Write a note on liquid oxygen . For md anaesthesia exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive information to write a detailed, exam-oriented note on liquid oxygen for MD Anaesthesia. Here it is:
Liquid Oxygen (LOx) - A Note for MD Anaesthesia
Definition
Liquid oxygen (LOx) is oxygen that has been cooled and compressed below its boiling point of -183°C (-297°F) so that it exists in the liquid state. It serves as the primary bulk oxygen supply source in most large hospitals and is the standard for industrial-scale medical oxygen delivery.
Physical and Chemical Properties
| Property | Value |
|---|---|
| Molecular formula | O₂ |
| Boiling point | -183°C (90 K) |
| Critical temperature | -119°C |
| Critical pressure | 50.1 atm |
| Colour | Pale blue |
| Odour | Odourless |
| Density (liquid) | ~1.14 kg/L |
| Expansion ratio | 1 litre LOx → ~840 litres of gaseous O₂ |
Critical temperature (-119°C): This is the temperature below which oxygen can be liquefied by pressure alone. Above this temperature, no amount of pressure will liquefy oxygen. Therefore, LOx must be stored well below -119°C in insulated cryogenic containers. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Why Liquid Rather Than Compressed Gas?
- Space efficiency: 1 litre of LOx produces ~840 litres of gaseous O₂ - far more compact than high-pressure cylinders
- Economics: More economical for large hospitals (lower cost per unit volume of oxygen delivered)
- Lower storage pressure: Stored at relatively low pressure compared to compressed gas cylinders (~2200 psig for E-cylinders)
- Fewer refills required: Bulk LOx tanks are refilled by tanker trucks on-site, reducing logistics burden
- Weight advantage: In portable systems (domiciliary), LOx reservoirs weigh less than equivalent compressed gas cylinders for the same oxygen content
Hospital Bulk LOx Supply System
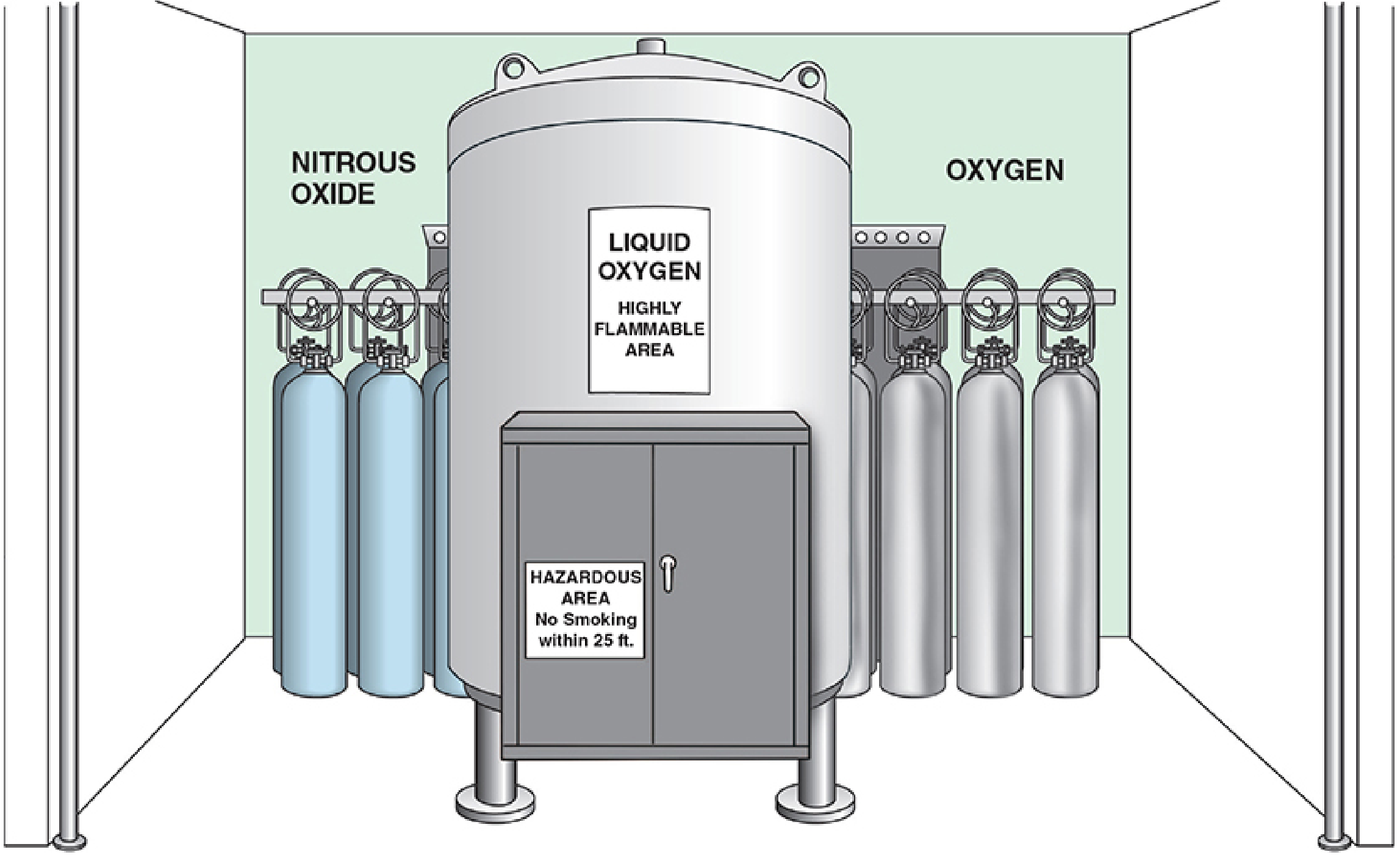
Liquid oxygen central storage tank flanked by backup H-cylinders - Morgan & Mikhail's Clinical Anesthesiology, 7e
Components:
-
Cryogenic bulk storage tank (Dewar vessel)
- Double-walled construction with vacuum insulation between inner and outer walls (similar to a Thermos flask)
- Maintains LOx at approximately -183°C
- Typical hospital tanks hold thousands of litres of LOx
- Refilled on-site from a tanker truck
-
Vaporizer/heat exchanger
- Converts liquid oxygen to gas before it enters the pipeline
- Usually an ambient-temperature vaporizer (coiled tubing exposed to outside air)
-
Pressure regulators
- Reduce gas pressure to pipeline working pressure (~50 psig / 3.4 bar)
-
Backup supply
- A smaller reserve LOx tank or bank of H-cylinders connected by manifold
- Designed to provide 24 hours of oxygen requirements
- Switches automatically if main supply fails
-
Alarm systems
- Low-pressure alarms
- Low-level alarms
