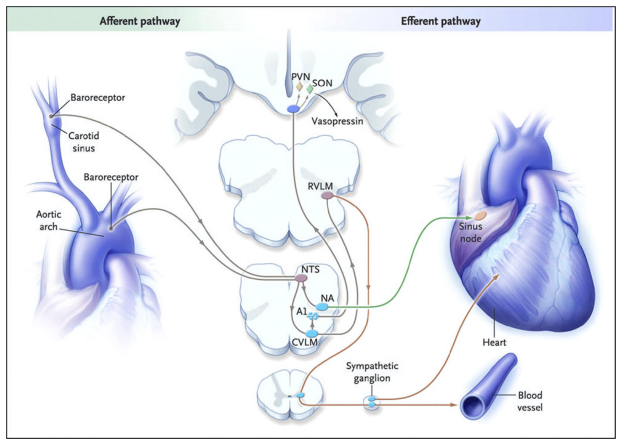
Afferent & Efferent Pathways in Syncope
The Core Concept: A Reflex Arc
1. AFFERENT PATHWAY — "The Trigger Signal Going IN"
Primary Sensors: Baroreceptors
- Location: Carotid sinus and aortic arch
- Function: Mechanoreceptors (stretch receptors) that sense changes in arterial wall pressure/stretch
- When blood pools in the legs on standing → cardiac output falls → arterial pressure falls → baroreceptors are UNLOADED (less stretch = less firing)
Signal Transmission
- Afferent signals travel via cranial nerve IX (glossopharyngeal) from the carotid sinus and cranial nerve X (vagus) from the aortic arch
- These signals are relayed to the Nucleus Tractus Solitarius (NTS) in the dorsomedial medulla — the primary baroreceptor relay center
Other Afferent Triggers (Situational Syncopes)
| Trigger | Afferent Source |
|---|---|
| Orthostatic stress | Carotid/aortic baroreceptors |
| Carotid sinus pressure | CN IX from carotid sinus |
| Cough, Valsalva | Pulmonary stretch receptors |
| Micturition, defecation | Urogenital/GI afferents |
| Pain, fear, sight of blood | Cortical/limbic → hypothalamus → NTS |
| Cardiac outflow obstruction | Cardiac mechanoreceptors (Bezold-Jarisch) |
All these different afferent pathways converge on the Central Autonomic Network (CAN) in the medulla, which integrates all inputs and coordinates the final vasodepressor-bradycardic response.
2. CENTRAL INTEGRATION — "The Control Center"
| Nucleus | Role |
|---|---|
| NTS (Nucleus Tractus Solitarius) | Primary relay — receives all baroreceptor afferent input |
| NA (Nucleus Ambiguus) | Mediates parasympathetic (vagal) output to the sinus node → bradycardia |
| CVLM (Caudal Ventrolateral Medulla) | Excitatory pathway — intermediate relay in sympathetic control |
| RVLM (Rostral Ventrolateral Medulla) | Drives sympathetic outflow to heart and blood vessels; activated by disinhibition |
| PVN/SON (Hypothalamus) | Vasopressin release via A1 noradrenergic projections from CVLM |
- NTS → ↑ RVLM activity → ↑ sympathetic tone → vasoconstriction + ↑ heart rate → blood pressure maintained
- Something causes the NTS to trigger a paradoxical response — instead of sympathetic activation, there is sudden sympathoinhibition + parasympathetic surge
3. EFFERENT PATHWAY — "The Response Going OUT"
Efferent Branch 1 — PARASYMPATHETIC (via Vagus Nerve, CN X)
- NTS → NA → Vagus nerve → SA node of heart
- Result: Bradycardia (↓ heart rate, sometimes asystole)
- This is the cardioinhibitory component of vasovagal syncope
- In extreme cases: prolonged sinus pause/asystole → sudden LOC
Efferent Branch 2 — SYMPATHETIC
- NTS → CVLM → RVLM → Sympathetic ganglia → Blood vessels
- Normal: RVLM activates sympathetic ganglia → norepinephrine release → vasoconstriction
- In vasovagal syncope: sympathetic WITHDRAWAL (sympathoinhibition) → peripheral vasodilation
- Result: Vasodepression (↓ systemic vascular resistance, blood pools in periphery)
Three Efferent Subtypes Based on Which Branch Dominates:
| Subtype | Efferent Predominance | What Happens |
|---|---|---|
| Cardioinhibitory | Parasympathetic ↑ | Severe bradycardia or asystole; BP falls secondary |
| Vasodepressor | Sympathetic withdrawal | Peripheral vasodilation; HR may be normal; BP falls |
| Mixed | Both simultaneously | Both bradycardia AND vasodilation — most common type |
4. THE FINAL COMMON PATHWAY
↓ Cardiac Output + ↓ Systemic Vascular Resistance
↓
↓ Systemic Blood Pressure (SBP <50 mmHg)
↓
↓ Cerebral Blood Flow (<25 mL/min/100g)
↓
Failure of Cerebral Autoregulation
↓
LOSS OF CONSCIOUSNESS (Syncope)
- Cessation of cerebral blood flow for just 6–8 seconds is sufficient to cause loss of consciousness
- Cerebral autoregulation normally maintains CBF constant from 50–150 mmHg perfusion pressure, but has a 5–10 second latency — rapid BP drops bypass this protection
5. WHAT FAILS IN DIFFERENT TYPES
| Type of Syncope | Afferent Problem | Efferent Problem |
|---|---|---|
| Vasovagal | Paradoxical afferent activation (e.g., vigorous cardiac contractions in underfilled ventricle → Bezold-Jarisch) | Sudden sympathoinhibition + vagal surge |
| Orthostatic hypotension | Baroreceptors fire normally — afferent is intact | Efferent sympathetic fails chronically (autonomic neuropathy) |
| Carotid sinus syndrome | Carotid sinus hypersensitive → excessive afferent signal | Normal efferent → exaggerated bradycardia/vasodilation |
| Cough/micturition syncope | Afferent trigger from pulmonary/GI/GU systems → NTS | Same efferent vasodepressor-bradycardic response |
| Cardiac syncope (arrhythmia) | Afferent system is bypassed entirely | No reflex arc — direct ↓ cardiac output causes hypoperfusion |
Summary
- Afferent pathway: Baroreceptors (carotid sinus, aortic arch) → CN IX/X → NTS in medulla. Detects the hemodynamic stress and converges from multiple peripheral triggers into the central autonomic network.
- Efferent pathway: NTS → NA (vagal/parasympathetic → bradycardia) + NTS → CVLM → RVLM → sympathetic ganglia → blood vessels (normally vasoconstriction; in syncope this is WITHDRAWN causing vasodilation).
- In neurally mediated syncope, the efferent response is paradoxically reversed: instead of compensating for low BP, the nervous system causes further bradycardia + vasodilation → catastrophic BP fall → syncope.