Mode of transmission of e.histolytica
Reading File
Finding Sources
Searching the Web
Entamoeba histolytica mode of transmission cyst fecal oral route
Reading File
Reading File
Here is a complete summary of the mode of transmission of Entamoeba histolytica, compiled from authoritative medical textbooks:
Mode of Transmission of Entamoeba histolytica
Primary Route: Fecal-Oral
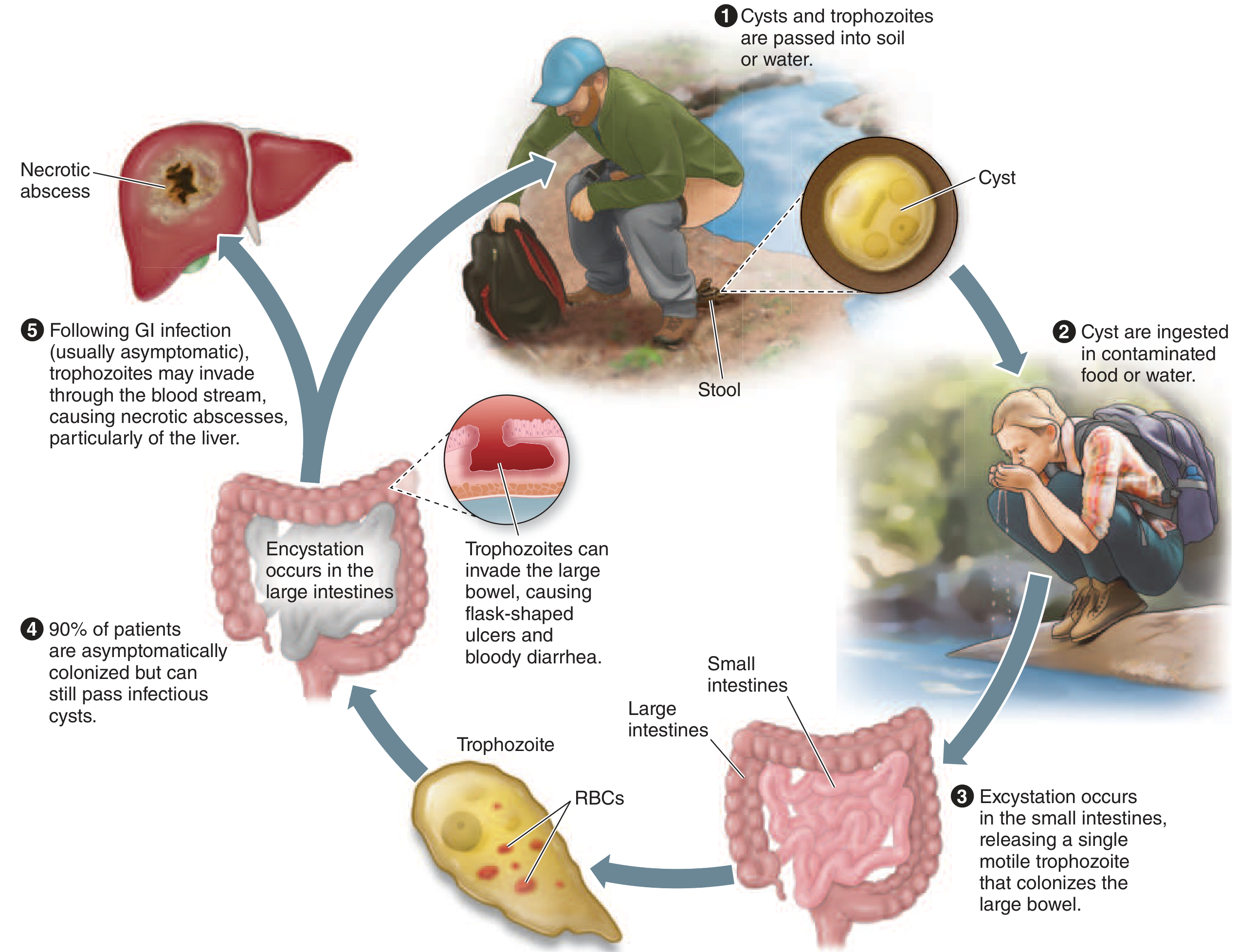
The dominant mode of transmission is fecal-oral, occurring through ingestion of food or water contaminated with the infective cyst form of the parasite. - Rosen's Emergency Medicine, p. 3200; Fishman's Pulmonary Diseases, p. 1078
Infective Form: The Mature Cyst
- Only the cyst is infective - not the trophozoite
- Cysts are quadrinucleate (4 nuclei) and are passed in the feces of infected individuals
- Cysts can survive in the external environment for weeks to months, especially in damp conditions and temperatures between -5°C and 40°C - Fishman's Pulmonary Diseases, p. 1082
- Trophozoites, by contrast, do NOT survive outside the human host and are therefore not infectious by ingestion
Specific Mechanisms of Spread
| Mechanism | Notes |
|---|---|
| Contaminated water | Most common vehicle in endemic regions |
| Contaminated food | Especially raw vegetables washed with polluted water, or handled by infected food handlers |
| Oral-anal sexual contact | Relevant in men who have sex with men (MSM) - Fishman's, p. 1078 |
| Person-to-person (direct contact) | In institutions (prisons, psychiatric facilities) with poor sanitation |
| Flies and cockroaches | Can mechanically carry cysts from feces to food (mechanical vectors) |
Life Cycle After Ingestion
- Ingested cysts pass through the stomach (acid-resistant wall protects them)
- In the small intestine, each cyst excysts and forms 8 daughter trophozoites (via metacystic division)
- Trophozoites migrate to the large intestine, where they may:
- Remain as commensals (asymptomatic in ~90% of cases)
- Invade the mucosa, causing amoebic colitis/dysentery
- Enter the portal circulation and reach the liver (amebic liver abscess)
- In the colon, trophozoites encyst again and are excreted in feces, completing the cycle - Fishman's Pulmonary Diseases, p. 1082
High-Risk Groups
- People in developing countries with poor sanitation
- Travelers to endemic regions (India, Africa, Mexico, Central/South America)
- Institutionalized individuals
- MSM (men who have sex with men)
- Immigrants from endemic areas - Rosen's Emergency Medicine, p. 3211
Key Points for Exam
- Infective stage = mature quadrinucleate cyst (ingested)
- Diagnostic stage = trophozoite or cyst (passed in stool)
- E. histolytica is classified as a Category B biodefense pathogen (CDC/NIAID) because of its low infectious dose, environmental stability, resistance to chlorine, and ease of spread through food/water contamination
- Entamoeba dispar is morphologically identical but non-pathogenic and 10x more prevalent; differentiation requires antigen, PCR, or immunologic testing - Fishman's Pulmonary Diseases, p. 1080