The main supply source of oxygen in a large hospital usually is a cryogenic bulk oxygen storage system, refilled on site from a truck carrying liquid oxygen. Oxygen storage systems must have backup supply and alarm systems in place. - Miller's Anesthesia, 10e
Pipeline Delivery to the Operating Room
- LOx is vaporised and delivered through hospital pipeline at 50 psig (3.4 bar)
- Pipeline terminates at the operating room via DISS (Diameter Index Safety System) connectors - gas-specific and non-interchangeable
- The anaesthesia machine connects to this pipeline; a check valve prevents back-flow
- Colour coding: Green (USA) / White (International) for oxygen pipeline
Dewar Flask (Storage Vessel)
Named after Sir James Dewar, the Dewar consists of:
- Inner container (holds LOx)
- Outer container
- Interposed vacuum insulation layer
- Pressure-relief venting mechanism (mandatory - as LOx vaporises continuously, pressure rises)
Small portable dewars (5-10 lb) are used in domiciliary LOx systems, refilled from a larger stationary reservoir (up to 100 lb capacity). - Fishman's Pulmonary Diseases and Disorders
Safety Considerations (High Yield for Exams)
Fire and Explosion Risk
- Oxygen is a powerful oxidiser - it does not burn itself but vigorously supports and accelerates combustion
- Any material that burns in air burns far more intensely in an oxygen-enriched atmosphere
- No smoking permitted within 25 feet of LOx storage
- LOx must be stored away from combustible materials and ignition sources
Cryogenic Burns/Frostbite
- Contact with LOx causes immediate cryogenic tissue injury (frostbite)
- Skin contact can cause freeze burns similar to dry ice
Explosion risk from spills
- A spill of LOx rapidly vaporises, creating an oxygen-enriched atmosphere that can cause ignition of normally non-flammable materials
Pipeline failure scenario
- In 2002, a faulty joint ruptured at the bottom of a cryogenic oxygen storage tank, releasing 8,000 gallons of LOx and compromising oxygen delivery to an entire medical centre. - Barash Clinical Anesthesia, 9e
- Anaesthesiologist's response to pipeline O₂ failure:
- Immediately turn on the backup E-cylinder on the anaesthesia machine
- Disconnect the pipeline supply (mandatory - because the machine preferentially uses the higher-pressure pipeline supply even if it contains the wrong gas or has failed)
Pressure-relief venting
- LOx continuously vaporises even with perfect insulation (Leidenfrost effect)
- Pressure-relief valves are mandatory - if venting is blocked, the vessel can explode
- Stored tanks must be vented outdoors
Comparison: LOx vs. Compressed Gas Cylinders
| Feature | Liquid Oxygen (LOx) | Compressed Gas (E/H Cylinder) |
|---|---|---|
| Storage pressure | Low (~1-3 atm) | High (1800-2200 psig) |
| Storage temperature | -183°C | Room temperature |
| Space efficiency | Very high (1:840 ratio) | Lower |
| Portability | Portable dewars available | E-cylinder portable |
| Cost for large volume | More economical | More expensive |
| Risk | Cryogenic, fire/oxidiser | Explosion at high pressure |
| Pressure gauge useful? | No (pressure doesn't reflect volume) | Yes (linear relationship) |
Note: Like nitrous oxide in cylinders, the pressure gauge does not accurately reflect the remaining liquid oxygen volume until all liquid has vaporised. Volume must be assessed by weighing the tank.
Oxygen Cylinder vs LOx: Key Facts to Remember
- E-cylinder: 625-700 L of O₂ at 1800-2200 psig; pressure falls proportionally as gas is used
- A full E-cylinder at 2000 psig = ~660 L; at 1000 psig ≈ half full ≈ 330 L; at 3 L/min flow, lasts ~110 min when half-full
- H-cylinder: 6000-8000 L of O₂
- LOx bulk tank: equivalent of many H-cylinders, refilled by truck
Anaesthesia-Specific Pearls
- Always have a backup E-cylinder of oxygen available during every anaesthetic - even with bulk LOx pipeline supply, which can fail
- The anaesthesia machine has a fail-safe valve (oxygen failure cutoff valve) that shuts off nitrous oxide if O₂ supply pressure drops - protects against hypoxic mixture delivery
- Pipeline crossover (wrong gas in O₂ pipeline) is a rare but life-threatening hazard; an in-line oxygen analyser is the last line of defence
- DISS connectors and Pin Index Safety System (PISS) are engineering safeguards against incorrect gas connections - but are not foolproof; always read tank labels
- LOx is stored outside the hospital; the gas travels through an extensive pipeline, making it vulnerable to pipeline leaks, crossovers, and pressure drops
Summary Box (Exam Quick Revision)
- LOx = oxygen stored below -183°C in cryogenic Dewar vessels
- Critical temperature = -119°C (must store below this)
- Expansion ratio = 1:840 (1L liquid gives 840L gas)
- Pale blue in colour
- Hospital use: bulk cryogenic tank → vaporiser → pipeline (50 psig) → DISS connectors → anaesthesia machine
- Safety: fire/oxidiser risk, cryogenic burns, pressure-relief venting mandatory
- Backup: always have E-cylinder on anaesthesia machine
- Failure response: turn on cylinder, then disconnect pipeline
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e | Miller's Anesthesia 10e | Barash Clinical Anesthesia 9e | Fishman's Pulmonary Diseases and Disorders
Oxygen concentrators and their Uses. Co.plications of hyperbaric oxygen. Oxygen toxicity . For md anaesthesia exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full exam note.
OXYGEN CONCENTRATORS, HYPERBARIC OXYGEN COMPLICATIONS & OXYGEN TOXICITY
Notes for MD Anaesthesia Examination
PART 1: OXYGEN CONCENTRATORS
Definition
An oxygen concentrator is a medical device that concentrates oxygen from ambient air by removing nitrogen, delivering oxygen at higher-than-atmospheric concentrations without requiring refilling or replacement of cylinders or liquid oxygen systems.