Pathogenicity of E. Histolytica
Finding Sources
Searching the Web
Entamoeba histolytica pathogenicity mechanisms virulence amoebapore galactose lectin
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a detailed, structured account of the pathogenicity of Entamoeba histolytica based on Harrison's (22nd Ed.) and Goldman-Cecil Medicine:
Pathogenicity of Entamoeba histolytica
Key Principle
Only trophozoites (not cysts) invade tissue. ~90% of infections remain asymptomatic - full invasive disease requires disruption of the host-parasite equilibrium. - Harrison's, p. 1797
Step-by-Step Mechanism of Pathogenicity
Step 1 - Adherence: Gal/GalNAc Lectin
- The trophozoite surface carries a galactose and N-acetyl-D-galactosamine (Gal/GalNAc)-specific lectin
- This lectin binds to carbohydrate determinants on colonic epithelial cells and mucus
- Adherence is the first and essential step - without it, no invasion occurs
- The Gal/GalNAc lectin is also directly linked to virulence: ingestion of enteropathogenic bacteria (e.g., EPEC, Shigella) increases its expression, while commensal E. coli decreases it - Harrison's, p. 2243
Step 2 - Mucus Degradation
- After attachment, trophozoites release glycosidases and proteases that degrade mucus polymers
- This strips away the protective mucous layer overlying the epithelium
- E. histolytica encodes at least 44 cysteine proteinase genes involved in:
- Degrading colonic mucin glycoproteins
- Digesting extracellular matrix components (collagen, elastin, villin)
- Digesting hemoglobin
- Inactivating IL-18 (an anti-parasitic cytokine)
- Cleaving IgA and IgG antibodies, neutralizing host defenses
- Degrading complement anaphylatoxins C3a and C5a - Goldman-Cecil, p. 3302; Harrison's, p. 2238
Step 3 - Contact-Dependent Cytotoxicity (Three Mechanisms)
Once the mucous barrier is breached, trophozoites destroy host cells by direct contact via three mechanisms:
| Mechanism | Details |
|---|---|
| Apoptosis induction | Gal/GalNAc lectin binding activates host caspase-3 within minutes; caspase-3 inhibitors block amebic killing |
| Trogocytosis | "Nibbling" - trophozoites ingest fragments of living host cells, a process called amebic trogocytosis, which leads to cell death |
| Cell lysis | Release of phospholipase A and amoebapores (pore-forming peptides) lyses neutrophils, monocytes, lymphocytes, colonic cells, and hepatic cells |
- Goldman-Cecil, p. 3302; Harrison's, p. 2240
Step 4 - Contact-Independent Cytotoxicity
- Trophozoites produce prostaglandin E2 and other inflammatory mediators
- These increase ion permeability of intercellular tight junctions, disrupting epithelial barrier integrity - Harrison's, p. 2240
Step 5 - Phagocytosis of Host Cell Corpses
- After killing cells, trophozoites phagocytose the apoptotic corpses using multiple ligands including the Gal/GalNAc lectin, a phosphatidylserine receptor, serine-rich E. histolytica protein (SREHP), and collectins
- This phagocytic step is required for colonic infection to progress - Goldman-Cecil, p. 3302
Step 6 - Invasion and Ulcer Formation
- Trophozoites penetrate the colonic mucosa, producing characteristic flask-shaped ulcers (narrow neck, broad base in submucosa)
- Ulcers may coalesce, causing hemorrhage, perforation, or toxic megacolon in severe cases
Step 7 - Evasion of Host Immunity
- Antioxidant defense: E. histolytica lacks glutathione but uses a thioredoxin-thioredoxin reductase system to resist reactive oxygen and nitrogen species (ROS/RNS) from host phagocytes - Harrison's, p. 2242
- This is also the target of metronidazole (inhibits this antioxidant system)
- Complement resistance: Cysteine proteases cleave C3a and C5a, preventing complement-mediated lysis
- Antibody degradation: IgA and IgG are proteolytically degraded
- Cathelicidin resistance: Amebic cysteine proteinases digest antimicrobial peptides produced by the host intestine
Step 8 - Hepatic (Extraintestinal) Invasion
- Trophozoites penetrate the intestinal wall and enter portal venous circulation
- Reach the liver, causing inflammation, necrosis, and formation of a hepatic "abscess" (actually a necrotic cavity, not a true pus-filled abscess)
- The right hepatic lobe is most commonly affected (due to portal blood flow patterns)
- Invasive disease is 10x more common in men than women - attributed to differences in complement-mediated killing and testosterone effects on IFN-γ secretion - Harrison's, p. 2222
Role of Gut Microbiome in Pathogenicity
The microbiome significantly modifies disease severity:
- Protective bacteria (Ruminococcaceae, Coriobacteriaceae, Clostridiaceae) are present in asymptomatic carriers but absent in invasive disease
- Pathogenic gut flora (Shigella, EPEC) upregulate Gal/GalNAc lectin expression, worsening invasive capacity
- High Prevotella copri abundance in infants correlates with diarrhea during infection - Harrison's, p. 2248
Immune Response Summary
| Component | Role |
|---|---|
| Neutrophils/Eosinophils | First responders (days 1-2); depletion worsens disease |
| Macrophages + T lymphocytes | Recruited by day 3; macrophages gain amebicidal activity via IFN-γ, TNF-α |
| Secretory IgA (intestinal) | Protective - anti-Gal/GalNAc IgA reduces reinfection risk by 64% |
| Serum IgG | NOT protective; correlates with duration, not severity of illness |
| Innate lymphoid cells type 2 | Coordinate protective type 2 immune responses |
- Goldman-Cecil, p. 3303; Harrison's, p. 2251
Summary of Virulence Factors
| Virulence Factor | Function |
|---|---|
| Gal/GalNAc lectin | Adherence to host epithelium; triggers apoptosis |
| Cysteine proteinases (44+ genes) | Degrade ECM, mucin, IgA, IgG, C3a, C5a, IL-18 |
| Amoebapores (pore-forming proteins) | Lysis of host cells and immune cells |
| Phospholipase A | Membrane disruption and cell lysis |
| Thioredoxin-reductase system | Resistance to host ROS/RNS; target of metronidazole |
| Trogocytosis | Nibbling and ingestion of living host cells |
| Prostaglandin E2 | Disrupts tight junctions (contact-independent toxicity) |
This is a shared conversation. Sign in to Orris to start your own chat.