Principle of Operation
Pressure Swing Adsorption (PSA) using zeolite molecular sieves:
- Compression: An electric compressor draws in ambient air and compresses it
- Heat exchange: Compressed air (heated by compression) passes through a heat exchanger to cool it
- Molecular sieve beds: Air is passed through beds of zeolite crystals - granular particles that selectively adsorb nitrogen (and argon) based on their molecular properties, allowing oxygen to pass through
- Cycling: Two sieve beds cycle alternately - while one is adsorbing nitrogen, the other is regenerating (by venting trapped nitrogen as waste)
- Product tank: Concentrated oxygen collects in a reservoir tank, pressurised to ~10 psi, filtered through a bacteria filter, then delivered to the patient via a flow meter
Oxygen concentrators use a technique called pressure swing adsorption and zeolite crystals to extract nitrogen from the air to produce oxygen. - Miller's Anesthesia, 10e
Oxygen Purity (Output Concentration)
| Flow Rate | Typical O₂ Purity |
|---|---|
| 2 L/min | 95-97% |
| 3-5 L/min | 86-93% |
| > 5 L/min (large concentrators) | Further drop |
| High flow rates (resource-limited) | May drop to ~85% |
- Pure oxygen cylinders deliver 100% O₂ at any flow rate up to 6 L/min
- Only 2 of 8 concentrators in one performance study delivered >82% O₂ at 35°C and 50% relative humidity (Miller's)
- Output purity is NOT the same as piped hospital oxygen (100%) - this has anaesthetic implications
Types
1. Stationary/Large Concentrators
- Weigh ~35 lb (16 kg)
- Deliver up to 10 L/min
- Require humidification at high flow rates
- Tethered to power source
- Used in home oxygen therapy, wards, PACU in resource-limited settings
2. Portable Concentrators
- Weigh 5-10 lb (2.3-4.5 kg)
- Battery life ~2.5 hours
- Max flow typically ≤5 L/min
- Approved by FAA for use on aircraft
- Used for ambulatory oxygen therapy
Delivery Pressure Limitation (Critical for Anaesthesia)
- Most portable concentrators deliver oxygen at pressures far less than 3.4 bar (50 psi)
- Pipeline oxygen is delivered at 50 psi
- Therefore, oxygen concentrators cannot drive:
- Ventilators without a built-in turbine or compressor
- Anaesthesia machines that require pipeline pressure
- Most pneumatically driven devices
- They can supply supplemental oxygen in:
- Operating theatre (via drawover anaesthesia system)
- PACU
- Ward
- Higher flow rates can be achieved by combining multiple concentrators in parallel
Uses of Oxygen Concentrators
Clinical Uses
| Setting | Application |
|---|---|
| Home oxygen therapy | LTOT for COPD (>15 h/day), ILD, chronic hypoxia |
| Hospital wards | Supplemental O₂ therapy, especially in resource-limited settings |
| PACU/recovery rooms | Post-operative oxygen supplementation |
| Drawover anaesthesia | Supplemental O₂ in resource-limited operating theatres |
| Paediatric wards | Low-flow O₂ in developing nations |
| Air travel | FAA-approved portable units for passengers with chronic lung disease |
| Ambulatory patients | COPD, pulmonary fibrosis on LTOT requiring mobility |
Specific Indications (LTOT Guidelines)
- PaO₂ ≤55 mmHg OR SpO₂ ≤88% at rest on room air
- PaO₂ 56-59 mmHg with cor pulmonale or polycythaemia
- Minimum prescription: 15 hours/day
- Target: Resting SpO₂ >90%
- Starting flow rate: 2 L/min (titrated)
Advantages
- No cylinders to refill - works as long as electricity is available
- Cost-effective for long-term use
- Compact and convenient for home use
- No high-pressure storage hazard
- Continuous supply (no "running out" as with cylinders)
Limitations
- Requires electricity - failure during power cuts (need backup cylinders)
- Purity drops at high flow rates
- Insufficient pressure to drive most ventilators/anaesthesia machines
- Not suitable for driving flow-dependent or pressure-dependent equipment
- Performance degrades in high temperatures and high humidity
- Require regular maintenance (filters, valves, compressors)
- Not all models conform to WHO guidelines
PART 2: HYPERBARIC OXYGEN (HBO) THERAPY AND ITS COMPLICATIONS
Definition
HBO therapy (HBOT) delivers 100% oxygen at pressures exceeding ambient atmospheric pressure (>1 ATA / >760 mmHg). This dramatically increases oxygen partial pressure and dissolved oxygen in plasma.
At sea level: PaO₂ breathing air ≈ 100 mmHg; breathing 100% O₂ at 3 ATA ≈ 2000+ mmHg
Types of Hyperbaric Chambers
Monoplace Chamber
- Accommodates one patient (or one tender + small child)
- Walls of Plexiglas - allows visual observation
- Compressed with 100% oxygen (chamber atmosphere is pure O₂)
- Limit: 3 ATA maximum
- Advantages: Lower cost, easier installation, can connect to hospital O₂ supply
- Limitations:
- Patient not directly accessible
- Emergency airway management impossible during treatment
- Pneumothorax cannot be decompressed until chamber decompresses (potentially fatal tension pneumothorax)
- Psychological aversion to confinement
Multiplace Chamber
- Accommodates multiple patients + medical staff (up to 12+ patients)
- Compressed with air; patients breathe 100% O₂ via mask, hood, or ETT
- Allows direct access to patients by nursing/medical personnel
- Monitoring and resuscitative procedures are straightforward
- More expensive, requires significant space
- Medical staff inside incur a decompression obligation (limiting treatment time)
Established Indications for HBOT
(High Yield List)
| Category | Condition |
|---|---|
| Diving/Pressure | Decompression sickness ("the bends"), Arterial gas embolism |
| Infections | Clostridial myonecrosis (gas gangrene), Necrotising fasciitis, Refractory osteomyelitis |
| CO Poisoning | Carbon monoxide poisoning (esp. with neurologic impairment or cardiac involvement) |
| Wounds | Diabetic foot ulcers, Compromised skin grafts/flaps, Radionecrosis (osteoradionecrosis) |
| Vascular | Central retinal artery/vein occlusion (within 24 hours) |
| ENT | Idiopathic sudden sensorineural hearing loss |
| Anaerobic infections | Various anaerobic bacterial infections |
HBOT Indications for CO Poisoning Specifically:
- Loss of consciousness (even transient)
- Neurologic impairment (dizziness, confusion, headache)
- Cardiac abnormalities (ischaemia, arrhythmias, ventricular failure)
- Metabolic acidosis
- HbCO >25%
- Pregnancy with fetal distress
- Protocol: 2.8-3 ATA for 1-3 treatments or until clinically stable
COMPLICATIONS OF HYPERBARIC OXYGEN THERAPY
1. Oxygen Toxicity (CNS - Paul Bert Effect)
- Occurs when O₂ partial pressure exceeds 1.4-1.6 ATA
- Symptoms: Visual disturbances, tinnitus, nausea, facial twitching, grand mal seizure (most feared)
- Seizures can be fatal if patient is underwater (drowning risk in divers)
- Precipitants: Hyperthermia, CO₂ retention, exertion, hyperthyroidism
- Management: Air breaks (5-min air-breathing intervals), reduce O₂ partial pressure
2. Pulmonary Oxygen Toxicity (Lorrain Smith Effect)
- Occurs with prolonged high O₂ exposure
- Early: Tracheobronchitis - substernal burning chest pain, cough, tightness
- Progressive: Decreased vital capacity, decreased lung compliance
- Severe: ARDS-like picture
- Risk thresholds:
- Onset after 12-16 h at 1 ATA
- Onset after 8-14 h at 1.5 ATA
- Onset after 3-6 h at 2 ATA
- Mitigation: "Air breaks" - 5-minute periods of air breathing interspersed during treatment to slow rate of pulmonary toxicity development
3. Ear and Sinus Barotrauma (Middle Ear/Sinus Squeeze)
- Most common complication of HBOT
- Caused by failure to equilibrate middle ear/sinus pressure during compression or decompression
- Presents as ear pain, fullness, hearing loss, tympanic membrane rupture
- Prevention: Valsalva manoeuvre, slow compression rate
- Contraindication: Recent ear surgery, perforated tympanic membrane (relative)
4. Dental Barotrauma (Barodontalgia)
- Pain in teeth with air-containing cavities during pressure changes
- Related to poorly restored cavities or recent dental work
5. Pulmonary Barotrauma
- Rare but life-threatening
- Gas trapping (e.g., emphysema, asthma, COPD) can lead to pneumothorax or tension pneumothorax during decompression
- In monoplace chambers: Tension pneumothorax cannot be treated until chamber decompresses - potentially fatal
- Requires chest drain insertion before treatment if significant bullous disease
6. Decompression Obligation for Attendants
- In multiplace chambers, medical staff breathing air at high pressure dissolve nitrogen into their tissues
- Must decompress slowly on exit - limits their ability to accompany critically ill patients for prolonged treatments
7. Fire/Explosion Risk
- 100% oxygen atmosphere in monoplace chambers is highly flammable
- Strict protocols: No petroleum products, no synthetic fibres, no electronic devices inside
- All equipment must be HBOT-compatible
8. Claustrophobia/Psychological Distress
- Confinement in the chamber causes distress in susceptible patients
- Limits treatment time in monoplace chambers
9. Visual Changes (Myopia)
- Transient myopia occurs with prolonged courses of HBOT
- Generally reverses within weeks of treatment cessation
- Mechanism: Lens changes from O₂-induced protein oxidation
10. Hypoglycaemia
- HBOT can precipitate hypoglycaemia in diabetic patients
- Blood glucose must be monitored before and after each session
11. Confinement/Isolation Issues
- Boredom, anxiety, and patient isolation are practical limiting factors for treatment schedules
- Particularly problematic for repeated or prolonged treatments
PART 3: OXYGEN TOXICITY
Historical Note
- 1775: Joseph Priestley (discoverer of oxygen) wrote that oxygen "might not be so proper for us in the usual healthy state of the body"
- 1899: J. Lorrain Smith first systematically described pulmonary O₂ toxicity in animals
Mechanism: Free Radical Injury
At normal FiO₂, mitochondrial metabolism generates reactive oxygen species (ROS) but cellular antioxidant defences are adequate. At high O₂ partial pressures, ROS production overwhelms defences:
Reactive Species Generated:
- Superoxide anion (O₂⁻)
- Hydrogen peroxide (H₂O₂)
- Hydroxyl radical (OH•) - most reactive
- Singlet oxygen (¹O₂)
Cellular Damage:
- Lipid peroxidation → membrane dysfunction
- Protein oxidation → enzyme failure
- DNA/nucleic acid damage → mutagenesis, cell death
Antioxidant Defences (overwhelmed in hyperoxia):
| Enzyme/Factor | Action |
|---|---|
| Superoxide dismutase (SOD) | O₂⁻ → H₂O₂ |
| Catalase | H₂O₂ → H₂O + O₂ |
| Glutathione peroxidase | H₂O₂ + lipid peroxides → H₂O |
| Glutathione reductase | Regenerates glutathione |
| Vitamin E (α-tocopherol) | Lipid antioxidant |
| Vitamin C (ascorbate) | Water-soluble antioxidant |
A vast body of evidence supports that O₂ toxicity is caused by the excessive production of oxygen-free radicals. At high O₂ partial pressures, scavenging mechanisms can be overcome by increased rates of free radical production. - Miller's Anesthesia, 10e
Pulmonary Oxygen Toxicity (Most Relevant Clinically)
Timing
- Subtle pulmonary function changes: 8-12 hours of 100% O₂
- Increased capillary permeability and decreased pulmonary function: after 18 hours
- Serious injury: Requires much longer exposure
- FiO₂ < 0.5 (50%): Generally considered safe long-term
- 100% O₂ for 10-20 hours: Generally considered safe
- FiO₂ > 50-60% for prolonged periods: Undesirable, risk of toxicity
Pathological Phases
Phase 1 - Exudative Phase (3-4 days after hyperoxic exposure):
- Death of alveolar Type I pneumocytes and capillary endothelial cells
- Interstitial oedema
- Exudative alveolar filling
- Neutrophil recruitment (capillaries → interstitium → alveoli)
Phase 2 - Proliferative Phase:
- Proliferation of Type II pneumocytes (cover exposed basement membrane)
- Endothelial cell proliferation
- Fibroblast proliferation
- Recovery: Interstitial scarring, fairly normal appearing capillary endothelium and alveolar epithelium
Clinical Manifestations
- Tracheobronchitis: Substernal chest pain, cough (earliest symptom)
- Decreased vital capacity (VC)
- Decreased diffusion capacity (DLCO)
- Decreased lung compliance
- Widening A-a gradient
- Progressive ARDS picture
- In neonates: Bronchopulmonary dysplasia (BPD)
Most Clinically Relevant Concerns (Exam Focus)
- Absorption atelectasis
- Hypercapnic respiratory failure in COPD patients (loss of hypoxic drive)
- ARDS (with prolonged high FiO₂)
- Hyaline membrane disease / Bronchopulmonary dysplasia in neonates
Absorption Atelectasis
- Occurs when high FiO₂ washes out nitrogen from poorly-ventilated alveoli
- Nitrogen normally acts as a "splint" keeping alveoli open (inert, cannot diffuse into blood)
- When nitrogen is replaced by oxygen, alveolar gas is absorbed into capillary blood
- Low V/Q segments collapse → intrapulmonary shunt → worsening hypoxaemia (paradoxical)
- Mathematically: Time to alveolar collapse after airway occlusion:
- Breathing air (3 min preoxygenation): ~37 minutes
- After preoxygenation with 100% O₂: ~8.7 minutes
- Clinical application: Using 30-40% O₂ during induction (rather than 100%) reduces post-induction atelectasis
CNS Oxygen Toxicity (Hyperbaric Conditions Only)
- Occurs at PO₂ > 1.4-1.6 ATA (not seen at 1 ATA)
- Symptoms: VENTID mnemonic:
- Visual disturbances (tunnel vision)
- Ear symptoms (tinnitus)
- Nausea
- Twitching (facial/lip muscles - early warning sign)
- Irritability, anxiety
- Dizziness → Grand mal seizure (most severe)
- Precipitating factors: CO₂ retention, hyperthermia, exertion, hyperthyroidism
- Rarely occurs at clinical HBOT pressures (2-3 ATA) with air breaks
- At 1 ATA: O₂ toxicity is almost exclusively pulmonary
Retinopathy of Prematurity (ROP)
- Neovascular retinal disorder in premature infants (especially <28 weeks gestation)
- Formerly called retrolental fibroplasia
- Risk factors: High FiO₂ (historically unmonitored), low birth weight, sepsis, prematurity
- Correlates with arterial (not alveolar) O₂ tension - contrast with pulmonary toxicity
- Recommended PaO₂ in premature infants: 50-80 mmHg (SpO₂ 88-95%)
- Does not mean withholding O₂ when cardiopulmonary indications exist
Hypoventilation from Supplemental O₂ (COPD)
- COPD patients with chronic CO₂ retention develop hypoxic ventilatory drive dependency
- Correcting hypoxaemia to normal levels removes this drive → severe hypoventilation
- Additionally: High O₂ in COPD causes V/Q mismatch worsening (Haldane effect)
- Use controlled low-flow O₂ (24-28% via Venturi mask) targeting SpO₂ 88-92%
- Pulse oximetry is a poor monitor for opioid-induced hypoventilation if supplemental O₂ is running - opioid-depressed ventilation may be masked
Summary Table: Oxygen Toxicity - Quick Revision
| System | Threshold | Manifestation |
|---|---|---|
| Pulmonary | FiO₂ > 0.5 for prolonged periods; 100% O₂ > 18-24h | Tracheobronchitis → ARDS; BPD in neonates |
| CNS | PO₂ > 1.4 ATA (hyperbaric only) | VENTID symptoms → Grand mal seizure |
| Eye (ROP) | Uncontrolled high FiO₂ in premature neonates | Retinal neovascularisation → blindness |
| Atelectasis | High FiO₂ in low V/Q areas | N₂ washout → alveolar collapse → shunt |
| COPD | Any supplemental O₂ | Hypoventilation, hypercapnic crisis |
Anaesthesia-Specific Pearls (Exam Focus)
- Pre-oxygenation debate: 100% O₂ for RSI vs. lower FiO₂ to reduce atelectasis - current evidence favours FiO₂ 0.8-1.0 for denitrogenation/apnoeic oxygenation safety margin despite some atelectasis risk
- Oxygen concentrators deliver <50 psi - cannot drive standard anaesthesia machines; use only with drawover systems
- HBOT chambers during anaesthesia: Drug dosing may be altered under pressure; pharmacodynamics can change
- Neonatal anaesthesia: Target SpO₂ 88-95% in premature infants; avoid hyperoxia
- Air breaks in HBOT: 5-minute air-breathing intervals reduce both CNS and pulmonary O₂ toxicity accumulation during prolonged HBO treatment schedules
Sources: Miller's Anesthesia 10e | Morgan & Mikhail's Clinical Anesthesiology 7e | Goodman & Gilman's Pharmacological Basis of Therapeutics | Fishman's Pulmonary Diseases and Disorders | Murray & Nadel's Respiratory Medicine | Barash Clinical Anesthesia 9e
This is a shared conversation. Sign in to Orris to start your own chat.